Recent study results have shown clear progress in improving outcomes for breast cancer patients
Prof Seamus O'Reilly, Consultant Medical Oncologist, Cork University Hospital, Cork and Dr Jodie Battley, Medical Oncology Registrar, Cork University Hospital, Cork
A record number of 19,859 attendees at this year’s European Society of Medical Oncology (ESMO) 2014 Congress in Madrid, discussed changes to oncology that will soon have a positive impact on the care of patients around the world.
The conference theme was Precision Medicine in Cancer Care, working towards the common goal of improved patient outcomes. There was a 24% increase in abstract submission and a 23% increase in registered attendees from 131 countries. The results of a number of very important studies were presented during the five-day meeting (September 26-30) that will have a direct impact on the way we treat patients in the clinic, in a range of tumour types including lung cancer, breast cancer, and melanoma. Summarised below are some of the highlights from the scientific programme focusing on the treatment of breast cancer.
HER2-negative metastatic breast cancer – the role of bevacizumab maintenance
Results from two randomised phase III trials investigating bevacizumab maintenance in HER2-negative metastatic breast cancer (MBC) were presented:
The IMELDA trial
The IMELDA study found that adding capecitabine to maintenance bevacizumab provided statistically significant and clinically meaningful improvements in progression-free survival (PFS) and overall survival (OS). In HER2-negative patients with locally recurrent/metastatic breast cancer, the combination of bevacizumab with first-line chemotherapy, particularly a taxane, was shown to improve PFS. Also, prolonging first-line chemotherapy results with maintenance treatment may influence overall survival (OS). Continued taxane chemotherapy, however, is limited by cumulative toxicity; capecitabine may provide a more tolerable maintenance alternative.
In this open-label randomised phase III study, patients with HER2-negative metastatic breast cancer without disease progression following bevacizumab/docetaxel, were randomised to bevacizumab alone or bevacizumab/capecitabine until disease progression.1 The addition of capecitabine to maintenance bevacizumab demonstrated significant improvements in PFS (HR 0.38, p < 0.001; median 11.9 versus 4.3 months) and improvement in median OS (HR 0.42, p < 0.001; 39 versus 23.3 months).
Important points raised by these results were that patients in the capecitabine/bevacizumab arm had a longer duration of treatment with twice the number of cycles than those in the bevacizumab alone arm. In addition, > grade 3 toxicities were almost doubled in the combination arm. Further data are required to clarify whether bevacizumab is an adequate maintenance therapy after response to first-line chemotherapy, and if these results truly represent a synergism between bevacizumab and capecitabine or the effect of capecitabine maintenance.
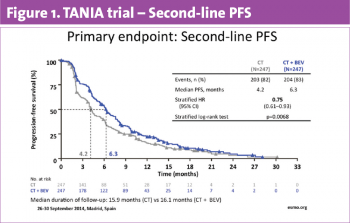
The TANIA trial
Results of the pre-specified second-line PFS analysis from the phase III TANIA study were also presented. Patients with HER2-negative, locally recurrent/metastatic breast cancer with disease progression during or after ≥ 12 weeks of first-line bevacizumab plus chemotherapy were randomised to second-line single-agent chemotherapy, either alone or with bevacizumab.
TANIA also met its primary endpoint demonstrating a small but statistically significant improvement in PFS with bevacizumab after progression on first-line bevacizumab-containing therapy, suggestive of maintenance of VEGF-dependent neo-angiogenesis following disease progression on bevacizumab.2 The median second-line PFS in the single-agent chemotherapy arm was 4.2 months compared with 6.3 months with the combination group (HR = 0.75; 95% CI, 0.61-0.93; p = 0.0068).
(click to enlarge)
There was an increase in stable disease but no difference in overall response rate. Consistent with prior studies, the most pronounced benefit was in triple-negative breast cancer (TNBC). Higher rates of toxicity were found in the chemotherapy/bevacizumab group. Final endpoints relating to third-line therapy and overall survival are anticipated in 2015.
At present, the role of bevacizumab in breast cancer remains uncertain and unclear benefits must be weighed against increased cost and toxicity.
HER2-positive metastatic breast cancer
The CLEOPATRA trial
The final overall survival data from the CLEOPATRA trial in patients with HER2-positive metastatic breast cancer (MBC) were presented. In this pivotal phase III study, 808 patients were randomised to receive first-line placebo/trastuzumab/docetaxel or pertuzumab/trastuzumab/docetaxel treatments. The previously presented results at primary analysis demonstrated statistically significant improvement in PFS and a strong trend to improvement in OS with the addition of pertuzumab.3 The OS benefit continued to improve at the second interim analysis. The latest analysis after 50 months median follow-up demonstrated that patients in the combination arm with pertuzumab lived 15.7 months longer than those who received trastuzumab and chemotherapy alone.4 The safety profile in the overall population and in patients who crossed over to the pertuzumab arm was consistent with the known safety profile of pertuzumab, with no new safety concerns seen with longer follow-up and no increase in cardiac toxicity.
CLEOPATRA is one of the first trials reporting an improvement in overall survival in patients with metastatic disease using targeted therapy. This substantial improvement confirms a pertuzumab-containing regimen as standard of care as first-line therapy for HER2-positive MBC. Looking to the future, additional studies are needed to establish if we can improve OS beyond five years, selection of patients that can forgo the need for chemotherapy, and identification of the mechanisms of resistance to HER2-directed therapy. An area of great interest going forward is the potential synergism with other emerging targeted therapies, P1K3CA/anti-PD1.
HER2-positive early breast cancer
The latest analysis of the large phase III trial ALTTO was presented at the ESMO meeting. Initial results, presented at ASCO 2014, showed no significant improvement in disease-free survival (DFS) with the addition of HER1-HER2 tyrosine kinase inhibitor lapatinib to trastuzumab in HER2-positive early breast cancer.5 A post-hoc analysis demonstrated improved outcomes with trastuzumab compared to lapatinib alone. After 4.5 years of follow-up, 18% of patients receiving lapatinib experienced at least one disease event, compared to 14% of patients receiving trastuzumab. A DFS benefit was also seen in disease-free patients who were offered trastuzumab as adjuvant treatment (at least one dose received by 52%) after being treated with lapatinib alone (HR = 0.67; 95% CI, 0.49-0.91).
This important trial, while negative, demonstrated better overall outcomes with a substantial number of women with HER2-positive breast cancer being cured with current chemotherapy and trastuzumab. Lapatinib alone may have some activity in the adjuvant setting, particularly in ER-negative disease.6 Positive results from the adjuvant neratinib trial have also been announced in a recent US press release.
Dual HER2 targeting in early breast cancer in the neoadjuvant setting
Dual HER2 targeting has been demonstrated as more effective than single HER2 blockade in the neoadjuvant setting as well as in metastatic disease. Two studies were presented addressing strategies to refine dual HER2 blockade. The randomised phase II EORTC 10054 study replacing neoadjuvant paclitaxel with docetaxel 100mg/m2 every three weeks following combination lapatinib/trastuzumab did not result in improvement in safety or tolerability of treatment. Meanwhile, lower than anticipated pathological complete response (pCR) rates were demonstrated in the German multicentre, open-label, phase II DAFNE study using a combination of trastuzumab and EGFR2 inhibitor afatinib followed by epirubicin/cyclophosphamide and trastuzumab.
Increased activity with dual HER2 blockade in PIK3CA wildtype tumours
Mutations in the PIK3CA gene are among the most common genetic aberrations in breast cancer. PIK3CA mutations occur in 20-25% of HER2-positive breast cancer. Preclinical data have found mutated PIK3CA to be associated with resistance to lapatinib and trastuzumab and have been demonstrated to carry a poorer prognosis in advanced HER2-positive breast cancer patients.
Presentation of retrospective analyses of three neoadjuvant trials, NeoALTTO, GeparQuinto and GeparSixto, evaluating the association between PIK3CA mutations and pCR, confirmed lower rates of pCR in patients with PIK3CA mutations. While mutation status did not impact on response to single HER2 blockade, PIK3CA wild-type breast carcinomas may be more sensitive to dual HER2 targeting than mutated disease. Prospective analysis is needed to further define the role of PIK3CA mutation status as a predictor of response to ensure that patients receive the most appropriate therapy for their tumour type. Several questions remain unanswered, such as, is pCR the best surrogate of survival in PIK3CA mutant breast cancer? How do these findings translate to the adjuvant setting? Will PIK3CA inhibition reverse resistance to HER2 blockade?
Immunotherapy in breast cancer
Evasion of immune destruction is an emerging hallmark of cancer. Although traditionally focused on ‘immunogenic’ solid tumours, such as renal cell carcinoma and melanoma, emerging evidence from preclinical and correlative studies indicate activity with immunotherapy agents in certain breast cancer subtypes, in particular HER2-positive and triple-negative breast cancer (TNBC) (see Figure 2).
(click to enlarge)
The role of tumour-infiltrating lymphocytes in breast cancer
In recent decades, an increasing body of evidence has emerged demonstrating that the immune system participates both in tumour development and in tumour elimination and control.7 Tumour-infiltrating lymphocytes (TILs) implicated in killing tumour cells, have been associated with improved patient outcomes, particularly for rapidly proliferating tumours with a higher mutational load. TIL count has been associated with improved survival in patients with oestrogen receptor-negative tumours. Large studies in the neoadjuvant and adjuvant settings suggest that TILS are a potential prognostic and predictive marker in breast cancer, especially in HER2-positive and TNBC subtypes.8,9 Results from the neoadjuvant GeparSixto trial indicate that the predictive effect of TILs for pCR is particularly evident with carboplatin. These results highlight the need to include TILs in clinical trial parameters and clinical studies for immune checkpoint inhibitors.
Increased understanding of the molecular complexities of breast cancer, identification of predictive biomarkers and advances in genomic technology continue to help define treatment strategies that it is hoped will lead to improved outcomes for breast cancer patients.
References
Gligorov J, Doval D, Bines J, et al. Maintenance capecitabine and bevacizumab versus bevacizumab alone after initial first-line bevacizumab and docetaxel for patients with HER2-negative metastatic breast cancer (IMELDA): a randomised, open-label, phase III trial. The Lancet Oncol 2014; (Early Online Publication) Sept 28
von Minckwitz G, Puglisi F, Cortes J, et al. Bevacizumab plus chemotherapy versus chemotherapy alone as second-line treatment for patients with HER2-negative locally recurrent or metastatic breast cancer after first-line treatment with bevacizumab plus chemotherapy (TANIA): an open-label, randomised phase III trial. The Lancet Oncol 2014; 15(11): 1269-1278.
Baselga J, Cortes J, Kim SB, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. NEJM 2012; 366(2): 109-119.
Swain SM, Kim SB, Cortes J, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA study): overall survival results from a randomised, double-blind, placebo-controlled, phase III study. The Lancet Oncol 2013; 14(6): 461-471.
Piccart-Gebhart MJ HA, Baselga J, et al. First results from the phase III ALTTO trial (BIG 2-06; NCCTG [Alliance] N063D) comparing one year of anti-HER2 therapy with lapatinib alone (L), trastuzumab alone (T), their sequence (T→L), or their combination (T+L) in the adjuvant treatment of HER2-positive early breast cancer (EBC). J Clin Oncol 2014; 32: 5s (suppl; abstr LBA4).
Goss PE, Smith IE, O’Shaughnessy J, et al. Adjuvant lapatinib for women with early-stage HER2-positive breast cancer: a randomised, controlled, phase III trial. The Lancet Oncol 2013; 14(1): 88-96.
Criscitiello C, Esposito A, Gelao L, et al. Immune approaches to the treatment of breast cancer, around the corner? Breast Cancer Res 2014; 16(1): 1-8.
Loi S, Sirtaine N, Piette F, et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin Oncol 2013; 31(7): 860-867.
Denkert C, Loibl S, Noske A, et al. Tumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancer. J Clin Oncol 2010; 28(1): 105-113.
 (click to enlarge)
(click to enlarge)
