General practice plays an increasingly important role in detecting and managing hepatitis C infection in the community, with recent developments in treatment offering a 95% cure rate
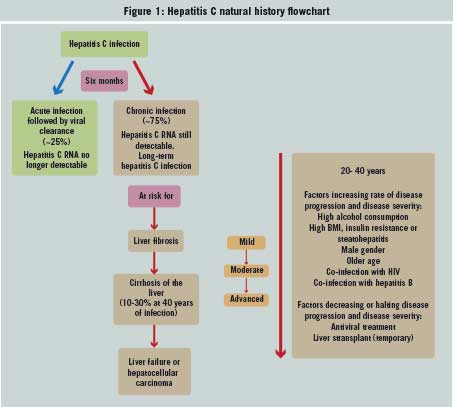
Hepatitis C (HCV) is a viral infection spread through contact with the blood of an infected person. The incubation period is between two weeks and six months. A person is infectious for the period. As long as the virus is detectable in their blood, they are viraemic.
Various studies show that between 15-45% of people will clear the virus within a year. However, it has been estimated that between 55-85% of patients untreated will develop chronic infection and are at risk of developing liver disease, namely cirrhosis and liver cancer. Liver disease develops gradually in chronic infection. The morbidity of HCV infection is closely related to the development of cirrhosis.
HCV was first identified in 1989. It became a notifiable disease in Ireland in 2004. The recent development of effective treatments has meant that 95% of people infected can expect to be cured. However, the major challenge, for GPs in particular, is to identify patients at risk in the community and diagnose and treat the disease.
Without good testing and treatment, mortality from the complications of chronic HCV will continue to increase. A recent study estimated that 60% of HCV infected people in Ireland have not been diagnosed.1
Healthcare provision is challenging as in Ireland many of those at risk of infection or already infected with HCV come from marginalised groups in society. Therefore, the aim of national policy is to create shared care programmes between hospitals and community settings. Patients treated in the community are likely to achieve the same outcomes as those under specialist care.
One of the challenges of HCV treatment across different settings is the need to collect outcome data – a key factor in eradicating the disease and assessing performance of the model of care being used. Collection of data depends on support across the treatment sites in providing appropriate information.
There are at least six different genotypes, with over 90 subtypes. Routine screening of blood donations commenced in 1991. Prior to that, some 1,700 people had been infected through contaminated blood.1 The current practice is that blood donated to the Irish Blood Transfusion Service is tested for anti-HCV. In addition, Individual Donation (ID)-NAT using a multiplex assay testing for HIV-RNA, HCV-RNA and HBV-DNA is undertaken.
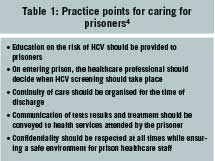
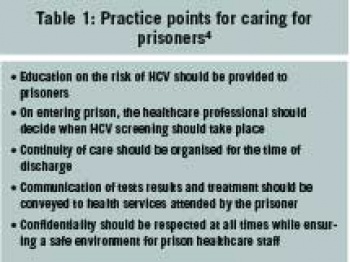
In recent years heroin injection has become the main risk factor, with various studies reporting a prevalence of 60-80% in that group. Prisoners also have high rates of infection of around 13%.
Some 70-80 million people are living with chronic HCV infection worldwide, according to a World Health Organization report.2 The Eastern Mediterranean region has the highest prevalence followed by the European region.
The virus was transmitted towards the end of the 20th century to many middle and low income countries as a result of healthcare procedures that were unsafe and also with the increase in injected drug use. Risk factors vary depending on the region.
Of the people infected worldwide, some 8% are injected drug users. This has an impact on how prevention, care and treatment services are provided and the need for a healthcare environment free from stigma and discrimination, according to the WHO report.
There is a larger ill-defined proportion of patients who are former drug injectors or who were infected through unsafe healthcare-related procedures. WHO recommends that people living with HIV should be tested for HCV infection. HIV co-infection doubles the risk of mother-to-child transmission and is associated with less spontaneous HCV clearance, higher HCV viral loads and more rapid progression of liver disease.
WHO has set a goal of eliminating HCV as a public health problem by 2030. Targets include reducing new HCV infections by 80%, the number of deaths by 65% and increasing HCV diagnoses from 20% to 90%.
In Ireland, the Health Protection Surveillance Centre (HPSC) gives the latest risk factor data for cases of HCV notified in 2018.3 People who inject drugs accounted for 64%. Other risk factors included received blood or blood products(3%), tattooing and body piercing (6%), various types of sexual exposure (10%) and no known risk factor (12%).
Highly effective direct-acting antiviral (DAA) treatments have been available in Ireland since 2015. These can eradicate the virus in 95% of cases.
“With improved case ascertainment, referral and treatment uptake, hepatitis C could become a rare disease in Ireland,” the HPSC notes.
(click to enlarge)
Screening
The HSE National Hepatitis C Treatment Programme was established in Ireland in 2016 with screening guidelines developed in 2017.4 The long asymptomatic period of the disease provides a window of opportunity for early detection in at-risk patients. There are clear criteria on whom and when to treat and both community and specialist services are in place in some areas. The HSE, the National Patient Safety Office and the ICGP provide support and guidelines for treating HCV patients.
Screening guidelines offer an assessment of the evidence on whether screening should be offered to various groups and examine the available evidence for and against.4 These groups include pregnant women, children born to mothers with HCV infection, household contacts of someone with HCV infection, those abusing non-injectable drugs, prisoners, donors of blood, tissue or organs and healthcare workers.
An aspect to bear in mind is that episodes of risk may have occurred years before the patient presents. They may have engaged in past intravenous drug usage, have lived in an area of high HCV prevalence, had a blood transfusion or procedure in a country where health practices are less than safe or have undergone tattooing in a non-sterile environment.
HCV testing can be done using different types of specimens including serum, plasma, dried blood spots and oral fluid. Serum and plasma using quality assured assays are preferred for screening and diagnostic testing. A plain serum blood test is sent to the National Virus Reference Laboratory and it is advisable to request reflex RNA testing and genotyping on each sample.
Other blood-borne viruses with the same risk factors for transmission, HIV and HBV, should be requested at the same time. This avoids having to do a second blood test. Co-infection will affect the type of treatment and the treatment setting. Therefore a vaccination history should be taken to determine if the patient has been already vaccinated for hepatitis B and A.
Some patients will have had incomplete travel vaccination schedules and therefore inadequate response to hepatitis B vaccine, requiring booster or re-vaccination with hepatitis B. The patient should also be vaccinated for hepatitis A if indicated.
The following aspects should be considered:
Any contact with health services provides an opportunity for screening at risk patients
Some patients may have more than one risk factor for HCV and require repeat screening
When offering screening, the patient should be counselled on the testing process, how results will be received and the importance of returning for test results stressed
Confidentiality is key in all steps of the process
Take the opportunity to counsel about prevention and harm reduction.
Diagnosis
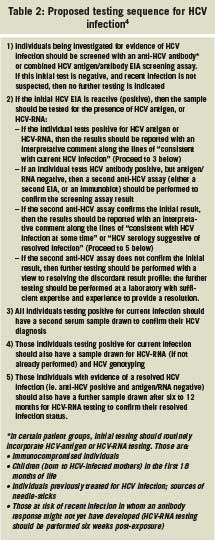
HCV infection is diagnosed by the detection of antibody to HCV (anti-HCV) in blood or oral fluid of the detection or the detection of HCV core antigen (HCV-Ag) or HCV-RNA in the blood. Antibodies are detectable from seven to eight weeks after infection.4
A positive antibody test will not distinguish between acute, chronic or resolved infection. If a person has had a recent negative test, this may be helpful. Chronic disease is diagnosed if HCV-RNA is still detectable after six months.
Detection of HCV-RNA by nucleic acid testing indicates current infection. HCV-RNA can be detected from one to two weeks after infection.
Initial infection with HCV is asymptomatic or mildly symptomatic so infection is commonly not detected in the acute phase. Common symptoms include nausea and vomiting, jaundice, abdominal discomfort and loss of appetite.
Progression to chronic liver disease is associated with excessive alcohol intake, co-infection with hepatitis B, HIV, being male and older age. Liver transplant may be the required treatment for some patients.
Developments in treatment have occurred along with advances in testing methods. A non-invasive fibroscan can stage HCV-associated liver disease. This has largely replaced the need for liver biopsy. These recent advances mean that there is an increased role for primary care in identifying and managing HCV patients.
Treatment
The availability of direct-acting antivirals (DAAs) has revolutionised HCV treatment in the past five years, with a cure possible in most patients. Previously HCV was treated with interferon and ribavirin-based regimens that required parenteral administration. These had many adverse side-effects with poor outcomes for many genotypes. In addition, they were contraindicated in many high-risk groups.
Treatment duration was long, often up to six months. Liver disease staging was carried out by liver biopsy and this proved a major barrier for patients to HCV treatment. Also, treatment was limited to hospital-based services.
From December 2014, access to oral interferon-free DAA regimens were made available as part of an early access programme for patients with specific clinical parameters.
The National Hepatitis C Treatment Programme (NHCTP) was set up in March 2015 and its clinical groups make recommendations on treatment and follows the National HCV strategy.
The new DAA drugs were initially prioritised for patients who acquired their infection through blood products. This was then extended to wider access, irrespective of fibroscan score or histologic staging. The guidelines were then extended to hospital-based and community treatment sites. The guidelines cover preferred regimens for patient without cirrhosis (fibroscan less than 12kPa or liver biopsy with stage 111/IV fibrosis), and regimens for patients with compensating cirrhosis.
At present, community treatment is available for non-cirrhotic patients with a fibroscan score of less than 12kPa. The efficacy of new treatments and the increased tolerability of interferon-free regimens has made exact staging of disease less important. More complicated patients with cirrhosis are treated in eight hospital-based treatment centres.
GPs have a major role to play identifying undiagnosed patients and managing care or referring to specialist services. Community-based treatment may be easier to access and may be a more suitable setting for some patients. This had been piloted successfully.
(click to enlarge)
Exclusions for community treatment include5:
Cirrhosis with fibroscan > 12kPa
Co-infection with HIV or hepatitis B
Previous treatment with DAAs for hepatitis C
Pregnancy or lactation
Less than 18 years of age
Organ transplant recipient or immuno-compromised (eg. steroids, azathioprine or TNF inhibitors)
Renal failure requiring replacement therapy
Major medical comorbidity
Significant drug interactions difficult to manage in primary care.
DAAs are now available free of charge to all patients with chronic HCV infection. Choices for community treatment are pangenotypic regimens and indications. The community-based initiatives have proved successful and have engaged large numbers of patients who may have previously not attended hospital clinics.
Access to DAA treatment through the National HCV Treatment Programme requires the following assessment to be made and reported, prior to commencing therapy. Full recommendations on drug regimes for various patients are set out by its Clinical Advisory Group.6
Registration with the National HCV Treatment Registry
Baseline HCV-RNA assessment within six months of the start date of treatment
Baseline laboratory parameters as per protocol
Evaluation of liver staging (impact of cirrhosis staging on treatment duration, ribavirin, etc):
– Fibroscan – kPa, IQR, success rate
– Serum markers of fibrosis, if available
Evaluation of cirrhosis staging
Assessment for potential drug-drug interactions.
Treatment lasts for between eight and 12 weeks. Side-effects are minimal. It is usual that patients report good effects within two to three weeks of starting treatment.
DAAs for community treatment5
Sofosbuvir/velpatasvir 400mg/100mg: One tablet daily at the same time each day. Twelve-week course. Main side-effect is headache.
Glecaprevir/pibrentasvir 100mg/40mg: Three tablets daily with food. Eight-week course. Main side-effects are headache and fatigue.
Patients are PCR-tested 12 weeks after completing treatment to assess whether the drug has been effective and there has been a cure. Sustained virological response (absence of active virus – PCR negative) is defined as a cure and is expected in 90-95% of patients. A national register keeps track of people who have been successfully treated and to date this exceeds 5,000 people (including over 2,00 injected drug users).
When prescribing DAAs, there is a potential for drug-drug interactions. Special attention should be given to taking a full drug history and a medication review. This includes prescribed medications, OTCs, herbal products and illicit drugs. Where potential drug-drug interactions are unavoidable, alternative treatment may have to be considered.
(click to enlarge)
One group for concern is patients who are using fentanyl recreationally. Treatment with glecaprevir/pibrentasvir (Maviret) could lead to life-threatening or fatal respiratory depression. Caution is advised in patients taking GHB and they should be monitored for adverse events. Drug-drug interactions can be checked at www.hep-druginteractions.org/checker
Women are advised to avoid pregnancy during treatment and contraceptive methods should be discussed. The practice within the current programme is to stop DAAs where a pregnancy occurs, although there is limited information to date on adverse effects in patients exposed to DAAs.
This is an important public health programme so significant budget and resources for medication have been provided by the HSE. Training is available for GPs who want to treat patients and also play a role in prevention and detection of HCV. The ICGP ran a day course in HCV management in February and is providing ongoing educational resources to GPs.
Several challenges to diagnosis and treatment that need to be overcome still remain. Interferon-related treatment fears still persist. Many parts of the country have no access to mobile elastography or treatment centres. There is still a stigma around HCV infection. At present resources have not yet been allocated for implementation or assessment of the effectiveness of guidelines.
The ICGP’s Addiction Management in Primary Care provides GP education in this area and runs regular training workshops.
References
Thornton et al. Determination of the burden of hepatitis C virus infection in Ireland. Epidemiol Infect 2012; 140(8): 1461-8
World Health Organisation Global Hepatitis Report 2017 available at www.who.int/hepatitis/publications/global-hepatitis-report2017/en/
HPSC. Epidemiology of hepatitis C in Ireland – April 2019 available at www.hpsc.ie/a-z/hepatitis/hepatitisc/
Hepatitis C Screening. National Clinical Guideline No. 15. National Patient Safety Office available at www.gov.ie
National Hepatitis C Treatment Programme, Clinical Advisory Group, Community Treatment Guidelines 2019 available at www.hse.ie/eng/national-hepatitis-c-treatment-programme/
National Hepatitis C Treatment Programme. Clinical Advisory Group Treatment Guidelines 2020
 (click to enlarge)
(click to enlarge)