Lung cancer has the highest rate of cancer mortality with 1.59 million annual deaths worldwide, according to the World Health Organisation in 2012. It is the most commonly diagnosed cancer in males and third most common in females. In Ireland, in 2013, there were 4,508 lung cancer patients and an annual incident rate per 100,000 of 40.3 and 57.2 in females and males respectively. Prognosis has only slightly improved over the past two decades with the five-year net survival increasing from 9.3% in 1994 to 14.4% in 2011. The outcome depends on many factors including grade, type and stage of lung cancer.
Non-small cell lung cancers
Approximately 87% of primary lung cancer are grouped into a single category: non-small cell lung cancer (NSCLC), consisting of adenocarcinomas, squamous cell carcinomas, large cell carcinomas and bronchial carcinoid tumours.1,2,3,4 Regarding NSCLC, wide-excision surgery is considered the therapy of choice, however, only 20-25% of patients are suitable for such procedures.5 Risk factors include smoking (polycyclic hydrocarbons) and occupational and radon exposure. Histologically, NSCLC is characterised by larger cells and abundance of cytoplasm. Patients may have a mixture of subtypes. Due to its tendency for early micrometastases and dissemination, many patients relapse post surgery and radiotherapy. Studies have also shown limited benefit on overall survival with platinum-based chemotherapy agents.6, 7
Small cell lung cancers
Approximately 13% of all primary lung cancers diagnosed are small cell lung cancers (SCLC). SCLC is defined as ‘a malignant epithelial tumour consisting of small cells with scant cytoplasm, ill-defined cell borders, finely granular nuclear chromatin, and absent or inconspicuous nucleoli’.8 The diagnosis relies on histology and immunohistochemical analysis.8 SCLC is an aggressive neuroendocrine subtype and presents as an extensive disease state with a highly metastatic phenotype. SCLC has a distinct molecular signature, and microarray analyses show very specific gene expression features. Molecular features include identified autocrine growth loops, proto-oncogene activation, and loss or inactivation of tumour-suppressor genes (FHIT, RB1, TP53). EGFR and KRAS signalling genes are rare.9
The majority of cases are diagnosed in elderly patients with a heavy smoking history. Approximately 80% of patients are stage IV at diagnosis, which is associated with poor prognosis and a dismal survival of two to four months without treatment. Prognosis is related to the rapid onset of symptoms due to the intrathoracic lesion, extrapulmonary distant metastases and paraneoplastic syndrome. Conventional chemotherapy with platinum-based agents is often used with etoposide or irinotecan. SCLC is very chemosensitive with good initial response but the challenge with treatment arises from recurrence. Topotecan is often given as second-line therapy in combination with paclitaxel. Maintenance therapy is suggested in the management of SCLC in order to prevent recurrence. Immunotherapy is currently being trialled in SCLC.10
Role of the immune system in lung cancer
Immune evasion is an emerging hallmark of cancer pathogenesis described by Hanahan and Weinberg.11 Immune inflammatory cells are a crucial component of the tumour microenvironment. These cells can have both tumour promoting and antagonising functions.11 Cancer immunoediting theory describes the dynamic role of the immune system ranging from phases of tumour elimination, equilibrium and escape of tumour from the immune response. Tumour cells are eliminated initially by the immune system. The cells that survive then enter the equilibrium phase. The tumour still remains restricted. Further resistance continues and the tumour enters an escape phase. The anti-tumour immune response can be triggered by innate immunity and adaptive immunity.
Recent breakthroughs on the immune system’s role in detecting and eliminating primary and metastasised tumour cells have shifted the focus into the development of immunotherapies to treat cancer patients. The administration of immune system cytokines (IL-2/IFN-α) revealed a sustainable positive response in traditionally immunogenic tumours, such as melanoma and renal cell carcinoma,12, 13 but failed to generate such response in NSCLC, signifying its poor immunogenicity.14,15 Yet, evidence points to the fact that the immune system plays a vital role in lung tumourigenesis and progression. Immunosuppressed patients such as solid organ transplant recipients16,17 and HIV victims18 have increased risk of developing lung cancer compared to the general population. In 1986, a study by Papa et al used mouse models to demonstrate the beneficial effect of adoptive transfer of lymphokine-activated killer (LAK) cells plus low-dose recombinant IL-2 on pulmonary metastases. LAK cells were able to significantly induce tumour regression of multiple histological types with variable immunogenicity including pulmonary metastasised sarcoma, melanoma and colonic adenocarcinoma.19 Tumour-infiltrating lymphocyte functional studies from NSCLC biopsies established the occurrence of cytotoxic activity against autologous tumour cell lines, challenging the idea of lung cancer being non-immunogenic.20
Many recent phase 3 clinical trials attempting to utilise immunological approaches, such as therapeutic vaccination and dendritic cell (DC) activation, have failed in meeting significant therapeutic endpoints in NSCLC patients.21 Nonetheless, they provided evidence that patient test subgroups who underwent simultaneous chemoradiation22 or recently completed chemotherapy23 experienced the most benefit, indicating a synergistic effect of chemoradiotherapy and immunotherapy.
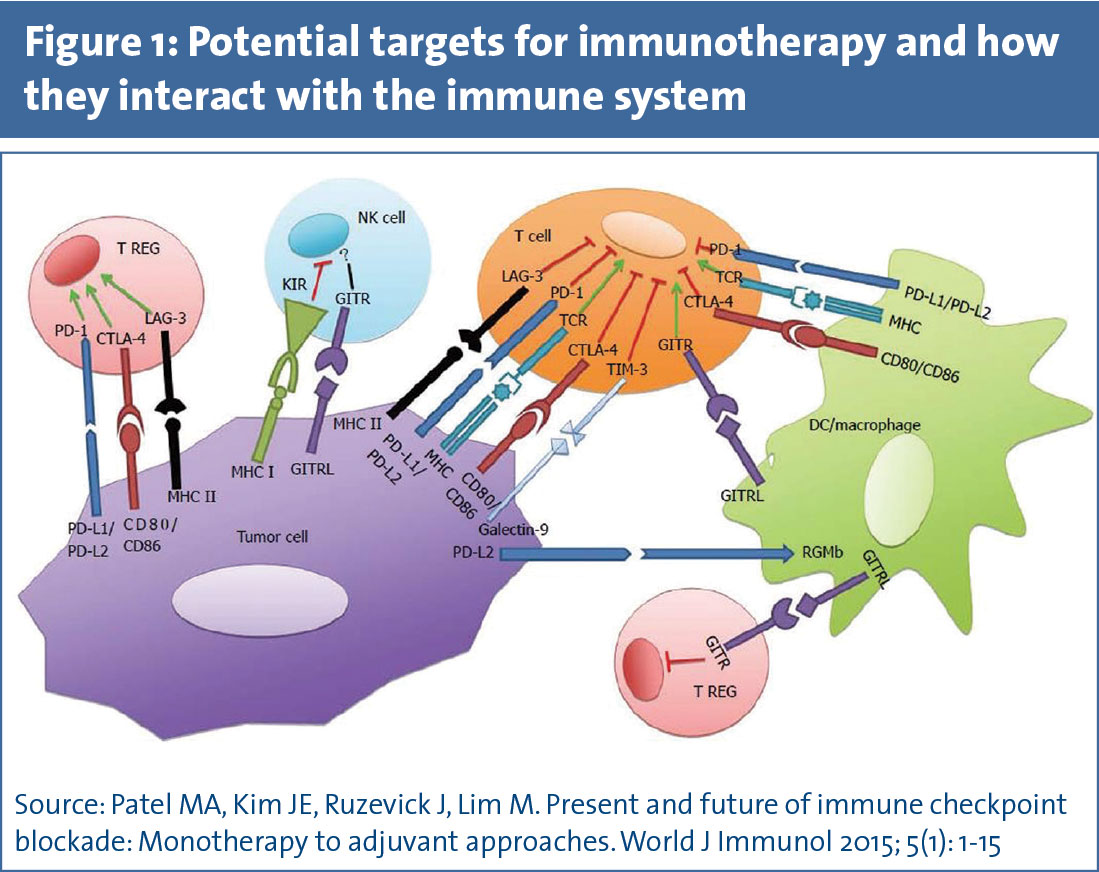
Various cells of the immune system play a role in immunoediting. T cells are considered the most effective in their cytotoxicity towards tumours. T cell response is regulated by several co-simulatory and co-inhibitory signals. The co-inhibitory signals have shown to promote tumour tolerance. The main co-inhibitory signals that have been targeted therapeutically include the checkpoints CTLA-4 and PD-1 (and its ligand PD-L1).
PD-1 is a transmembrane protein that downregulates the activation of T-cells when it engages with its ligand PD-L1 and PD-L2. PD-1 is largely expressed in activated T-cells in the periphery and prevents excess destruction of host tissues during inflammatory response. PD-L1 is constitutively expressed in myeloid cells, professional antigen presenting cells (APCs), lymphoid cells, and cancer cells, while PD-L2 expression is inducible and largely limited to APCs. The structure of PD-1 includes the cytoplasmic structural motifs, immunoreceptor tyrosine-based inhibitor motif and immunoreceptor tyrosine-based switch motif (ITSM); on ligand binding to PD-1, ITSM recruits phosphatases SHP-1 and SHP-2, which are capable of inhibiting downstream kinases that in turn inhibit T-cell proliferation, cytokine release, and cytotoxic function.
PD-1 ligation results in mitigated phosphorylation of the ZAP70/CD3ζ signalosome, resulting in downregulation of the T-cell receptor signalling pathway and subsequent T-cell activation. Finally, PD-1 has been shown to downregulate IFN-γ production as evidenced by relatively increased IFN-γ levels after PD-1/PD-L blockade. IFN-γ is a marker of the Th1 phenotype as well as the activation of effector CD8+ T-cells, and decreased IFN-γ production may reflect a depressed immune response. The overexpression of PD-L1 and PD-1 in lung cancer is a means of immune evasion and can be therapeutically targeted.
CTLA-4 is a co-inhibitory receptor, competing with the co-stimulatory receptor CD28 for their shared ligands B7-1 (CD80) and B7-2 (CD86). By sequestering CD80/CD86, CTLA-4 is capable of inhibiting T-cell receptor (TCR) function while preventing CD28 from binding to its ligands and promoting TCR-mediated T-cell activation. The purpose of CTLA-4 is to check T-cell activation by attenuating T-helper cell activity and up-regulating the immunosuppressive activity of Tregs. Tregs are CD4+ lymphocytes that downregulate immune effector function, typically to prevent autoimmunity. In the tumour micro-environment, cancer cells may upregulate Treg activity through ligand-receptor interactions, leading to the inactivation of effector T-cell responses. CTLA-4 inhibition can be used to upregulate the effector T-cells in tumour immune response.
Other immune checkpoints that could potentially be targeted include LAG-3, TIM-3 and KIR. Co-stimulatory regulators can also be agonised, these include OX 40, GITR and 4-1BB (see Figure 1).24
(click to enlarge)
Role of biomarkers
With the advent of personalised medicine there is emergence of the use of biomarkers for diagnosis, prognosis and treatment response prediction. The current strategies of using immunotherapy as monotherapy or combination therapy shows varying results in different subsets of patients and across different trials. Targeting immune checkpoints can be further defined and stratified by using biomarkers of response. The use of biomarkers has a health economic benefit along with benefits to the patient by preventing any unnecessary morbidity.
PD-1/PD-L1 targeting has shown promising results. Biomarkers of response could direct clinicians in assessing which patients are most likely to benefit from therapy. PD-L1 expression on tumour as a biomarker of response to immunotherapy has shown varied results. However, appropriately characterising tumours via immunohistochemical analysis of PD-L1 expression may help identify patients who would benefit from anti PD1/PD-L1 immunotherapy.25
Several different antibodies exist that can be used to detect PD-L1 by immunohistochemistry as well as fresh frozen plasma samples. The varied antibodies are used in studies and each has its own detection profile. This adds to the challenge of harmonising mode of analysis of PD-L1. Some of these antibodies only stain tumour cells and others also stain tumour-infiltrating immune cells. This makes it difficult to confirm validity of these tests. A meta analysis is required to compare the specificity, sensitivity and the reproducibility of these tests. Another discrepancy among the modalities of testing for PD-L1 exists in assessment of cell-surface PD-L1 versus cytoplasmic PD-L1, the former being most important in tumour and immune cells interactions. There is also a need for standardisation of the definition of PD-L1 positivity. After such methods of analysis can be harmonised there can be a more informed analysis of whether PD-L1 can be used as a predictive biomarker of response to immunotherapy.25
The importance of measuring non-DNA markers (eg. mRNA and proteins) becomes crucial in immuno-oncology (IO), since transcriptional reprogramming, cell-signalling, tumour micro-environment, and protein-protein interactions dominate the immune response. This would lead to the development of multi-analyte-type (mRNA + protein) biomarker signatures to guide cancer immunotherapy. The challenge with this would be analysis of large amounts of data.26
Current immunotherapy and advanced trials
Immune checkpoint anti-PD-1
In March 2015, the US Food and Drug Administration approved nivolumab (immune checkpoint PD-1 inhibitor) as the first immunotherapy agent indicated for recurrent advanced squamous NSCLC patients. Nivolumab binds to and blocks PD-1 hence preventing further inhibition signals to effector T-cells resuming their anti-tumour activity.
Clinical trials of nivolumab include CheckMate-063,27 a phase 2 single-arm trial in 117 patients with advanced stage squamous cell NSCLC still progressing after two or more previous treatment regimens. Median progression-free survival (PFS) and overall survival (OS) were 1.9 and 8.2 months respectively. It was noted that stronger response rates were in subgroups of at least 50% PD-L1 positivity by immunohistochemistry staining. CheckMate-057, a phase 3 trial on non-squamous NSCLC patients, tested the effects of nivolumab versus docetaxel after standard first-line therapy.28 Median OS was 12.2 and 9.4 months (p = 0.002) for nivolumab and docetaxel arms respectively. Survival rates in the nivolumab group after 12 and 18 months were 51% and 39%, respectively, compared to 39% and 23% in the docetaxel group. CheckMate-017, a phase 3 clinical trial, recruited 272 stage IIIB or stage IV squamous cell NSCLC patients who had one previous unsuccessful platinum-based regimen and compared nivolumab with docetaxel.29 Median OS in the nivolumab arm was 9.2 months compared with 6.0 months in docetaxel patients, and a 41% reduced risk of death with nivolumab. Of the patients who received nivolumab, 21% exhibited one-year PFS compared with 6% of patients in the docetaxel arm. Survival rates in the nivolumab group after 12 and 18 months were 42% and 28%, compared with 24% and 13% in the docetaxel group. Adverse events monitoring revealed that nivolumab is better tolerated than docetaxel.
Pembrolizumab also blocks PD-1 pathway via humanised monoclonal IgG4 antibody. It was FDA approved in September 2014, for treatment of metastatic or inoperable melanoma with disease progression after treatment of ipilimumab (see Table 1).30 Initially, evaluated in the phase 1 KEYNOTE-001 trial,31 495 treatment-naïve and treatment-experienced stage IIIB/IV NSCLC patients were recruited. All histological types were included in this study. Higher proportion of treatment-naïve patients responded to therapy (25% vs 18%), increased response duration (23.3 vs 10.4 months) and longer median OS (16.2 vs 9.3 months) compared with treatment experienced patients. No significant difference in response rate between squamous and non-squamous subtypes. Immunohistochemistry staining for PD-L1 revealed a response rate of 45.2% in tumour biopsies with > 50% of cells expressing PD-L1 compared to an overall response rate of 19.4%. Phase 2/3 KEYNOTE-01032 compared pembrolizumab and docetaxel in 1,034 patients with PD-L1+ NSCLC unsuccessfully treated with at least one cycle of platinum-based chemotherapy. Two doses of pembrolizumab were tested, 2mg/kg and 10mg/kg. Longer median OS was demonstrated in the high-dose pembrolizumab arm compared with low-dose and docetaxel (17.3 months vs 14.9 months vs 8.2 months). Positive response was not limited to tumours with > 50% expression of PD-L1 but showed an overall improvement across all test groups. PFS of high-dose, low-dose pembrolizumab and docetaxel were 5.2, 5.0, and 4.1 months, respectively. Currently pembrolizumab is being investigated as first-line treatment for stage IV untreated NSCLC in clinical trials KEYNOTE-024 (NCT02142738) and KEYNOTE-042 (NCT02220894). KEYNOTE-024 published results in November 2016 showing phase 3 trial data of 10.3 months PFS in the pembrolizumab group versus six months in platinum-based therapy group.
PD-1 blockade is in early stage trials for SCLC. Checkmate 032 finished phase 1 trials in which they used dual bloackade of PD-1 and CTLA-4 with nivolumab and ipilimumab. The objective responce rate (ORR) was 10% in the nivolumab-only group and 23% in the combination group.33
Immune checkpoint anti PD-L1
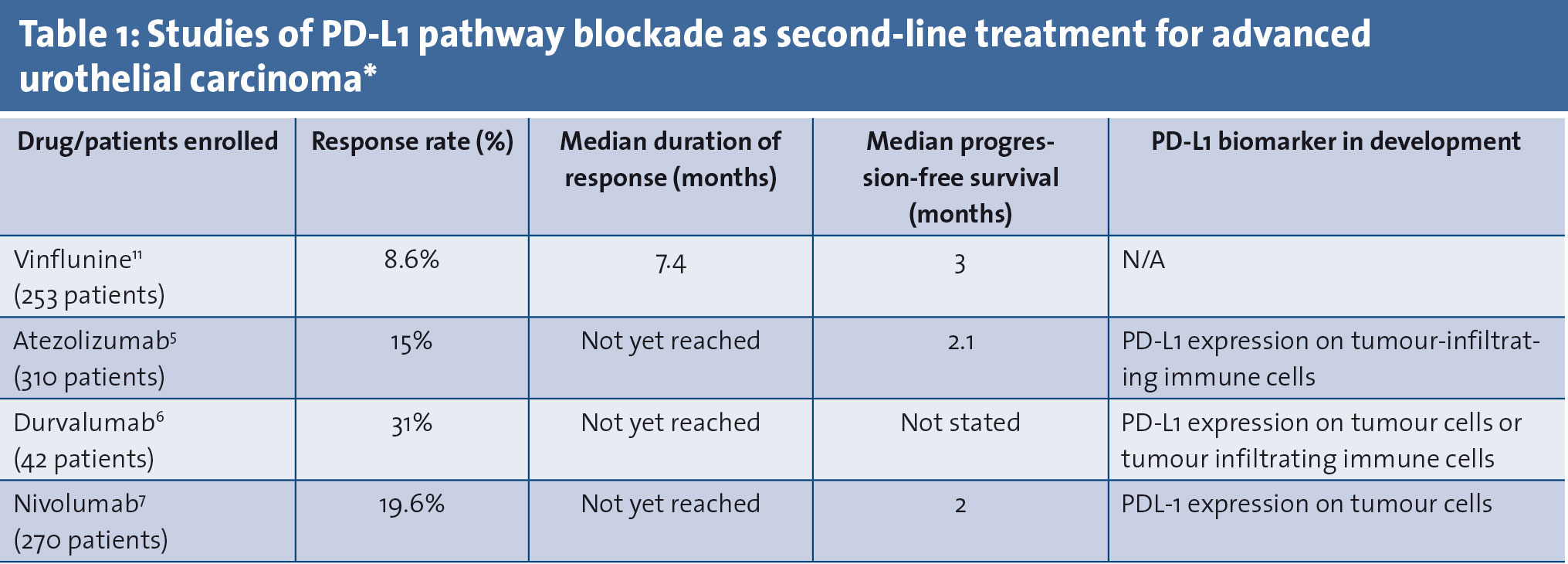
Other drugs that block the PD-1 receptor pathway include ligand blockers: anti PD-L1 antibodies. Atezolizumab (MPDL3280A) is an IgG1 PD-L1-specific antibody that recently underwent a phase 1 trial34 to determine safety, activity and biomarkers of response in 129 aggressively pre-treated advanced NSCLC patients. A dose escalation 1-20mg/kg per three weeks was incorporated in the study, however dose-related toxicities and maximum tolerated dose were not reported, suggesting a positive safety profile. End results were: 45% demonstrated a 24-week PFS and overall response rate of 21%. POPLAR (NCT01903993), a phase 2 trial investigating atezolizumab, recruited 287 NSCLC patients who progressed after previous treatments. Patients were subdivided according to histological type, PD-L1 status and previous therapies later randomised to atezolizumab (n = 144) and docetaxel (n = 143). The atezolizumab arm reported longer OS compared to docetaxel (12.6 months vs 9.7 months). The benefit from atezolizumab was directly correlated with increasing PD-L1 expression on immunohistochemistry. In contrast, there was minimal to no benefit of antibody treatment in patients with the lowest levels of PD-L1. Ongoing atezolizumab trials include: phase 2 trial atezolizumab monotherapy for PD-L1+ NSCLC (NCT01846416) and phase 1 trials investigating combination with VEGF-A inhibitor bevacizumab (NCT01633970), targeted therapy EGFR inhibitor erlotinib (NCT02013219) and MEK inhibitor cobimetinib (NCT01988896).
Immune checkpoint anti-CTLA-4
Ipilimumab, a checkpoint inhibitor, targets the CTLA-4 inhibitory pathway. Blocking CTLA-4 promotes anti-tumour immune response and leads to the depletion of Treg cells preventing Treg-induced tumour-antigen tolerance.35,36 The FDA first approved ipilimumab in 2011 for treating melanomas. Currently ipilimumab is under investigation for NSCLC. A phase 2 randomised trial37 tested the effects of ipilimumab over placebo with combination chemotherapy (carboplatin and paclitaxel) in advanced, untreated NSCLC. Test groups were further divided into concurrent chemoimmunotherapy and phased group (administration of ipilimumab after two cycles of combined chemotherapy). Phased ipilimumab showed most improvement in median OS (12.2 vs 9.7 vs 8.3 months) and overall response rate (32% vs 21% vs 18%) compared with concurrent treatment and placebo. Squamous NSCLC patients experienced the most benefit from phased ipilimumab. The results of this study led to designing a phase 3 testing of combined chemoimmunotherapy in squamous NSCLC (NCT01285609).
Therapeutic vaccines
Not all immunotherapy agents seem as promising as immune checkpoint inhibitors. Other strategies developed include the use of therapeutic vaccines that can theoretically induce the innate immune system to help form a long-lasting adaptive memory against NSCLC tumour cells. Vaccines currently considered for NSCLC are divided into two types: tumour cell vaccines (injection of non-tumourigenic NSCLC whole cells into the patient) and antigen-specific vaccines (injection of tumour specific antigens).
Antigen-specific vaccines include injection of MAGE-A3 (melanoma-associated antigen-A3). MAGE-A3, a tumour-associated antigen of the cancer/testis gene family, is not expressed on normal tissue except the testis and placenta.38 MAGE-A3 is expressed in less than 35% of early-stage and 55% of advanced-stage lung cancer and considered an independent factor of poor prognosis in NSCLC.39, 40 MAGRIT, a phase 3 clinical trial, recruited 2,270 patients with MAGE-A3+ NSCLC after complete resection of the tumour. The placebo-controlled study showed the vaccine was well tolerated but was stopped for not meeting the study’s PFS and OS endpoints.41
Tecemotide is a peptide vaccine for mucin 1 (MUC1) that is expressed in more than 80% of tumour cells and 60% of NSCLC cells.42 High MUC1 expression is associated with tumour metastasis, resistance to chemotherapy and poor outcome.43,44,45 START, a phase 3 double-blind trial, is an international study that recruited 1,513 patients from 33 countries to test tecemotide as maintenance therapy. Patients included had stage 3 unresectable NSCLC that is stabilised after completing chemoradiotherapy. No OS benefit was noted in the tecemotide group compared to placebo.46 START2, a clinical trial of tecemotide, was prematurely terminated due to low probability of reaching its endpoints.47
Whole cell vaccines have not seen much success either in treating NSCLC. Belagenpumatucel-L (Lucanix) and tergenpumatucel-L are whole-cell vaccines based on NSCLC cell lines H460, H520, SKLU-1 and RH2 and transforming growth factor-β (TGF-β) antisense gene via plasmid and transfection respectively.48, 49 Inhibition of TGF-β is of interest due to its association with immunosuppression, tumour progression and metastasis. It is also a poor prognostic factor in patients with NSCLC.50 STOP is a phase 3 trial that investigated belagenpumatucel-L as potential second-line maintenance therapy in stable stage III/IV NSCLC after standard platinum-based chemotherapy. Even though treatment was well tolerated, the study failed to meet its endpoints.50 Tergenpumatucel-L is currently undergoing phase 3 trial (NCT01774578) comparing its efficacy to docetaxel in relapsed or progressed NSCLC patients after treatment with first-line therapy.26
(click to enlarge)
Future immunotherapies in lung cancer
Immunotherapy in lung cancer over the past number of years has been headlined by checkpoint inhibition of PD-1 and CTLA-4. There are also several other checkpoint signalling pathways that can be targeted, which include LAG-3, TIM-3 and KIR.
LAG-3 is a co-inhibitor checkpoint of T-cells. It is co-expressed with PD-1 on tumour infiltrating cells. Anti-LAG-3 and anti-PD-1 antibodies could be combined to decrease tumour growth and enhance antitumour immunity. This has been shown in preclinical models.51 Two anti-LAG-3, BMS-986016 and LAG525, are being tested in phase 1 clinical trials alone and in combination with anti-PD-1 drugs (nivolumab [NCT01968109] and PDR001 [NCT02460224], respectively).
MBG453, an anti-TIM3 antibody, is being studied as a single agent and in combination with PDR001 (NCT02608268). This is another checkpoint-targeted therapy inducing T-cells.
KIR is a molecule in the NK cell that binds HLA molecule to the surface of tumoural cell, inhibiting NK lymphocyte cytotoxic activity against malignant cells. KIR blockade would result in NK cell cytotoxicity towards the tumour. An anti-KIR antibody is being tested with nivolumab in advanced solid tumours (NCT01714739). Lirimumab, also an anti-KIR antibody, is currently in phase 1 trials in NSCLC (NCT01750580).52
Agonistic targeting of co-stimulatory molecules can also be a therapeutic mechanism. CD28, CD27, 4-1BB GITR and OX40 are co-stimulators relevant to T-cells. GITR enhances T-cell function and survival. GITR agonist antibody destabilises intra-tumour Tregs allowing for enhanced cytolysis by CD8+ T cells. TRX518 and MEDI1873 are both anti-GITR antibodies. These are currently in phase 1 trials (NCT01239134, NCT02583165). There are also agonists for 4-1BB and OX40 under early stage trials.53
Novel future strategies in lung cancer immunotherapy
Immunotherapy in lung cancer continues to pose several questions as well as offer several answers. The developing topical areas to consider in lung cancer immunology include immunotherapy to enhance radiotherapy, synergistic targeting immunotherapy, and immunotherapy scheduling as we tackle immunotherapy resistance.
Immunogenic cell death results in the release of pro-inflammatory cytokines. Release of calreticulin and other cytokines during the pre-apoptotic phase of the cancer cell can recruit further immune cells including dendritic cells. These then present the tumour antigen to T-cells. Radiation therapy leads to DNA damage leading to apoptosis, and then causes similar calreticulin exposure and pro-inflammatory cytokine release. This would recruit dendritic cells and then further attract T-cells. This underpins the mechanism of combining radiotherapy with immunotherapy. Given the durable remissions seen with antiPD-1/PD-L1 monoclonal antibody for some patients with NSCLC and the important role played by radiotherapy in the management of NSCLC, it is logical to try to increase response rates and improve outcome by combination approaches.54
Recent trials are targeting multiple checkpoints using a combination of nivolumab and ipilimumab. This is an interesting concept of treatment and requires further investigation. Also similar synergistic effect may be achieved by co-stimulatory agonist therapy simultaneously with checkpoint inhibition. Furthermore, combination of this with radiotherapy may achieve the strongest immune response. The current issues facing this modality of treatment concern toxicity. If antibodies could be designed that simultaneously targeted multiple mechanisms this may lead to a potentially promising solution. Another target of synergistic tackling could be by combining MAPK inhibitors with immunotherapy. Since several tumours show a mutational EGFR, Kras, Alk signature and PD-L1 overexpression, the combination of therapy that targets those mechanisms may be beneficial.55
Several trials are showing an emergence of patients resistant to immunotherapy. This may be due to unspecified inclusion errors, which may be corrected with further use of biomarkers. There is also a key role for cancer stem cells and their interaction with the tumour microenvironment. New drugs that target various mechanisms of cancer stem cells and their interaction with the tumour niche are being developed and studied. There is theoretical benefit in combining stem cell-targeted therapy with immunotherapy to prevent resistance. However, if conventional cytotoxic chemotherapy is also used there may be issues with immunotherapy scheduling. Cytotoxic therapy generally induces an immunosuppressed state, this may render the use of combined immunotherapy pointless.
Conclusion
Immune evasion is a hallmark of cancer. The field of lung cancer is dynamic with new high-impact publications every month. The field is currently showing many promising results in areas such as checkpoint inhibition. The majority of the trials are conducted in advanced cases and face difficulties when devising inclusion and exclusion criteria. There is ongoing advancements in understanding the molecular and genetic signature of an individual patient’s cancer and targeting therapy accordingly. This form of personalised medicine will help the development of appropriate strategies and scheduling of combined therapies. The role of the immune system will remain key. However, it is important to acknowledge that study design and trial execution has significant impact on results and this may be the reason why there is often conflicting data. With an increasing number of immune modulation targets being researched it is beneficial to constantly study and critically analyse the data being published. Informed clinical guidelines need to be devised as expanding data emerges.
References
Siegel R, Ma J, Zou Z, Jemai A. Cancer statistics 2014. CA Cancer J Clin 2014; 64: 9-29
Herbst RS, Heymach JV, Lippman SM. Lung cancer. N Engl J Med 2008; 359: 1367-80
Villaruz LC, Kalyan A, Zarour H, Socinski MA. Immunotherapy in lung cancer. Transl Lung Cancer Res 2014; 3: 2-14
Bobbio A, Alifano M. Immune therapy of non-small cell lung cancer: the future. Pharmacol Res 2015; 99: 217-22.
Datta D, Lahiri B. Preoperative evaluation of patients undergoing lung resection surgery. Chest 2003; 123: 2096-2103
Felip E, Martinez-Marti A, MartinezP, Cet al. Adjuvant treatment of resected non-small cell lung cancer: state of the art and new potential developments. Curr Opin Oncol 2013; 25: 115-120
Berghmans T, Paesmans M, MeertAP, et al. Survival improvement in resectable non-small cell lung cancer with (neo)adjuvant chemotherapy: results of a meta-analysis of the literature. Lung Cancer 2005; 49: 13-23
Travis Wd, Brambilla E, Muller-Hermelink HK, Harris CC, eds. World Health Organisation classification of tumours: pathology and genetics: tumours of the lung, pleura, thymus and heart, vol 10. Lyon; iarc press 2004. http://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb10/bb10-cover.pdf (accessed Dec 1, 2016)
Franklin WF, Nogouchi M, Gonzalez A. Molecular and cellular pathology of lung cancer. In: Pass HI, Carbone DP, Hohnson DH, Minna JD, Scaloitti GV, Turrisis AT, eds. Principles anad practice of lung cancer, 4th edn. Philadelphia, PA: Lippincott Williams & Wilkins 2010: 287-324
Khanert K, Kauffmann-Guerrero D, Huber RM. SCLC – State of the art and what does the future hold in store. Clinical Lung Cancer 2016; 17(5): 325-333
Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell 2011; 144(5): 646-74
Jonasch E, Haluska FG. Interferon in oncological practice: review of interferon biology, clinical applications, andtoxicities. Oncologist 2001; 6: 34-55
Dutcher JP. Current status of interleukin-2 therapy for metastatic renal cell carcinoma and metastatic melanoma. Oncology 2002; 16(11 Suppl13): 4-10
Ridolfi L, Bertetto O, Santo A, et al. Chemotherapy with or without low-dose interleukin-2 in advanced non-small cell lung cancer: results from a phase 1II randomized multicentric trial. IntJOncol 2011; 39: 1011-7
Ardizzoni A, Salvati F, Rosso R, et al. Combination of chemotherapy and recombinant alpha-interferon in advanced non-small cell lung cancer. Multicentric Randomized FONICAP Trial Report. The Italian Lung Cancer Task Force.Cancer 1993; 72: 2929-35
Vajdic CM, van Leeuwen MT. Cancer incidence and risk factors after solid organ transplantation. IntJ Cancer 2009; 125: 1747-54
Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet 2007; 370: 59-67
Sigel K, Wisnivesky J, Gordon K, et al. HIV as an independent risk factor for incident lung cancer. AIDS 2012; 26: 1017-25
Papa MZ, Mule JJ, Rosenberg SA. Antitumor efficacy of lymphokine-activated killer cells and recombinant interleukin 2 in vivo: successful immunotherapy of established pulmonary metastases from weakly immunogenic and nonimmunogenicmurine tumors of three district histological types. Cancer Res 1986; 46: 4973–4978
Tucker ZC, Laguna BA, Moon E, Singhal S. Adjuvant immunotherapy for non-small cell lung cancer. Cancer Treat Rev 2012; 38: 650-61
Pennell NA. Understanding the Rationale for Immunotherapy in Non-Small Cell Lung Cancer. Semin Oncol 2015; 42 Suppl 2: S3-10
Butts C, Socinski MA, Mitchell PL, et al. On behalf of the START Trial Team. Tecemotide (L-BLP25) versus placebo after chemoradiotherapy for stage III non-small-cell lung cancer (START): a randomised, double-blind , phase 3 trial. Lancet Oncol.2014; 15: 59-68
Giaccone G, Bazhenova L, Nemunaitis J, et al. A phase 1II study of belagenpumatucel-L therapeutic tumor cell vaccine for non-small cell lung cancer (NSCLC). Eur J Cancer 2013; 49(Suppl3): Abstract LBA2
Patel MA, et al. Present and future of immune checkpoint blockade: Monotherapy to adjuvant approaches World J Immunol 2015; 5(1): 1-15
Teixido C, et al. Assays for prediciting and monitoring responses to lung cancer immunotherapy. Cancer Boil Med 2015; 12: 87-95
Beechem et al. Biomarker development for cancer immuno-oncology/immunotherapy: Simultaneous digital counting of nucleic acids and proteins at 800-plex. Cancer Immunology Research 2016; 4(1 Supplement): Abstract A013
Rizvi NA, Mazieres J, Planchard D, et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): a phase 2, single-arm trial. Lancet Oncol 2015; 16(3): 257-65
Borghaei H, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer N Engl J Med 2015; 373(17): 1627-39
Brahmer J, Reckamp KL, Baas P, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med 2015; 373(2): 123–35
Barbee MS, Ogunniyi A, Horvat TZ, Dang TO. Current status and future directions of the immune checkpoint inhibitors ipilimumab, pembrolizumab, and nivolumab in oncology. Ann Pharmacother 2015; 49: 907-37
Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the treatment of non-small cell lung cancer. N Engl J Med 2015; 372(21): 2018–28
Herbst RS, Baas P, Kim D-W, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet 2016; 387: 1540-50
Khanna P, Blais N, Gaudreau PO, Corrales-Rodriguez L. Immunotherapy Comes of Age in Lung Cancer. Clin Lung Cancer 2016; pii: S1525-7304(16) 30146-2
Shepherd FA, Douillard JY, Blumenschein GR Jr. Immunotherapy for non-small cell lung cancer: novel approaches to improve patient outcome. J Thorac Oncol 2011; 6: 1763-73
Kono K. Current status of cancer immunotherapy. J Stem Cells Regen Med 2014; 10: 8-13
Lynch TJ, Bondarenko I, Luft A, et al. Ipilimumab in combination with paclitaxel and carboplatin as first-line treatment in stage IIIB/IV non-small-cell lung cancer: results from a randomized, double-blind, multicenter phase 1I study. J Clin Oncol 2012; 30(17): 2046-54
Yang X-N, Huang L, Chen Y, et al. Single nucleotide polymorphisms of MAGEA3 gene and its clinical implications in Chinese patients with non-small cell lung cancer (NSCLC). Chin J Cancer Res 2015; 27: 301-8
Declerck S, Vansteenkiste J. Immunotherapy for lung cancer: ongoing clinical trials. Future Oncol 2014; 10: 91-105
Vasekar M, Liu X, Zheng H, Belani CP. Targeted immunotherapy for non-small cell lung cancer. World J Clin Oncol 2014; 5: 39-47
GlaxoSmithKline press release. Update on phase 1II clinical trial of investigational MAGE-A3 antigen-specific cancer immunotherapeutic in non-small cell lung cancer. April 2014. Available at http://us.gsk.com/en-us/media/press-releases/2014/update-on-phase-iii-clinical-trial-of-investigational-mage-a3-antigen-specificcancer-immunotherapeutic-in-non-small-cell-lung-cancer. Accessed: July 14, 2016.
Villaruz LC, Kalyan A, Zarour H, Socinski MA. Immunotherapy in lung cancer. Transl Lung Cancer Res 2014; 3: 2-14
Declerck S, Vansteenkiste J. Immunotherapy for lung cancer: ongoing clinical trials. Future Oncol 2014; 10: 91-105
Thomas A, Hassan R. Immunotherapies for non-small-cell lung cancer and mesothelioma. Lancet Oncol 2012; 13: e301-10
Freeman-Keller M, Goldman J, Gray J. Vaccine immunotherapy in lung cancer: clinical experience and future directions. Pharmacol Ther 2015; 153: 1-9
Butts C, Socinski MA, Mitchell PL, et al. Tecemotide (L-BLP25) versus placebo after chemoradiotherapy for stage III non-small-cell lung cancer (START): a randomised, double-blind, phase 3 trial. Lancet Oncol 2014; 15: 59-68
Anagnostou VK, Brahmer JR. Cancer immunotherapy: a future paradigm shift in the treatment of non-small cell lung cancer. Clin Cancer Res 2015; 21: 976-84
Nemunaitis J, Nemunaitis M, Senzer N, et al. Phase 1I trial of belagenpumatucel-L, a TGF-beta2 antisense gene modified allogeneic tumor vaccine in advanced non small cell lung cancer (NSCLC) patients. Cancer Gene Ther 2009; 16: 620-4
Anagnostou VK, Brahmer JR. Cancer immunotherapy: a future paradigm shift in the treatment of non-small cell lung cancer. Clin Cancer Res 2015; 21: 976-84
Nemunaitis J, Nemunaitis M, Senzer N, et al. Phase 1I trial of belagenpumatucel-L, a TGF-beta2 antisense gene modified allogeneic tumor vaccine in advanced non small cell lung cancer (NSCLC) patients. Cancer Gene Ther 2009; 16: 620-4
Villaruz LC, Kalyan A, Zarour H, Socinski MA. Immunotherapy in lung cancer. Transl Lung Cancer Res 2014; 3: 2-14
Benson DM Jr, et al. A phase 1 trial on anti-KIR antibody IPH2101 and lenalidomide in patients with relapsed multiple myeloma. Clin Cancer Reseearch 2015; 21: 4055-4061
Wan-Ling Tan, et al. Novel therapeutic targets on the horizon for lung cancer. Lancet Oncol 2016; 17; 347-362
Hanna GG, Illidge T. Radiotherapy and Immunotherapy Combinations in Non-small Cell Lung Cancer: A Promising Future? Clinical Oncology 2016; 28: 726-731
D’Incecco A, et al. PD-L1 and PD-1 expression in NSCLC patients. J Thorac Oncol 2014; 9(6): 741-749
 (click to enlarge)
(click to enlarge)