DIABETES
Diabetes and alcohol
Alcohol use in those with diabetes and the potential risks of hypoglycaemia and how to avoid them
May 13, 2014
-
Enjoying a drink is part of Irish culture, birthdays, weddings, funerals or celebrating the start of the weekend. Irish people find many good reasons to enjoy a drink. So, is drinking alcohol off limits for people with diabetes? The happy answer to that question is no. The majority of people with diabetes can continue to enjoy drinking alcohol, but they do need to be aware of the effect that alcohol may have on their blood glucose levels in order that they can drink safely.
Diabetes mellitus
Diabetes mellitus is characterised by chronically raised blood glucose levels caused by an absolute or relative lack of the hormone insulin. In type 1 diabetes insulin is not being produced by the pancreas, it is caused by an auto-immune destruction of the insulin producing beta-cells in the pancreas. It usually presents in childhood or early adulthood and it is treated with diet, exercise and insulin injections.
In type 2 diabetes there is insufficient insulin or ‘resistance’ to the action of insulin. Family history of diabetes, being overweight and having a sedentary lifestyle are major risk factors for the development of this type of diabetes.1
Diabetes and alcohol: How much is too much
The recommended alcohol intake for people with diabetes is the same as for the general population.
- Men: No more than 17 standard drinks per week
- Women: No more than 11 standard drinks per week
- Do not consume more than five standard drinks in one sitting.
- Allow at least two alcohol free days a week
-
One standard drink =
- Half a pint of larger
- Standard pub measure of a spirit
- Small glass of wine (125ml).2
Consistently drinking alcohol to excess has been linked with high blood pressure and obesity which are risk factors for type 2 diabetes.
There is some evidence to suggest that a moderate alcohol intake may have a protective effect against the development of type 2 diabetes. Some studies show a U-shaped relationship between alcohol intake and the risk of diabetes demonstrating a higher risk of developing diabetes with both low and high intakes of alcohol and a lower risk with a moderate intake of alcohol. These protective effects require further evaluation however and the evidence is not strong enough to advocate that teetotallers take up drinking alcohol. Also the interaction between alcohol intake and other risk factors for type 2 diabetes such as body weight and family history of diabetes was not examined.3
Regular drinking increases the risk of acute and chronic pancreatitis. A total of 70% of cases of chronic pancreatitis are due to long term heavy drinking, 50% of people who have chronic pancreatitis go on to develop diabetes.4
Role of the liver in maintaining blood glucose concentration
In order to understand the potential risks associated with drinking alcohol with diabetes, it is important to have some insight into how the body maintains normal blood glucose levels and the vital role that the liver plays in this.
In the fasting state the body has two major mechanisms for maintaining blood glucose levels. The first is the breakdown of glycogen (glycogenolysis) and the second is the production of glucose or gluconeogenesis. Glycogen is stored in the tissues particularly the liver. It serves as the first line of defence against hypoglycaemia as it is broken down into glucose and is secreted by the liver into the blood to maintain normal blood glucose levels. Glycogen stores may be depleted in someone with type 1 diabetes particularly if they have repeated episodes of hypoglycaemia. Gluconeogenesis also occurs primarily in the liver and it involves the formation of glucose from non-carbohydrate sources.
As 90-95% of alcohol is metabolised in the liver it shuts down the process of gluconeogenesis and thus the bodies second line of defence against hypoglycaemia. Therefore, alcohol tends to increase the risk of hypoglycaemia by impairing hepatic glucose release.5
Hypoglycaemia
In patients with diabetes treated with insulin, alcohol has been implicated in up to one-fifth of hospital attendances with hypoglycaemia.6
Hypoglycaemia can have serious even life-threatening consequences. The brain can only utilise glucose as an energy source unlike other tissues that can switch from oxidation of glucose to non-glucose fuels. Therefore the brain is dependent on a continuous supply of glucose from the circulation to maintain its metabolism and function. If the continuous supply of glucose is interrupted for even a few minutes it can lead to central nervous system dysfunction.1 For this reason the body employs multiple mechanisms to prevent hypoglycaemia. The first response to hypoglycaemia is the release of counter-regulatory hormones and secondly the body generates a specific set of symptoms. These symptoms consist of autonomic symptoms (anxiety, palpitations, hunger, sweating, irritability and tremor) and neuroglycopenic symptoms (dizziness, tingling, blurred vision, difficulty concentrating and faintness). Counter-regulatory hormones are released at a plasma glucose threshold of 3.5mmol/l, symptoms of hypoglycaemia occur at a plasma glucose threshold of 3.0mmol/l and cognitive function deteriorates when plasma glucose falls below 2.7mmol/l.7
Who is at risk of hypoglycaemia
Not everyone with diabetes is at risk of hypoglycaemia. Hypoglycaemia is a common side-effect of all insulins and certain drugs used in the treatment of type 2 diabetes called sulphonylureas which stimulate insulin secretion. Drugs in the sulphonylurea category include Diamicron and Amaryl. Hypoglycaemia caused by sulphonylureas can be prolonged and severe. The hypoglycaemia effect of insulin and sulphonylureas can be exacerbated by the simultaneous ingestion of alcohol.1
Patients on insulin therapy and sulphonylureas should be educated by their health care professional about the potential side effects of hypoglycaemia, including causes, treatment and avoidance. They should also be advised to carry carbohydrate with them, ie. glucose sweets if they need to treat a hypoglycaemia episode when they are away from home.
Alcohol and the risk of hypoglycaemia
Alcohol may be associated with hypoglycaemia in a variety of ways:
- Alcohol consumption can cause cognitive impairment affecting a persons ability to detect the warning symptoms of hypoglycaemia. If they are under the influence of alcohol they may not take corrective action to prevent the plasma glucose falling further such as taking carbohydrate therefore will not prevent neuroglycopenia
- Alcohol has been shown to blunt the body’s hormonal counter-regulatory response to hypoglycaemia
- Third parties may mistake the symptoms of hypoglycaemia for symptoms of intoxication, which may have potential health or even legal consequences for the individual
- Alcohol can increase the risk of nocturnal hypoglycaemia or hypoglycaemia the following day by impairing hepatic glucose release.4
Other factors influencing hypoglycaemia include the person’s glycaemic control at the time, recent exercise, insulin absorption, alcohol in relation to food intake and the duration of diabetes.
Glucagon hypokit, which is used to treat severe hypoglycaemia, only works when the liver has glycogen stores. It will therefore not work to treat hypoglycaemia caused by drinking too much alcohol. It is essential that people with diabetes are aware of the risks of hypoglycaemia following alcohol consumption to ensure they maintain their margin of safety. If patients are aware of the periods where they are most likely to be at risk of hypoglycaemia, it will enable them to be proactive by adjusting their carbohydrate intake or insulin dose accordingly.
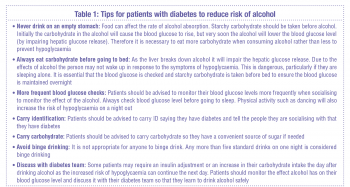 (click to enlarge)
(click to enlarge)
