“Surviving cancer is cool, but surviving old age is cooler.” Jarod Kintz
The worldwide population is aging. By 2050, one in every five people will be ≥ 60 years old and 21% of the older population is expected to be ≥ 80 years old. Increasing age is associated with increasing rates of cancer, corresponding to an 11-fold greater incidence in those aged 65 and older compared with their younger counterparts.1
Making the optimal treatment choice for the older patient is a complex multidisciplinary task requiring consideration of other medical needs arising from comorbid conditions and decreased physiological reserve.2 Co-ordination and partnership between members of the multidisciplinary team, the patient and their family and adequate resourcing by health funders represent the cornerstones of evolving models of care in geriatric oncology.
Older adults with cancer
Decision making in the elderly is complicated by the competing issues of decreased life expectancy (LE), increasing incapacity and disconnect between chronological age and functional age. The approach to managing older patients with cancer should take all these factors into consideration.
Determining whether symptoms will occur or life will be shortened by a cancer diagnosis helps to prioritise the value of treatment. Estimating LE is an important initial assessment of an older person with cancer that is often based on physicians’ experience as opposed to objective measurements. Tools such as www.eprognosis.com help to determine life expectancy independent of a cancer diagnosis.3
Physicians often fail to recognise mental incapacity.4 A dedicated effort should be made to establish a patient’s decision making capacity.5 Patient’s expectations of cancer treatment should also be ascertained, for example older patients may preference quality of life and functional capacity over prolonging survival.
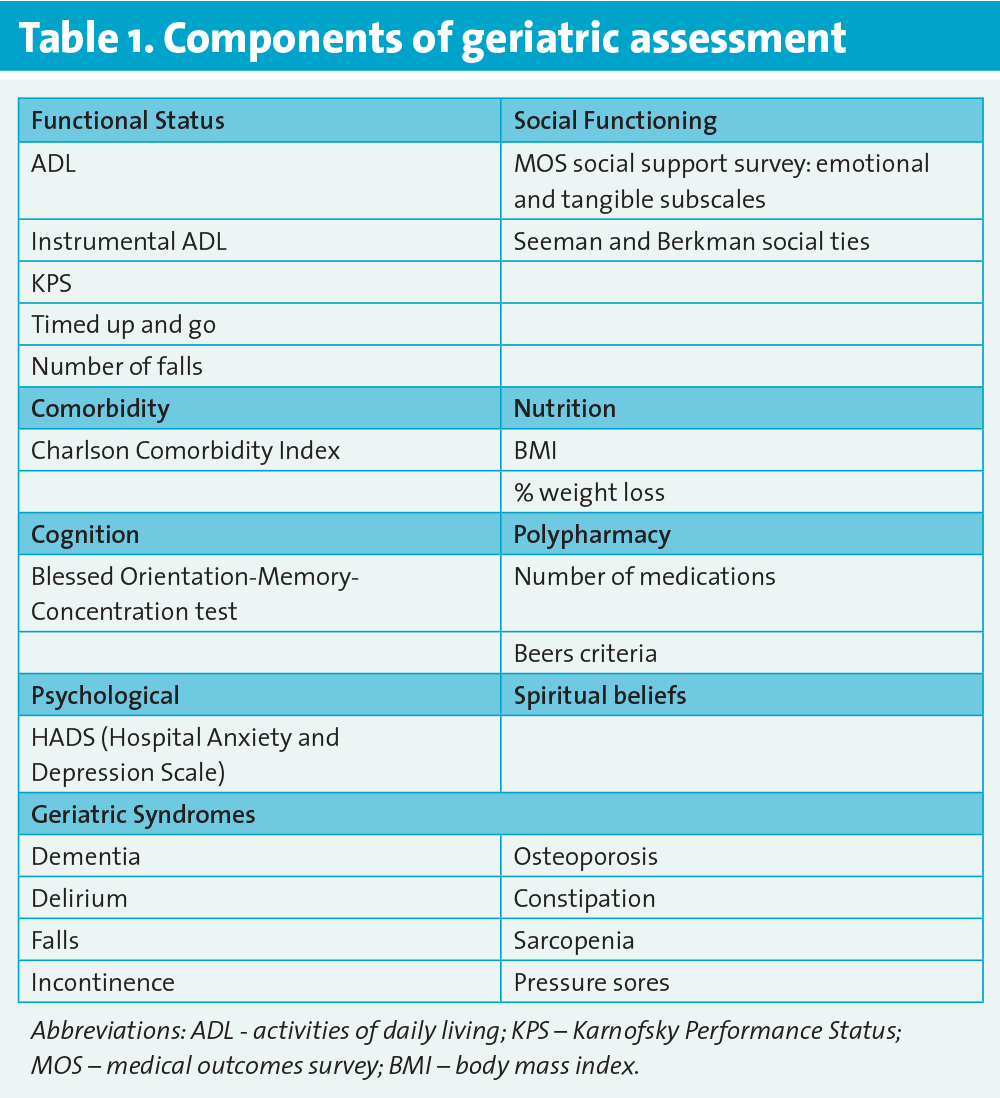
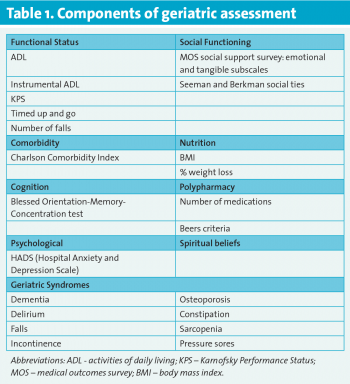
Aging is a heterogeneous process. Chronological age does not always equate to functional age. Decreased physiologic reserve is a hallmark of aging which may become readily apparent in the presence of a stressor, such as chemotherapy.6 A geriatric assessment (GA) is a multidisciplinary diagnostic process that evaluates the health of an older person through multiple domains.7
GA helps to identify health problems, estimate LE, and predict for toxicity, which are all relevant to older oncology patients (see Table 1).
(click to enlarge)
The aim of GA is to improve quality of care through directing targeted interventions and guiding appropriate treatment selection. Studies show that GA influences the cancer management plan in 20-50% of cases8,9 and leads to intervention in 25%.10 Prominent international bodies such as the US National Comprehensive Cancer Network and the International Society of Geriatric Oncology (SIOG) recommend GA in older patients.11,12 The SIOG taskforce on GA recommends performing a screening tool (eg. G-8 or VES13) in all patients ≥ 70 years with cancer followed by a GA in those with an abnormal screening result.
Older and younger adults derive similar benefit from chemotherapy.13,14 However, older patients are often not considered for chemotherapy or given attenuated regimens due to tolerability concerns.15,16 The Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) and the Cancer and Aging Research Group (CARG) score are predictive models incorporating geriatric and oncologic correlates of vulnerability to chemotherapy toxicity in older patients that help weigh the benefits and risks of chemotherapy17,18 It remains unknown, however, whether these tools are applicable to targeted therapy.
‘Prehabilitation’ describes interventions designed to improve functional capacity in anticipation of an upcoming physiologic stressor.19 This concept will become increasingly important in managing older oncology patients.
Challenges
Who constitutes an older person with cancer?
There is no consensus on the definition of an older adult with cancer. The operational definition of ‘frail’, ‘fit’ and ‘vulnerable’ formulated by Balducci and Extermann in 2000, has significant shortcomings.20
Appropriate referral of older patients for oncology opinion
Older age influences physicians’ decision to refer to medical oncology.21 Development of multidisciplinary care models and increasing awareness of the field of geriatric oncology should help to alleviate this problem.
Unique medical challenges of treating the older individual with cancer
Important pharmacokinetic differences can exist between older and younger patients that effect drug metabolism and the potential for toxicity.22 Age-related physiologic changes that predispose the older patient to toxicity include decreased haematopoietic stem cell reserves, reduced hepatic and renal function and loss of muscle mass. Comorbidities are prevalent in the older person and their influence on oncologic therapies can be detrimental.23
Lack of management guidelines for toxicity in the elderly can lead to suboptimal dosing and compromise outcomes.24 The prevalence of polypharmacy in older patients varies between 13% and 92%25 and is recognised as a common problem in older oncology patients.26,27 Compliance with oral chemotherapy is a potential challenge especially given the rise of oral chemo- and biologic therapies. Reduced mobility, visual, hearing and cognitive impairment are common in older patients and impact on their ability to attend for treatment and manage toxicities.
Lack of consensus regarding geriatric assessment
While there is a growing body of evidence supporting the use of GA in older patients with cancer, difficulties remain. There is no consensus regarding which domains or instruments should be used. The clinical value of GA has not been compared in a randomised manner with usual care in the oncology setting. Given the rising cost of cancer care it is not unreasonable that the cost-effectiveness of GA be determined before it deemed standard of care.28
The general principles of GA are thought to apply to all older adults, including those with cancer. Therefore, many believe GA is the gold standard and designing a clinical trial to study the utility of GA, whereby one arm receives less than standard of care, is probably unethical. However, countries such as Ireland where GA is not standard of care represent ideal environments to conduct such a landmark study.
Challenges for the caregiver
Family provide between 70-80% of the care needed for cancer patients.29 Spouse caregivers of older patients are often old themselves with comorbidities. This informal care system will become more important and physicians need to be aware of and assess the risk of psychological and physical problems for caregivers.30,31
Older patients may experience distress at the thought of being a financial burden to their family that can escalate into an inability to access to care. Recent data have shown that in the US, healthcare-related bankruptcy accounts for 33% of all personal bankruptcy.
Societal challenges
The projected rise in cancer incidence and cancer survivors places significant pressure on an overwhelmed oncology workforce. Ensuring appropriate staff exist to manage this problem represents a significant challenge. Combined geriatric oncology fellowship programmes exist in some centres in the US, such as Boston University and the University of Chicago, however, more are needed.
A potential solution
Technology can potentially integrate geriatric medicine and oncology care and represents a potential solution to some of the challenges highlighted. Older people are eager to embrace modern technology.32 The Positive Ageing Strategy in Ireland, launched in 2013, acknowledged the potential of assisted living technology to support older people in managing their chronic medical conditions at home and maintain their independence.33 Technology has many advantages, however human contact will always remain critical in the care of the older person with cancer.
Age bias
Clinical trials (CTs) help define a standard of care for the cancer patient. Older patients should always be considered for inclusion in CTs. Studies should endeavour to use populations that reflect clinical reality.34
Literature from the past decade is replete with articles documenting the scarcity of data to guide treatment decisions for older cancer patients.35 The elderly are thus under-represented in CTs. Talarico et al highlighted this issue a decade ago reporting that the proportion of older adults aged ≥ 65, ≥ 70 and ≥ 75 years enrolled onto registration trials for new cancer therapies, compared to the corresponding rates in the overall US cancer population from 1992-2002, were 36%, 20%, and 9% compared with 60%, 46%, and 31%, respectively.36 Ageism partly explains this problem. A survey of US oncologists indicated that 51% excluded patients from trials on the basis of age.37 This is despite patients’ willingness to participate in studies.38
Reports of CTs often fail to include population distribution by age and age-related efficacy and safety data.39 Selection bias depending on inclusion and exclusion criteria has led to exclusion of subgroups of older patients. For example, the AVEX trial enrolled patients ≥ 70 years with unresectable, metastatic colorectal cancer deemed unsuitable for oxaliplatin- or irinotecan-based regimens.40 The majority (> 90%) had an Eastern Co-operative Oncology Group performance status (ECOG PS) of 0 or 1. Why were these apparently fit patients unsuitable for irinotecan- or oxaliplatin-based chemotherapy? This raises concern regarding selection bias and our ability to apply results to the general older population. Elderly specific trials incorporating composite end points such as preservation of functional capacity are needed.41
Legislational change may be necessary to empower regulatory bodies to ensure adequate representation of older adults in drug registration trials.35
Rewards
Family, society, the physician and the patient all benefit from the appropriate management of the older oncology patient.
Integrating GA will hopefully prove to be a major step towards personalised medicine in the older oncology population, allowing us to make individualised decisions founded less on chronological but rather physiological age and ultimately allow us achieve the balance between treatment benefit and toxicity, and quantity versus quality of life.
Elderly people are valued for their positive contribution to their family unit and community. They embody the meaning of social connectedness. A quarter of older people in Ireland provide help to neighbours on a regular basis. A fifth volunteer at least once a week.42 Older adults are continuing to work beyond age 65. Extended labour market participation benefits the macro-economy by increasing output and delaying pension payments. Over 80% voted in the last general election highlighting the continued contribution older people make to society.42
Drawing from my own personal experience, one of the greatest rewards for the physician looking after older oncology patients is helping them to realise a good quality of life, which is paramount to the provision of good oncology care.
Conclusion
Dedicated geriatric oncology units and a co-management model similar to well established orthogeriatric services will in time tip the balance towards better care for the older individual with cancer and overcome the challenges discussed. However, irrespective of the model of care, it is imperative to create an environment of increased awareness of geriatric oncology throughout the fabric of our oncology community. We have a duty of advocacy to ensure optimal care for a population currently without a voice.
“Grow old along with me! The best is yet to be.” Robert Browning (1812-1889)
References
Surbone A, Kagawa-Singer M, Terret C, Baider L. The illness trajectory of elderly cancer patients across cultures: SIOG position paper. Ann Oncol 2007; 18: 633-8.
Balducci L, Aapro M. Complicate and complex: Helping the older patient with cancer to exit the labyrinth. J Geriatr Oncol 2014; 5(1): 116-118.
Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285: 2750-6.
Vellinga A, Smit JH, Van Leeuwen E, et al. Competence to consent to treatment of geriatric patients: judgements of physicians, family members and the vignette method. Int J Geriatr Psychiatry 2004; 19: 645-54.
Sessums LL, Zembrzuska H, Jackson JL. Does this patient have medical decision-making capacity? JAMA 2011; 306: 420-7.
Tanaka H, Monahan KD, Seals DR. Age-predicted maximal heart rate revisited. J Am Coll Cardiol 2001; 37: 153-6.
Rubenstein LZ, Josephson KR, Wieland GD, et al. Effectiveness of a geriatric evaluation unit. A randomized clinical trial. NEJM 1984; 311: 1664-70.
Caillet P, Canoui-Poitrine F, Vouriot J et al. Comprehensive geriatric assessment in the decision-making process in elderly patients with cancer: ELCAPA study. J Clin Oncol 2011; 29: 3636-42.
Aliamus V, Adam C, Druet-Cabanac M, et al. Geriatric assessment contribution to treatment decision-making in thoracic oncology. Rev Mal Respir 2011; 28: 1124-30.
Kenis C, Bron D, Libert Y et al. Relevance of a systematic geriatric screening and assessment in older patients with cancer: results of a prospective multicentric study. Ann Oncol 2013; 24: 1306-12.
Extermann M, Aapro M, Bernabei R, et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005; 55: 241-52.
Van Cutsem E, Kohne CH, Lang I, et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status. J Clin Oncol 2011; 29: 2011-9.
Muss HB, Woolf S, Berry D, et al. Adjuvant chemotherapy in older and younger women with lymph node-positive breast cancer. JAMA 2005; 293: 1073-81.
Muss HB, Berry DA, Cirrincione C et al. Toxicity of older and younger patients treated with adjuvant chemotherapy for node-positive breast cancer: the Cancer and Leukemia Group B Experience. J Clin Oncol 2007; 25: 3699-704.
Hurria A, Wong FL, Villaluna D et al. Role of age and health in treatment recommendations for older adults with breast cancer: the perspective of oncologists and primary care providers. J Clin Oncol 2008; 26: 5386-92.
Muss HB, Berry DA, Cirrincione CT et al. Adjuvant chemotherapy in older women with early-stage breast cancer. NEJM 2009; 360: 2055-65.
Extermann M, Boler I, Reich RR et al. Predicting the risk of chemotherapy toxicity in older patients: the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer 2012; 118: 3377-86.
Hurria A, Togawa K, Mohile SG et al. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicenter study. J Clin Oncol 2011; 29: 3457-65.
Carli F, Charlebois P, Stein B et al. Randomized clinical trial of prehabilitation in colorectal surgery. Br J Surg 2010; 97: 1187-97.
Balducci L, Extermann M. Management of the frail person with advanced cancer. Crit Rev Oncol Hematol 2000; 33: 143-8.
Kankesan J, Shepherd FA, Peng Y, et al. Factors associated with referral to medical oncology and subsequent use of adjuvant chemotherapy for non-small-cell lung cancer: a population-based study. Curr Oncol 2013; 20: 30-7.
Repetto L. Greater risks of chemotherapy toxicity in elderly patients with cancer. J Support Oncol 2003; 1: 18-24.
Yancik R, Ganz PA, Varricchio CG, Conley B. Perspectives on comorbidity and cancer in older patients: approaches to expand the knowledge base. J Clin Oncol 2001; 19: 1147-51.
Dale DC. Poor prognosis in elderly patients with cancer: the role of bias and undertreatment. J Support Oncol 2003; 1: 11-7.
Maggiore RJ, Gross CP, Hurria A. Polypharmacy in older adults with cancer. Oncologist 2010; 15: 507-22.
Puts MT, Costa-Lima B, Monette J, et al. Medication problems in older, newly diagnosed cancer patients in Canada: How common are they? A prospective pilot study. Drugs Aging 2009; 26: 519-36.
Lees J, Chan A. Polypharmacy in elderly patients with cancer: clinical implications and management. Lancet Oncol 2011; 12: 1249-57.
Puts MT, Hardt J, Monette J, et al. Use of geriatric assessment for older adults in the oncology setting: a systematic review. J Natl Cancer Inst 2012; 104: 1133-63.
Family caregiving in America: facts at a glance. 2012. (Accessed July 2013, at www.strengthforcaring.com/util/press/facts/facts-at-a-glance.html)
Goldzweiga G, Merimsb S, Ganonb R, et al Coping and distress among spouse caregivers to older patients with cancer: An intricate path. J Geriatr Oncol 2012; 3: 376-85.
Barbara Givena MG. Studies of caregivers of older cancer patients needed. J Geriatr Oncol 2012; 3: 295-8.
COBALT PROJECT. (Accessed 10.01.2014, at www.cobaltproject.org)
National Positive Ageing Strategy. In: Health Do, ed; 2013.
Aapro MS, Kohne CH, Cohen HJ, Extermann M. Never too old? Age should not be a barrier to enrollment in cancer clinical trials. Oncologist 2005; 10: 198-204.
Scher KS, Hurria A. Under-representation of older adults in cancer registration trials: known problem, little progress. J Clin Oncol 2012; 30: 2036-8.
Talarico L, Chen G, Pazdur R. Enrollment of elderly patients in clinical trials for cancer drug registration: a 7-year experience by the US Food and Drug Administration. J Clin Oncol 2004; 22: 4626-31.
Benson AB, 3rd, Pregler JP, Bean JA, et al. Oncologists’ reluctance to accrue patients onto clinical trials: an Illinois Cancer Center study. J Clin Oncol 1991; 9: 2067-75.
Townsley CA, Chan KK, Pond GR, et al. Understanding the attitudes of the elderly towards enrolment into cancer clinical trials. BMC Cancer 2006; 6: 34.
Lichtman SM. Clinical trial design in older adults with cancer - The need for new paradigms. Journal of Geriatric Oncology 2012; 3: 368-75.
Cunningham D, Lang I, Marcuello E, et al. Bevacizumab plus capecitabine versus capecitabine alone in elderly patients with previously untreated metastatic colorectal cancer (AVEX): an open-label, randomised phase 3 trial. Lancet Oncol 2013; 14: 1077-85.
Wildiers H, Mauer M, Pallis A et al. End points and trial design in geriatric oncology research: a joint European organisation for research and treatment of cancer – Alliance for Clinical Trials in Oncology – International Society Of Geriatric Oncology position article. J Clin Oncol 2013; 31: 3711-8.
Barrett A GS, Timonen V, Kenny RA (eds). Fifty Plus in Ireland 2011. First results from the Irish Longitudinal Study on Ageing (TILDA). In: Dublin; TILDA (The Irish Longitudinal Study on Ageing), 2011.
 (click to enlarge)
(click to enlarge)