Elbow pain is a commonly encountered presenting complaint in general practice. Lateral epicondylitis (LE) or ‘tennis elbow’ is the most common diagnosis in lateral elbow pain;1 its annual incidence has been reported as 1-3%, with men and women affected equally.2 It is more common in people over 40 years of age. Medial epicondylitis (ME) or golfer’s elbow is comparatively uncommon, with a prevalence of < 1%, occurring one third as frequently as the lateral elbow equivalent.3 Similarly to LE, it predominantly occurs in people in their forties and fifties, affecting men and women equally.
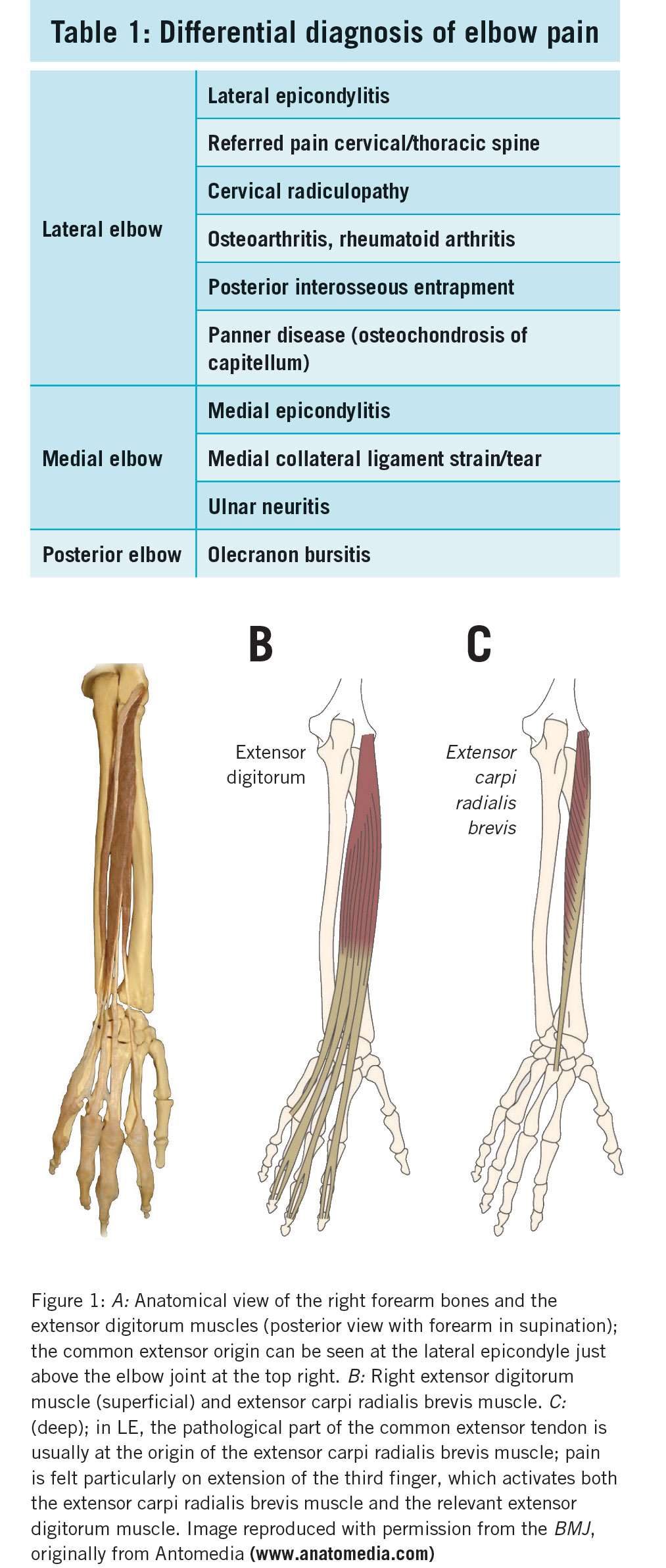
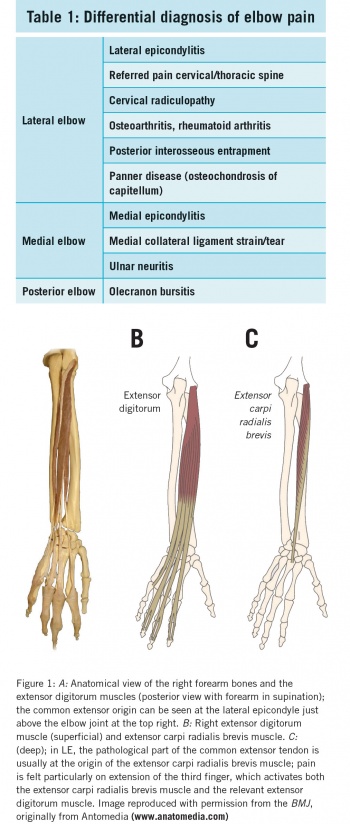
This article is primarily concerned with the management of LE and ME. However, elbow pain can arise from any of the structures associated with the joint, ie. tendons, ligaments, articular surfaces, nerves and bursae. Elbow pain may also be attributed to cervical radiculopathy or referred pain from the neck or ipsilateral shoulder. Differential diagnoses of elbow pain are presented in Table 1.
(click to enlarge)
Aetiology and pathogenesis
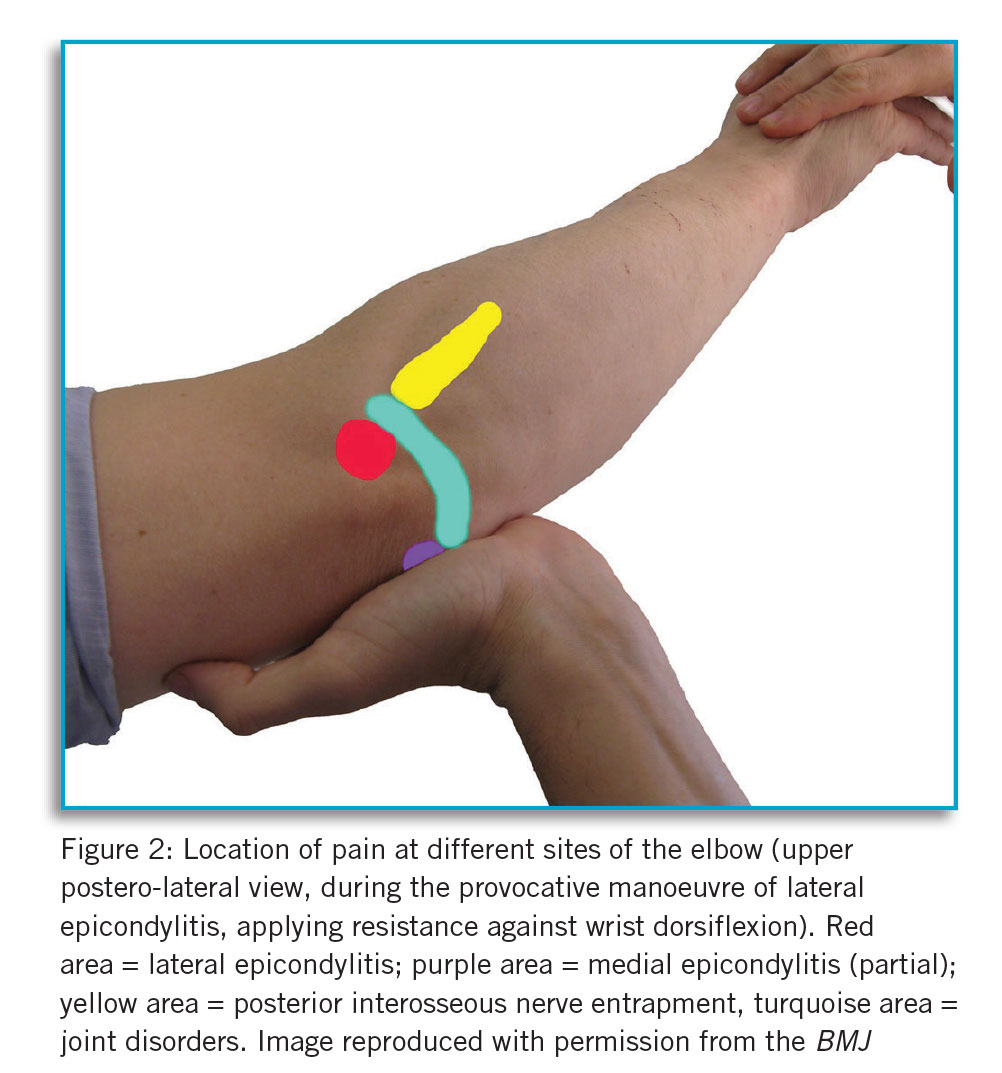
Strictly, it may be more accurate to describe LE as a tendinosis, a symptomatic degenerative condition of the wrist’s common extensor tendon origin, as inflammatory cells may be few on histological examination.1 However, it is referred to here as LE as this term is widely used and the distinction is not of significance in primary care. Extensor carpi radialis brevis (ECRB) is the most commonly affected muscle (see Figure 1). Repetitive use of the extensor muscles, eg. typing or manual labour, may lead to LE. Similarly, ME constitutes a tendinosis of the medial flexor/pronator tendon group. Patients complain of pain in the area just distal to the medial epicondyle of the humerus (see Figure 2). Those at risk of developing this condition include manual labourers who repetitively pronate the forearm and flex the wrist.
(click to enlarge)
Clinical assessment
History
The structures involved in the pain can usually be readily identified by asking the patient the site of the pain and what activities produce symptoms. Pain at the lateral elbow with gripping or lifting with the forearm pronated suggests LE. Where the patient is a tennis player, the backhand stroke is painful. Pain is usually insidious in onset but may be sudden after lifting a heavy object or after a forceful backhand. Medial elbow pain with gripping and/or wrist/elbow flexion implies ME.
Examination
With the patient’s upper limbs fully exposed, the elbows should be inspected. Observation should be made of the carrying angle of the elbows (normally a five degree [male] to 15 degree [female] angle). Any gross abnormalities such as erythema, ecchymosis, swelling or scars should be noted. The joint should be moved passively to assess pain, range of motion and end feel in flexion and extension at the elbow and supination and pronation of the forearm. Restriction in passive flexion of the elbow suggests an inherent joint issue such as osteoarthritis or rheumatoid arthritis. Similarly, restriction in passive supination and pronation of the forearm suggests arthritis of the proximal radio-ulnar joint. The patient is then asked to actively move the elbow joint. Limitation in active movement, with full passive range of motion, suggests pathology of muscles or nerves. Pain with resisted movement of the joint suggests muscle and/or tendon pathology.
There is full passive and active range of motion with LE and ME, provided there are no co-existent elbow conditions. Focal tenderness just anterior to the lateral epicondyle with the elbow flexed suggests LE. Diagnosis can be confirmed by resisted extension of the wrist with the elbow in extension. Pain is reduced by bringing the elbow into flexion. Pain is also expected with resisted extension of the middle finger.
Patients with ME experience pain on resisted flexion of the wrist. There may be reduced power in wrist flexion and forearm pronation compared to the unaffected side due to pain.3
Red flags
Urgent issues to be excluded at initial assessment include:
As clinical diagnosis is usually straightforward, investigations are generally not needed for LE and ME. Radiographs are normal. Nerve conduction studies are indicated for suspected concomitant nerve entrapment. Posterior interosseous nerve compression is coexistent with LE in 5% of cases;4 ulnar neuritis may be present in 20% of cases of ME.3
Management
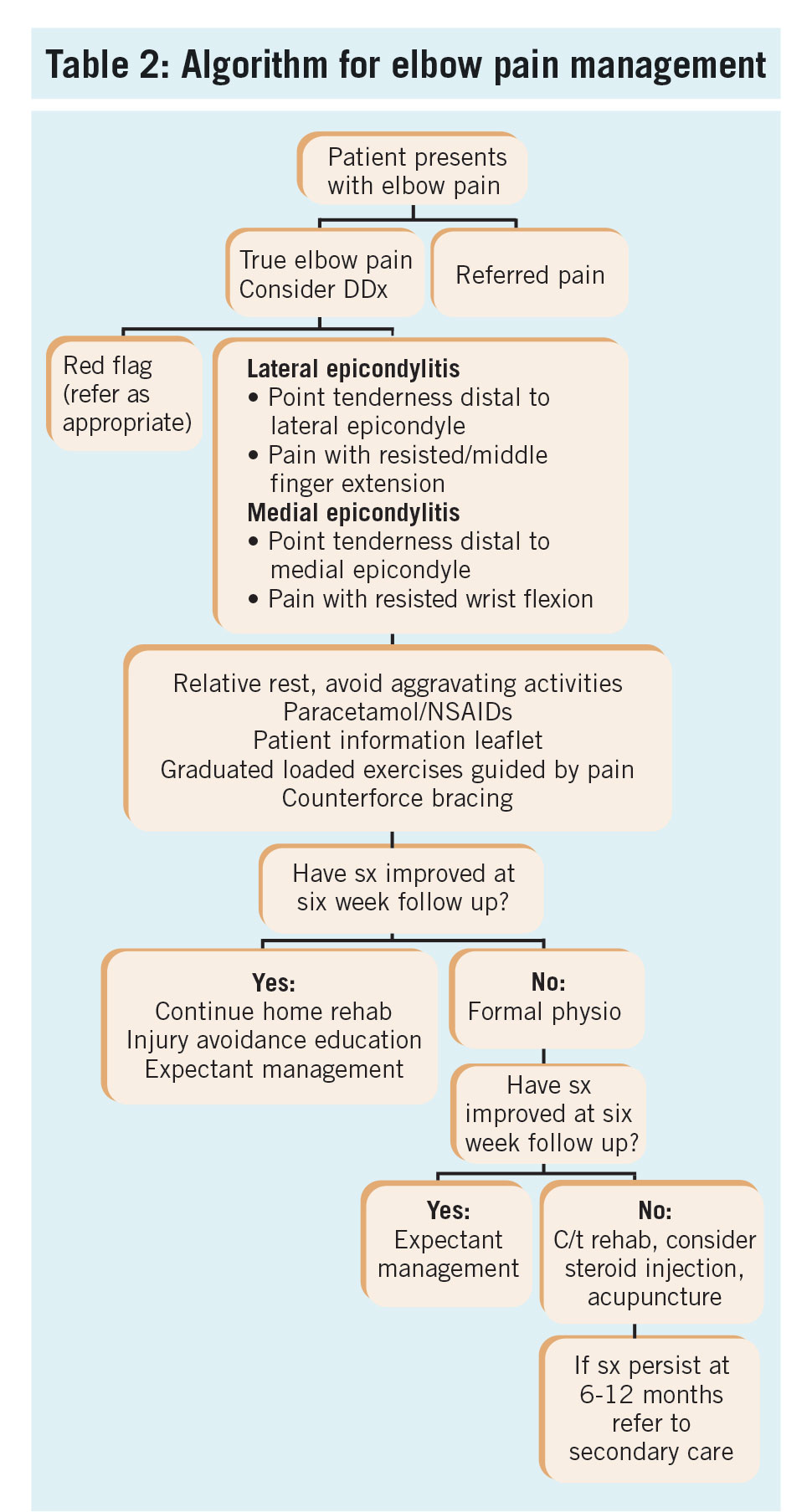
Given that LE is usually a self-limiting condition, resolving without treatment over 12 months, conservative treatment for that period of time is reasonable.5 ME should also be managed conservatively for six to twelve months.3,5 Acute treatment should aim at alleviating pain. Thereafter, the objective is to restore normal physical function and allow the patient to return to work/recreational activities. A suggested management algorithm is shown in Table 2.
(click to enlarge)
Acute pain relief and physiotherapy
Exercise is the key to managing acute elbow tendinopathy. Other treatments primarily serve to alleviate pain and facilitate rehabilitation.6 A period of relative rest should be advised, with the patient avoiding aggravating activities.1,4,5 The American College of Occupational and Environmental Medicine (ACOEM) recommends avoiding high force gripping activities in LE, albeit with an insufficient level of evidence.7 Short-term paracetamol may be used to provide temporary pain relief. It should be noted that topical and oral NSAIDs, while providing acute relief, will not alter the long term outcome of LE , while carrying the risk of NSAID-associated side-effects.8 Furthermore, NSAIDs have a theoretical risk of impairing tendon repair. While there has been a move from a ‘tendinitis’ to a degenerative tendinopathy model of pathophysiology, NSAIDs are still in common use clinically; benefits in short term use (seven to fourteen days) for relief of tendinopathy pain have been reported.9
To restore normal function, the tendon should be loaded appropriately to promote repair and strengthening and prevent weakening through underuse.8,10 Eccentric exercises with partial loading of the tendon are the mainstay of treatment of LE.8 Exercises should be progressively graduated. Pain during rehabilitation should be minimised through careful selection of load.6
Patient information leaflets on rehabilitation can be accessed at www.versusarthrits.org On return to sport, contributory deficiencies in equipment, eg. incorrect racquet grip or technique, should be addressed.
Counterforce bracing, deloading tape
With alleviation of stress on the affected tendon in mind, counterforce bracing may be applied to the proximal forearm in LE and ME. This may reduce pain and increase grip strength after three weeks.2 Use of a forearm strap for up to six weeks may improve ability to perform daily activities. Secondary nerve problems due to prolonged use of bracing have been reported.1 Deloading tape may be beneficial in those with severe pain or night pain.6
Corticosteroid injections
Local injection of a corticosteroid in the area of maximal tenderness is an option for acute pain relief. Injection of steroid in LE yields benefit at two to six weeks with respect to reduction in pain and increase in grip strength.2 Similar acute pain relief has been reported in ME.10 However, those treated with triamcinolone injection have been reported as less likely to have recovered or much improved at one year compared to placebo injections.11 They were also more likely to have had at least one recurrence. In addition, corticosteroid injection carries the risk of post-injection pain, hypopigmentation and lipoatrophy at the injection site with cosmetic consequences.
Where short-term pain relief is desired by the patient, eg. upcoming written exams, steroid injection may be considered. Having identified the point of maximal tenderness distal to the LE or ME with aseptic technique, 1ml triamcinolone may be injected into that point using a blue hub needle. The steroid should be ‘peppered’ around that point in a fan distribution. The patient should rest the elbow for 48 hours post-injection, with relative rest for 10 days. Stretching and strengthening exercises can be reintroduced after the rest period.
Botulinum toxin (botox)
The principle of a botox injection for treatment of LE is that paralysis of the extensor muscles will prevent repetitive trauma to the extensor tendons and thus allow repair. The clinical benefit of this intervention compared to placebo is as yet unproven.4 There is a high likelihood of finger extensor muscle lag (92% at eight weeks post-injection).6
Platelet-rich plasma and autologous blood injection
The proposed rationale for these treatments is the promotion of tendon healing through local delivery of growth factors and cytokines present in blood. There is currently insufficient evidence to recommend injections with autologous blood or platelet-rich plasma.4,6
Topical nitrates
One quarter of a 0.5mg/24h GTN patch may be placed over the most tender site of the extensor tendinopathy. Headaches and local skin rash are possible side-effects. GTN patches available in Ireland are not licensed for this use.
Acupuncture
While good short-term outcomes have been shown for acupuncture treatment of LE, long-term results remain unclear.1 The American College of Occupational and Environmental Medicine recommends acupuncture in individuals with chronic LE (with level of evidence ‘insufficient’).7
Surgery
As stated above, LE and ME are usually self-limiting conditions, settling within six to twelve months. Logically, therefore, referral to secondary care for consideration for surgery should be postponed until conservative measures have been employed for at least six months. Open, percutaneous and arthroscopic techniques have been described for the treatment of LE. Most techniques involve debridement of angio-fibrotic tissue at the ECRB tendon origin. Forced rest of the affected tendon followed by gradual reloading likely plays a part in the success of surgery.8
References
Vaquero-Picado A, Barco R, Antuna SA. Lateral epicondylitis of the elbow. EOR. 2016;1:391-397
Johnson GW, Cadwallader K, Scheffel SB, Epperly TD. Treatment of Lateral Epicondylitis. Am Fam Physician. 2007;76(6):843-848.
Barco R, Antuna SA. Medial elbow pain. EFFORT Open Rev 2017; 2;362-371
Javewd M, Mustafa S, Boyle S, Scott F. Elbow pain: a guide to assessment and management in primary care. BJGP 2015; 65:610-612
Descatha A, Despréaux T, Calfee RP, Evanoff B, Saint-Lary O. Progressive elbow pain. BMJ 2016;353:i1391
Brukner P et al. Clinical Sports Medicine. 5th Edition. Australia: McGraw-Hill Education;2017
Hegmann KT et al. JOEM. ACOEM Practice Guidelines: Elbow Disorders 2013;55(11);1365-1374
Orchard J, Kountouris A. The management of tennis elbow. BMJ 2011; 324:d2687
Rees JD, Stride M, Scott A. Tendons – time to revisit inflammation. Br J Sports Med 2014;48:1553–1557
Ciccotti MC, Schwartz MA. Diagnosis and treatment of medial epicondylitis of the elbow. Clin Sports Med 2004; 23:693– 70
Coombes BK, Bisset L, Brooks P, Khan A, Vicenzino B. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: a randomized controlled trial. JAMA 2013; 309 (5):461-9
 (click to enlarge)
(click to enlarge)