Irritable bowel syndrome (IBS) is defined by the World Gastroenterology Organisation as a functional bowel disorder in which abdominal pain or discomfort is associated with defecation or a change in bowel habit.
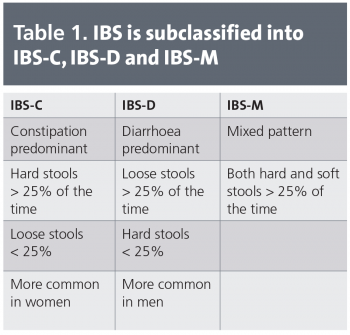
Bloating, distension and disordered defecation are commonly associated features (in some languages, the words ‘bloating’ and ‘distension’ may be represented by the same term).1 It can be subclassified into IBS-C (constipation predominant), IBS-D (diarrhoea predominant) and IBS-M (mixed stool pattern), see Table 1.
Specifically classifying any individual into one of the above groups may not be helpful as many patients will often transition over time between the groups.
Prevalence rates range from 10-15% in European countries and North America. Worldwide the available data suggest that the figure is similar across countries.1 Not only does IBS take its toll on the individual but the cost to the economy is significant as well.
It is estimated that European workers suffering with IBS miss on average 4 to 10.9 days work per year compared to 1.5 to 5.6 days reported by matched controls.2 Productivity is additionally affected as, due to the waxing and waning nature of the symptoms, absenteeism is more sporadic.3
(click to enlarge)
Aetiology and associations
The aetiology of IBS is poorly understood. A complex mix of inherited, environmental and individual characteristics bring about multiple manifestations which constitute the broad symptomatology of IBS.
Inherited
First-degree relatives of IBS sufferers are twice as likely to develop symptoms as the general population.4 However, studies of monozygotic and dizygotic twins have shown that rates of IBS are quite similar.5 This would suggest only a weak genetic link.
Studies show that parental influences are a significant contributory factor in the development of IBS6 and it has been identified that children of IBS patients make more healthcare visits, complain of more gastrointestinal (GI) and non-GI symptoms and have more school absences.7,8
Environmental
There is a very clear association between eating and the onset of symptoms. However, there is little evidence to suggest that IgE-mediated processes play a significant role in the development of IBS symptoms and so true food allergies/hypersensitivities are not seen as a cause of IBS.6
There is evidence to suggest an association between intake of food types known as FODMAPs and the onset of symptoms.
High intake of insoluble fibre has been linked with deterioration in symptoms. Importantly, in some patients soluble fibres such as ispaghula husk can be beneficial. Other food types that may have a detrimental effect include caffeinated drinks, dairy products and fruits.
Post-infectious IBS deserves special mention in that it is thought that between 6-17% of IBS sufferers develop symptoms after an episode of gastroenteritis.9 There is no particular association to any particular pathogen.10
Psychological associations
Previous life stressors and exposure to childhood abuse predispose to the risk of developing IBS in the future.11,12,13 Psychiatric illnesses or anxiety-provoking events preceded the onset of bowel symptoms in two-thirds of IBS patients attending one study in an outpatient setting.14 Additionally, 75% of IBS sufferers report an increase in abdominal pain and altered stool pattern during periods of emotional stress.15
Mechanisms
Many mechanisms have been described which underlie the development of the symptoms of IBS. They include:
Delayed gastric emptying
Exaggerated motor response to meal ingestion
High or low numbers of high-amplitude propagating contractions (HAPCs) in the small bowel
Heightened visceral sensitisation (both peripheral and central)
Central pain-processing abnormalities
Failure of descending inhibitory control within the spine.
Making the diagnosis
Taking an appropriate history and clinical exam is crucial and will usually provide you with the diagnosis of IBS.
There is no need for further investigation if symptoms suggestive of IBS have been present for many years prior to presentation (as most patients will in fact not present and most IBS sufferers are undiagnosed) and there is an absence of red flags (weight loss, rectal bleeding, age > 50, family history of cancer, abnormal physical exam).
The criteria for diagnosis of IBS adopted by the World Gastroenterology Organisation are the Rome III criteria:
Onset of symptoms at least six months before diagnosis
Recurrent abdominal pain or discomfort for > 3 days per month during the past three months
At least two of the following features: improvement with defecation, the association with a change in frequency of stool and/or the association with change in stool form.
Though it is estimated that 96% of sufferers experience bloating16 because it is such a common symptom of many other abdominal and extra-abdominal illnesses, it is not considered in the criteria. However, its presence is supportive of a diagnosis of IBS.
Other symptoms which are common in IBS but do not form part of the diagnostic criteria include feeling of incomplete evacuation, urgency of defecation and altered frequency of defecation.
Patients may often complain of other symptoms such as dyspepsia, heartburn, nausea or non-GI symptoms such as lethargy, headache, insomnia and intolerance to medication.1
With the exception of intermittent abdominal distension, physical exam is normal in IBS. Any abnormality found on physical exam should indicate an alternative diagnosis.
Further investigations
In view of the high prevalence of coeliac disease in Ireland it is worthwhile considering this as a differential. Many patients will have tried a gluten-free diet already and may have put other restrictions on their diet presuming a food allergy. Anti-transglutaminase (TTG) and anti-endomysial (EMA) antibodies are helpful but the gold standard for diagnosis is a jejunal biopsy.
Lactose intolerance is another consideration, especially in those of African origin. A simple test is to have the patient drink a pint of skimmed milk (which has approximately 25g of lactose). If the patient has lactose intolerance they should experience onset of symptoms.
Small-intestinal bacterial overgrowth or colitis are among other GI considerations.
Gynaecological considerations and symptoms of any comorbidity should also be considered. Any red-flag symptoms should be investigated and referral to a specialist may be required.
Clinical management
Having established a diagnosis of IBS it is important to note that there are many treatment options available for the safe and effective management of the condition. Once a patient understands their condition they can effectively control it, leading to improvement of their symptoms.
Dietary and lifestyle
Much of the treatment of IBS can be carried out as ‘self-help’6 and patients should be encouraged to take control of and monitor their condition. As the symptoms of IBS are often worsened by eating, many patients conclude that they are suffering from a food ‘allergy’.17
While there is little or no evidence to support this conclusion, investigations may be carried out in the form of an exclusion diet followed by serial reintroduction of individual foods.18
A type of elimination diet which has become popular in the treatment of IBS is called the low FODMAPs diet. FODMAP is an acronym for fermentable oligo-, di- and mono-saccharides and polyols. They are short-chain carbohydrates which are poorly absorbed from the small bowel and can result in many of the symptoms of IBS.
They include fructans and galactans, polyols, fructose and lactose. Foods known to contain FODMAPs are restricted for six-to-eight weeks and are then reintroduced in the form of ‘food challenges’.
Progress is reviewed throughout the diet and many patients can return to a normal diet after six-to-eight weeks with certain high FODMAP-containing foods restricted (for more information see Gibson and Shepherd).19
Patients should also be advised of the importance of eating regular meals, taking the time to eat, drinking plenty of non-caffeinated fluids, restricting caffeinated drinks, reducing intake of alcohol and high-fibre food.
Regular exercise also plays an important role in the management of IBS.
Pharmacological therapy
There are many pharmacological interventions available for the treatment of IBS. The selection and objective of the pharmacological agent will depend on the predominant symptoms being experienced by the patient.
It is worth noting here that the placebo effect has resulted in positive responses of up to 50% in IBS trials20 and healthcare professionals should be both aware of and manipulating this effect.21
Antispasmodic agents
The aim of using antispasmodic agents is to attenuate the heightened baseline and postprandial contractility seen in patients with IBS, especially those experiencing diarrhoea-predominant IBS.22
Common choices include mebeverine (135mg tid) or hyoscine (10-20mg qid).
Fibre and laxatives
Ispaghula husk is commonly used in the treatment of IBS-C. It acts to increase faecal mass and results in accelerated gut transit. Care must be taken, however, as many patients will complain that their symptoms are exacerbated by fibre.
Osmotic laxatives can be used to treat constipation and have been found to be well tolerated and effective in chronic constipation23 but whether this extends to IBS-C is unclear.
Antidiarrhoeal agents
The opioid analogue loperamide is commonly used to treat diarrhoea. It inhibits presynaptic receptors in the enteric nervous system resulting in inhibition of peristalsis and secretion.6
Loperamide is given at a 4mg stat dose followed by 2mg after each loose bowel motion, to a maximum of 10mg daily. Codeine phosphate is not commonly used due to the side-effects of dependence, nausea and drowsiness.
Antidepressants
Tricyclic antidepressants (TCAs) have been used to treat IBS but their anticholinergic side-effects (dry mouth, blurred vision, fatigue) have often resulted in poor compliance among patients. It has also been difficult to establish a clear evidence base for their use in IBS; however, in those who can tolerate the drug there can be benefit seen.24
Selective serotonin reuptake inhibitors (SSRIs) show more promise in the treatment of IBS. In one large randomised controlled trial it was found that a standard dose of an SSRI led to significant improvement of health-related quality of life in patients with chronic or treatment-resistant IBS.25
Psychological treatment
It is recommended that referral for psychological interventions including cognitive behavioural therapy, hypnotherapy and/or psychological therapy should be considered for patients who do not respond to pharmacological treatments after 12 months and who develop refractory IBS.17
Cognitive behavioural therapy (CBT) involves identifying the triggers for symptom exacerbation, understanding the patient’s response to symptoms and teaching adaptive ways of responding.6 However, its use and evidence for its use in IBS treatment is controversial.
Research has been carried out to establish how hypnotherapy may result in alleviation of IBS symptoms. It can mediate an improvement by normalising visceral sensation,26 reducing colonic contractions27 and reversing the patient’s negative feelings about their IBS.27 The American Psychological Association guidelines outline that hypnotherapy was the most accepted psychological treatment for IBS based on effectiveness and specificity.6
Summary
IBS is a common and complex syndrome. Therapeutic decisions can be frustrating for the clinician but not nearly as frustrating as the impact the symptoms have on the quality of life of the patient.
References
World Gastroenterology Organisation Global Guideline. April 2009. Irritable Bowel Syndrome: a Global Perspective.
Hungin AP, Chang L, Barghout V, Kahler K. The impact of IBS on absenteeism and work productivity: United States and eight European countries. Presented at: 68th Annual Meeting of the American College of Gastroenterology; October 13-15, 2003; Baltimore, Md.
Dean BB, Aguilar D, Barghout V et al. Impairment in work productivity and health-related quality of life in patients with irritable bowel syndrome. Am J Manag Care 2005; 11: S17-S26
Davidson M, Waserman R. The irritable colon of childhood (chronic non specific diarrhea syndrome). J Pediatr 1966; 69: 1027-1038
Mohammed I, Cherkas LF, Riley SA et al. Genetic Influences in irritable bowel syndrome: a twin study. Am J Gastroenterol 2005; 100: 1340-1344
Spiller R, Aziz Q, Rubin G et al. Guidelines on the irritable bowel syndrome: mechanisms and practical management. Gut 2007; 56: 1770-1798
Levy RL, Whitehead WE, Von Korff MR et al. Intergenerational transmission of gastrointestinal illness behaviour. Am J Gastroenterol 2000; 95: 451-456
Levy RL, Whitehead WE, Walker LS et al. Increased somatic complaints and health care utilization in children: effects of parents IBS status and parents response to gastrointestinal symptoms. Am J Gastroenterol 2004; 99: 2442-2451
Houghton LA, Whorwell PJ. Toward s a better understanding of abdominal bloating and distension in functional gastrointestinal disorders. Neurogastroenterol Motil 2005; 17: 500-511
Longstreth GF, Hawkey CJ, Mayer EA et al. Characteristics of patients with irritable bowel syndrome recruited from three sources: implications for clinical trials. Aliment Pharmacol Ther 2001; 15: 959-964
Creed F, Craig T, Farmer R. Functional Abdominal pain, psychiatric illness and life events. Gut 1988; 29: 235-242
Dinan TG, O’Keane V, O’Boyle C et al. A comparison of the mental status, personality profiles and life events of patients with irritable bowel syndrome and peptic ulcer disease. Acta Psychiatr Scand 1991; 84: 26-28
Howell S, Poulton R, Talley NJ. The natural history of childhood abdominal pain and its association with adult irritable bowel syndrome: birth-cohort study. Am J Gastroenterol 2005; 100: 2071-2078
Ford MJ, Miller PMC, Eastwood J, et al. Life events, psychiatric illness and the irritable bowel syndrome. Gut 1987; 28: 160-165
Drossman DA, Sandler RS, McKee DC et al. Bowel Patterns among subjects not seeking health care, Use of a questionnaire to identify a population with bowel dysfunction. Gastroenterology 1982; 83: 529-534
Neal KR, Hebden J, Spiller R. Prevalence of gastrointestinal symptoms six months after bacterial gastroenteritis and risk factors for development of the irritable bowel syndrome: a postal survey of patients. BMJ 1997; 314: 779-782
NICE clinical guideline 61
Jones VA, Shorthouse M, Hunter JO. Food Intolerance: A major factor in the pathogenesis of irritable syndrome. Lancet 1982 ;2: 1115-1117
Gibson PR, Shepherd SA. Evidence based dietary management of functional gastrointestinal symptoms: The FODMAP approach. JGHF 2010; 25: 252-258
Spiller RC, Problems and challenges in the design of irritable bowel syndrome clinical trials: experience from published trials. Am J Med 1999; 107: 91-7S
Enck P, Klosterhalfen S. The placebo response in functional bowel disorders: perspectives and putative mechanisms. Neurogastroenterol Motil 2005; 17: 325-331
Chey WY, Jin HO, Lee MH et al. Colonic motility abnormality in patients with irritable bowel syndrome exhibiting abdominal pain and diarrhea. Am J Gastroenterol 2001; 96: 1499-506
Attar A, Lemann M, Ferguson A et al. Comparison of a low dose polyethylene glycol electrolyte solution with lactulose for treatment of chronic constipation. Gut 1999; 44: 226-230
Drossman DA, Toner BB, Whitehead WE et al. Cognitive behavioural therapy versus education and desipramine versus placebo for moderate to severe functional bowel disorders. Gastroenterology 2003: 125:19-31
Vernia P, Riccardi MR, Frandina C et al. Lactose malabsorption and irritable bowel syndrome. Effect of a long term lactose-free diet. It J Gastroenterol 1995; 27: 117-121
Whorwell PJ, Houghton LA, Taylor EE et al. Physiological effects of emotion: Assessment via hypnosis. Lancet 1992; 340: 69-72
Gonsalkorale WM, Toner BB, Whorwell PJ et al. Cognitive change in patients undergoing hypnotherapy for irritable bowel syndrome. J Psychosom Res 2004; 56: 271-278
 (click to enlarge)
(click to enlarge)