Immunisation: Update on the national HPV programme
The HPV schools vaccination programme is currently being extended to boys. GPs are in a position to highlight the importance of the HPV vaccine in cancer prevention to their patients
Ms Lucy Jessop, Director, HSE National Immunisation Office, Dublin
We are living in exciting times where the elimination of cervical cancer as a public health problem may be possible in the future. In May 2018, the director general of the World Health Organization announced a global call to action towards the elimination of cervical cancer, underscoring renewed political will to make elimination a reality, and called for all stakeholders to unite behind this common goal. This elimination will require high coverage of HPV vaccine and cervical cancer screening.
We also now know that HPV causes more than just cervical cancer and that the vaccine can provide benefits to both boys and girls.
Following an announcement by Health Minister, Simon Harris in December 2018, the HPV programme in Ireland is being extended to include both boys and girls in first year of second level school from the academic year 2019-20.
What is human papillomavirus?
Human papillomavirus (HPV) is a double stranded DNA virus that infects squamous epithelia including the skin and mucous membranes of the upper respiratory and anogenital tracts. There are more than 100 different types of HPV, most of which are responsible for verrucae.
However, a causative association between HPV and cervical cancer was first recognised in the 1970s by Prof Harald zur Hausen.1 In 2000, evidence for a causal association between human papillomavirus and a subset of head and neck cancers was reported.2
At least 14 oncogenic HPV types have been identified. Although most HPV infections are asymptomatic and self-limiting, persistent infection with oncogenic HPV subtypes HPV 16, 18, 31, 33, 35, 45, 51, 52, and 56, may cause cancers of the cervix, oropharynx, anus, vagina, vulva and penis.
Persistent infection by such high-risk oncogenic HPV types is detectable in almost all cervical cancers. Of these high-risk oncogenic types, HPV16 is responsible for more than 60% and HPV18 for at least 15% of all cervical cancers. Oncogenic HPV is also responsible for a range of other precancerous lesions of the cervix, vagina and vulva in women. HPV types 6 and 11 are known to cause anogenital warts in both women and men.
Burden of HPV associated invasive cancers
The burden of HPV-related disease is now recognised as substantial. HPV is reported to be responsible for approximately one in every 20 cases of cancer across the world.
In July 2016, the Centers for Disease Control and Prevention (CDC) reported that more than 90% of anal cancers, almost 70% of vaginal and vulvar cancers, over 70% of oropharyngeal cancers and more than 60% of penile cancers are attributable to HPV.3 Overall rates of HPV associated invasive cancers are increasing in high income countries.
In the US the incidence of oropharyngeal cancers among men has now overtaken the incidence of cervical cancers in women. In 2018, there were 18,226 cases of oropharyngeal cancer and 11,866 cases of cervical cancer reported.
HPV-associated invasive cancers in Ireland
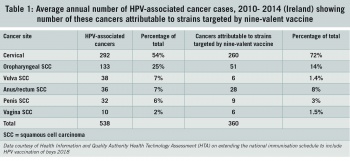
In Ireland, an estimated average of 538 HPV-associated cancers are diagnosed in both women and men every year. (see Table 1). A HPV-associated cancer is a specific cellular type of cancer that is diagnosed in a part of the body where HPV is often found. Three out of four of these cancers are diagnosed in women and one out of four in men. A HPV-attributable cancer is a cancer where there is direct evidence that the cancer is caused by HPV.
(click to enlarge)
Of the 538 HPV-associated cancers reported per year, 406 cancers are attributable to HPV infection. Of these cases, 307 are attributable to HPV 16 and 18 (targeted by the current four-valent HPV vaccine) and a further 53 cases are attributable to HPV 31, 33, 45, 52 and 58 (additionally targeted by the nine-valent HPV vaccine).
Cervical cancer is the most frequent HPV-associated cancer, with on average 292 cases diagnosed each year and from which 86 women die each year. Of the 292 cervical cancers caused by HPV, 260 (89%) are attributable to HPV strains targeted by the nine-valent HPV vaccine.
The next most frequent HPV-attributable cancers are oropharyngeal squamous cell carcinomas, of which 133 are diagnosed per year, with 75% of cases in men. Fifty-one (38%) of oropharyngeal squamous cell carcinomas are attributable to HPV strains targeted by the nine-valent HPV vaccine. Each year 25 people die secondary to oropharyngeal cancer in Ireland.
Thirty-one squamous cell carcinomas of the anus are diagnosed each year, 20 of these cancers (65%) are diagnosed in women. Twenty-five (90%) of these cancers are attributable to HPV strains targeted by the nine-valent HPV vaccine. See Table 1 for further information.
In Ireland there was annual increase of 2% in the rate of HPV-associated invasive cancers for women and men between 1994 and 2014.4
In fact, a recent clinical audit on oropharyngeal cancer cases diagnosed in the five-year period 2014-2018 reported a 37% increase in such cases compared with cases reported to the National Cancer Registry Ireland (NCRI) in the five year period 2009-2013.4 Overall, 77.5% of these cancers were in men, and approximately half are thought to be attributable to HPV.
HPV vaccines
Currently, there are two HPV vaccines available in Ireland. Gardasil (HPV4) was licensed in 2006 to prevent premalignant genital lesions (cervical, vulvar and vaginal) and cervical cancers causally related to HPV types 16 and 18 and types 6 and 11 that cause 90% of genital warts.
In 2014, Gardasil 9 (HPV9) was licensed. Gardasil 9 provides protection against seven oncogenic HPV types 16, 18, 31, 33, 45, 52, and 58. These seven HPV types are causative organisms in almost 90% of cervical cancers. Types 6 and 11 are causative organisms in 90% of genital warts.
The Gardasil 9 licensed indications are for protection against premalignant lesions and cancers affecting the cervix, vulva, vagina and anus caused by vaccine HPV types and genital warts. With time it is expected that the HPV vaccine will also be effective in reducing the incidence of other HPV attributable cancers.
The National Immunisation Advisory Committee (NIAC) recommends HPV vaccines may be given to men and women from nine to 26 years of age and to MSM up to 45 years of age.5
The HSE HPV vaccine programme will provide Gardasil 9 to boys and girls in the first year of second level school from September 2019.
Ideally, the vaccine should be administered before exposure to HPV at sexual contact and the vaccine is likely to be more effective in younger people because they have not been exposed to HPV.
The vaccine administration schedule is gender neutral for both HPV vaccines.
For those aged less than 15 years, the schedule is two doses given at 0 and 6 months. The minimum interval between dose one and dose two is five months for Gardasil 9. For those aged 15 years or older the schedule is three doses given at 0, 2 months and 6 months.
HPV vaccine effectiveness
In May 2018 a Cochrane Review of human papillomavirus (HPV) vaccines, based on 26 studies which included 73,428 women, reported that HPV vaccines were very effective in reducing precancers of the cervix and changes that could lead to cervical cancer. The Cochrane review also reported that HPV vaccines cause no serious side-effects.6
This review reported HPV vaccine was most effective against precancerous changes of the cervix when given to women aged 15-26 years. However, if the vaccine is given to young women who are negative for HPV infection at the time of vaccination, almost all cervical lesions caused by HPV 16 and 18 are eliminated.
HPV 16 and HPV 18 antibody levels in those vaccinated have remained stable and above natural infection-related antibody levels for up to 12 years. There is no evidence of weakened protection over time,7 therefore no booster doses are currently recommended.
In March 2019 the BMJ reported that routine HPV vaccination of 90% of all girls aged 12-13 years in Scotland since 2008 has led to a dramatic reduction in cervical precancers with an 89% drop in the numbers of those with CIN3 disease.8
HPV vaccine safety
In July 2017, The World Health Organization (WHO) Global Advisory Committee for Vaccine Safety (GACVS) reported that HPV vaccines were considered to be extremely safe, advising that the risk of anaphylaxis was approximately 1.7 cases per million doses and that syncope was established as a common anxiety or stress-related reaction to the injection.
No other adverse reaction was identified and GACVS considered HPV vaccines to be extremely safe. The GACVS had previously reviewed the evidence on the safety of HPV vaccine (Gardasil) in 2007, 2008, 2009, 2013, 2014 and 2015. WHO has never reported safety concerns with HPV vaccines.9
Internationally, no regulatory authority has issued a safety signal for any HPV vaccine.
HSE School Vaccination Programme
Since 2010 the HSE has offered the HPV vaccine (Gardasil) to all girls in first year in second level schools as primary prevention of HPV infection. Subsequently, this vaccine will provide protection from cervical cancer in adulthood. It was estimated that the HPV vaccine Gardasil would prevent the deaths of almost 70 women annually, if the vaccine target uptake of 80% was reached each year.
HPV vaccine programme for boys
HPV infection affects men and women almost equally but there is a naturally lower immune response to HPV infection in men.10 However trials on immunogenicity of the HPV-16/18 vaccine showed substantially higher immune response in young men compared with women of similar age groups. Post-vaccination antibody levels for the HPV-type vaccines were up to three times higher in boys than in girls.11
As a result of a health technology assessment (HTA) by the Health Information and Quality Authority (HIQA) and on the recommendation of the Department of Health, the HPV vaccine programme will be extended to boys in their first year of second level school.12
The HPV vaccine is being recommended for boys because:
HPV vaccination of boys provides direct protection against HPV-related disease to boys
– Every year, of the 538 cancers associated with HPV diagnosed in Ireland, a quarter are diagnosed in men. More than 75% of oropharyngeal cancers attributed to HPV are diagnosed in men.
– Unlike cervical precancers there is no screening test available for oropharyngeal, anal or penile cancers in men.
Vaccinating boys also provides greater protection to women
– Currently, women have the greatest burden of HPV disease in cervical cancer.
– However, this is likely to change, if HPV attributable oropharyngeal cancers continue to increase in Ireland.
– Universal vaccination for boys and girls would prevent further cervical cancer in women by herd immunity and will be likely to reduce the overall burden of HPV-related malignancy sooner than would a girls only programme.
A gender-neutral programme ensures that the vaccine programme is more robust
– In view of the recent decrease in HPV vaccination uptake among girls in Ireland a gender neutral programme ensures that the vaccine programme is more robust in relation to potential short-term fluctuations in uptake
Protection of vulnerable groups
– Extension of the HPV vaccine programme to include boys will likely greatly improve protection against HPV infection and associated HPV-attributable disease in vulnerable groups, eg. the MSM and migrant groups.
Change to HPV vaccination programme
HIQA recommended that the HPV immunisation programme should change to a HPV 9 vaccine programme, stating that a gender-neutral HPV 9 vaccine programme would be more effective than a girls-only HPV 9 vaccine programme. It is estimated that changing from a HPV 4 vaccine girls-only programme to a gender-neutral HPV 9 vaccine programme could prevent 113 deaths from HPV-attributable cancers annually. See Table 2 for information.
(click to enlarge)
However, HIQA stated that extending the HPV immunisation programme to boys and changing to a Gardasil 9 vaccine programme needs to be accompanied by a public awareness campaign to ensure adequate knowledge among parents about HPV-attributable disease and the benefits of HPV 9 vaccine not only for girls but also for boys.
GPs and practice nurses are in a position to inform parents about the importance of the HPV vaccine in cancer prevention. It is important that all healthcare staff have the relevant information to answer queries and concerns of parents and pupils about HPV vaccines.
The National Immunisation Office is producing an e-learning module on the online learning portal HSeLanD about the HPV vaccine programme including information on the gender- neutral programme for first years at second level school. We would encourage all GPs and practice nurses to look at this module to increase their knowledge and confidence in explaining and promoting the Gardasil 9 vaccine to parents and young people.
Gillison ML, Koch WM et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. Semin Oncol. 2004 Dec;31(6):744-54
HPV-Associated Cancer Statistics www.cdc.gov/cancer/hpv/statistics/index.htm
NCRI. Cancer trends: HPV-associated cancers. National Cancer Registry Ireland. 2017
National Immunisation Advisory Committee. Immunisation Guidelines for Ireland Dublin: Royal College of Physicians of Ireland. www.hse.ie/eng/health/immunisation/hcpinfo/guidelines/chapter10.pdf
Arbyn M, Xu L, Simoens C, Martin-Hirsch PPL. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. Cochrane Database of Systematic Reviews 2018, Issue 5. Art. No.: CD009069
Artemchuk M, Eriksson T et al, Long-term antibody response to human papillomavirus vaccines: up to 12 Years follow-up in the Finnish Maternity Cohort. Journal of Infectious Diseases, Volume 219, Issue 4, 29 January 2019, Pages 582-589
Palmer T, Wallace L, et al, Prevalence of cervical disease at age 20 after immunisation with bivalent HPV vaccine at age 12-13 in Scotland: retrospective population study BMJ 2019;365:l1161 www.bmj.com/content/365/bmj.l1161
WHO, Safety update of HPV vaccines (2017) www.who.int/vaccine_safety/committee/topics/hpv/June_2017/en/
Giuliano AR, Lu B, Nielson CM, Flores R, Papenfuss MR, Lee JH, et al. Age-specific prevalence, incidence, and duration of human papillomavirus infections in a cohort of 290 US men. J Infect Dis 2008;198:827-835
Block SL, Nolan T, Sattler C, Barr E, Giacoletti KE, Marchant CD. Protocol 016 Study Group. Comparison of the immunogenicity and reactogenicity of a prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in male and female adolescents and young adult women. Pediatrics. 2006 Nov; 118(5):2135-45.
Health Technology Assessment (HTA) of extending the national immunisation schedule to include HPV vaccination of boys. Health Information and Quality Authority (HIQA) Dec 2018. www.hiqa.ie/sites/default/files/2018-12/HTA-for-HPV-Vaccination-boys.pdf
 (click to enlarge)
(click to enlarge)
