Food allergy can be defined as “an adverse reaction to food mediated by an immunologic mechanism, involving specific IgE (IgE mediated mechanisms), cell mediated mechanisms (non-IgE mediated mechanisms) or a mixture of the two”.1 Food allergy is more common in children than adults, occurring in 5-6% of children in Ireland under the age of five. Ninety per cent of IgE reactions are caused by well known triggers – milk, egg, peanut, nuts and fish.2
IgE vs non IgE mediated reaction
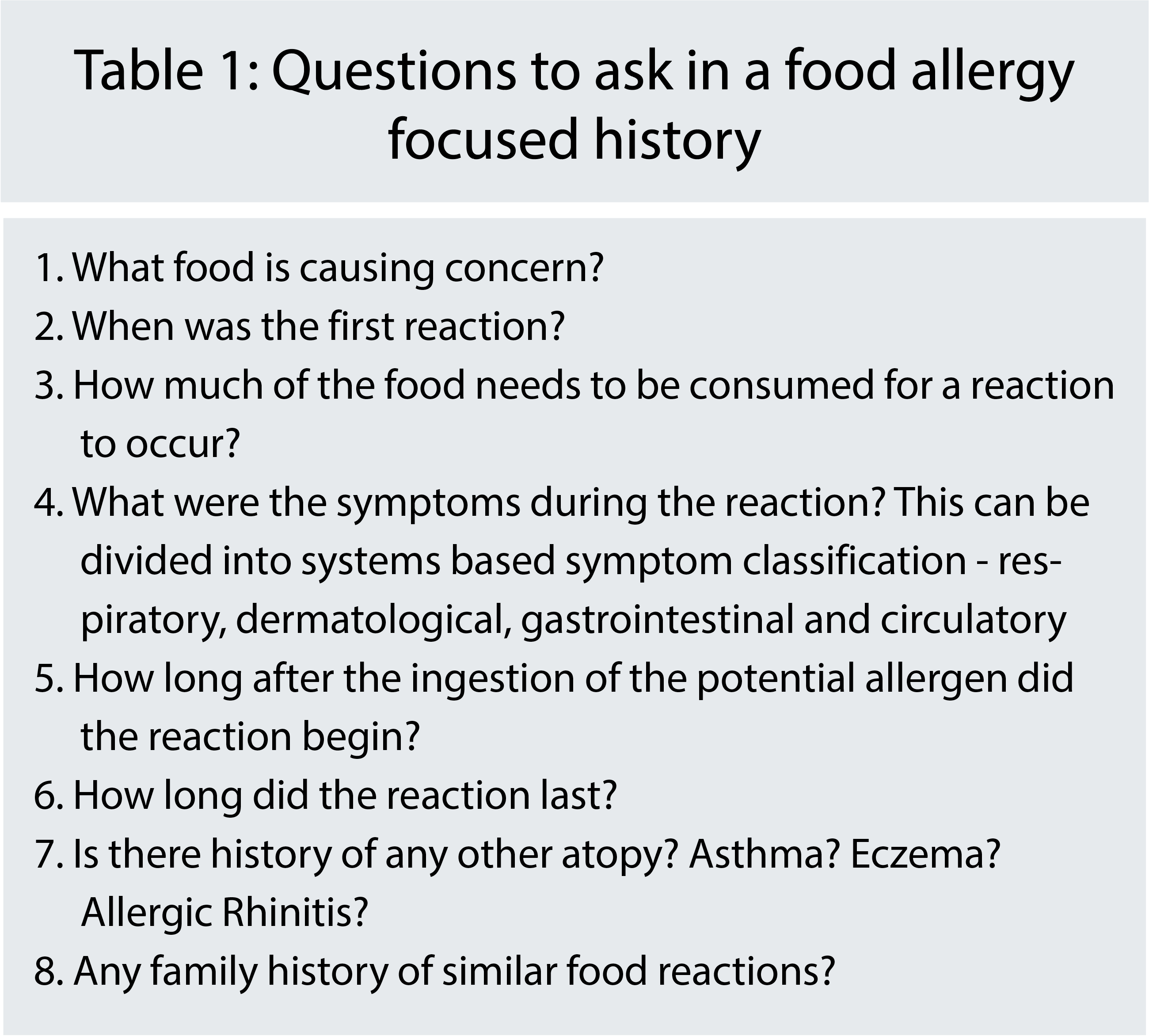
IgE and non-IgE mediated reactions can be differentiated through careful history taking. In addition to the questions in Figure One, it is important to assess how reproducible the reaction is, as food allergy is a consistent and reproducible reaction. If not reproducible, other potential diagnoses, eg. atopic dermatitis, hereditary urticarial syndromes should be considered. The prevalence of food allergies can vary between ethnic groups, and this should be noted when taking a history.
An IgE mediated reaction is an immediate, type one hypersensitivity reaction. The onset of symptoms occurs quite rapidly following the ingestion of the offending allergen – symptoms occur usually within minutes but can be delayed by up to two hours. Symptoms include urticaria, oedema of the lips, tongue and throat, nausea, vomiting and diarrhoea and wheeze, dyspnoea or cyanosis.2,3 The most important feature in the history is the timing of the onset of the reaction.
Non-IgE mediated allergy is a delayed or type 4 hypersensitivity reaction. These symptoms occur > 24 hours after exposure and affect a wide variety of organ systems. Symptoms can include pruritis, atopic eczema, loose stools, abdominal pain, constipation, pallor, and faltering growth.2,3
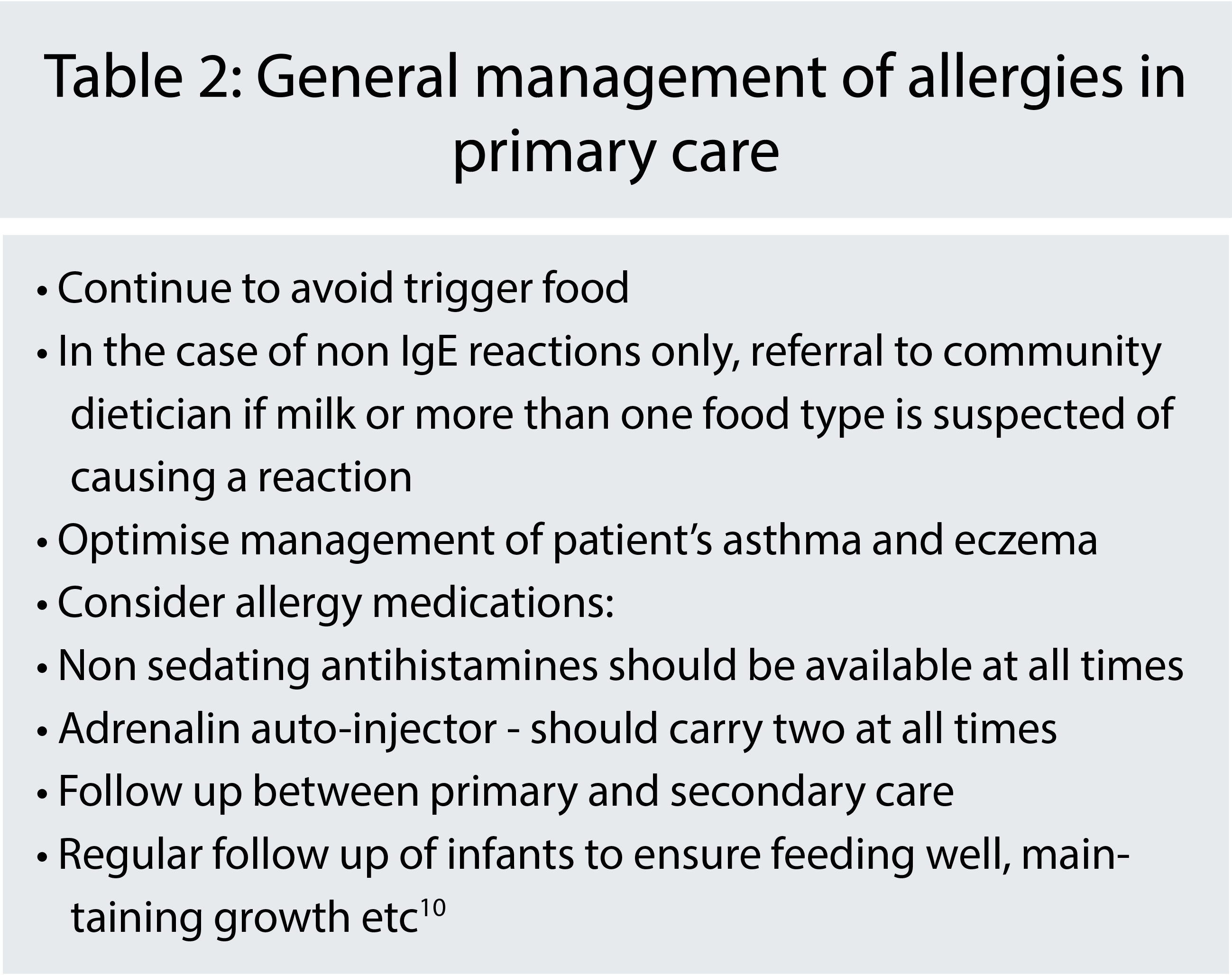
Following history and examination, children with suspected food allergy/anaphylaxis should be referred to secondary care for confirmation and appropriate management.
(click to enlarge)
(click to enlarge)
Diagnosis of allergy
Diagnosis of food allergy is sought through history of exposure and reaction. IgE mediated reactions can be assessed through specific IgE antibody levels and through skin prick testing. The availability of blood testing for specific IgE levels in general practice varies depending on the policy of the local laboratory.
For non IgE mediated reactions, the diagnosis is based on elimination of the suspected food allergen from the diet for usually four to six weeks with subsequent reintroduction of the food and monitoring of symptoms. This is usually done in combination with support from dietetics.3
Egg allergy
Egg is the most common food allergy in children.4 It is important to remind ourselves that egg allergic children can receive the MMR vaccination as part of the normal schedule in the community and do not need to attend hospital.5 The egg content of the influenza vaccine does vary yearly and guidelines should be checked before administration.6 The majority of children develop tolerance by 10 years of age.7 Ongoing monitoring with IgE specific to egg can assist in the decision to reintroduce. Reintroduction of egg occurs via the egg ladder.
Cow’s milk protein allergy (CMPA)
CMPA is the second most common food allergy affecting 2-7.5% of children under one year. Fortunately, resolution of the allergy is seen in 75-90% of children aged 5-6 years.8 Casein and whey in cow’s milk cause an immune mediated reaction leading to symptoms which can be divided, as discussed previously, into IgE and non IgE mediated. IgE mediated symptoms include – angio-oedema of oropharynx, pruritus and urticaria. Non-IgE mediated symptoms include – reflux, diarrhoea, constipation, colic and eczema. The management of CMPA involves removing CMP from the diet.9
Exclusively breastfed infants may improve with elimination of cow’s milk from the mother’s diet, which should be supplemented with calcium and vitamin D. This should be carried out under dietitian supervision.1,8
There are two kinds of formula replacements for CMPA in those under six months of age. The first line are the extensively hydrolysed formulas which have CMP degraded, eg. Aptamil Pepti, Nutramigen Lipil. Around 10% of infants will not respond to the first line replacement formulas and will need to be started on an amino acid based formula, eg. Nutramigen AA, Neocate.9 There is no role for other mammalian milks, eg. sheep or goats’ milk or lactose-free formulas in these patients . Once over six months, the use of soy milk can be considered.10
Non-IgE mediated CMPA should trial an elimination diet for four to six weeks, ideally this is supervised by a community dietician.
Elimination usually continues until the patient is approximately one year old, as 80% of children have outgrown the allergy at this age. Severity of the reaction depends on the environment in which reintroduction will occur. For children with non-IgE mediated CMPA – a trial reintroduction at home can be safely carried out unless there is a history of severe reaction – those patients should be managed in secondary care. Children with IgE mediated CMPA should be managed in secondary care with specialist knowledge of food allergy management. Reintroduction is guided by the milk ladder.8
Peanut allergy
Peanut allergy is one of the most common food allergies affecting older children with high prevalence in Western Europe.11 Unlike egg and milk allergy, it persists in 80% of cases. 85% of patients with a peanut allergy will react to the first consumption of peanut with up to 70% of these reactions being mild to moderate.
The severity of future reactions can be impossible to predict and with peanut allergy being responsible for the majority of food allergen related deaths in children, it is essential that patients carry adrenalin auto-injectors. Teenagers are particularly at risk of fatal anaphylaxis due to factors such as reduced supervision and a possible reluctance to carry auto-injectors.12
GP visits provide an opportunity to re-educate this group on allergen avoidance and auto-injector use. Correct use of the auto-injectors is vital. Local allergy clinics or paediatric units often arrange demonstrations for parents and patients. Up to date information and videos demonstrating use can also be found on product websites, eg. epipen.com. There are also apps to remind of expiry dates amongst other functions.
The mainstay of treatment is avoidance – careful review of food labels, not keeping peanuts in the household and not consuming foods without known ingredients are some of the tactics used.
Primary prevention of food allergy
The Learning Early about Peanut Allergy (LEAP) study published by Du Toit et al, examined 640 infants of at least four months of age with negative results on skin prick testing for peanuts and with a history of severe eczema, egg allergy or both.
The group was divided in two at random – to either consume or to avoid peanuts for a period of 60 months. It found that patients who were introduced earlier to peanuts were significantly less likely to develop an allergy compared to those who avoided peanuts for 60 months.14
The Enquiring About Tolerance (EAT) team published a study in 2016 that looked at 1,303 exclusively breastfed infants at three months old, dividing them into two groups: one would undergo early introduction of six potentially allergenic foods at three months of age (peanut, cooked egg, sesame, white fish, wheat and cow’s milk) and the second group which would follow standard practice of exclusively breastfeeding until six months old. The outcome assessed was development of food allergy between one to three years. There were issues with adherence during the study; however in those who adhered to the study protocol, there was a significantly lower relative risk of developing food allergy in the early intervention group. This was not statistically significant however, when data from all participants were analysed.15
The European Academy of Allergy and Clinical Immunology has recommended the following in relation to primary prevention of food allergy:
No special diet for pregnant women or breastfeeding mothers
Exclusively breastfeeding for four to six months
There is no need to avoid foods complementary to breastfeeding beyond four months and at present the “evidence does not justify recommendations about withholding or encouraging consumption of potentially allergenic foods after four months” once weaning has started16
Further studies on the benefits and safety of early introduction to allergenic foods needs to be carried out before a population wide recommendation can be made.
 (click to enlarge)
(click to enlarge)