The demographics and modes of diagnosing diverticulitis are assessed by
Prof Gerry O’Sullivan and colleagues using investigative methods
Mr M Sufian Khalid, Surgical Tutor/registrar, Mercy University Hospital, Cork, Mr A Wahid Khan, Surgical Tutor/registrar, Mercy University Hospital, Cork, Mr Akbar Achakzai, Surgical Tutor/registrar, Mercy University Hospital, Cork, Mr Michael O'Riordain, Consultant in Surgery and Gastroenterology, Mercy University Hospital, Cork, Mr Muhammed Naeem, Consultant Surgeon, Mercy University Hospital, Cork and Prof Gerry O'Sullivan, Consultant Surgeon, Mercy University Hospital, Cork
The presentation, investigations and management of diverticular disease are diverse. Our objectives were to retrospectively assess the demographics of the disease, alongside the mode of presentation, investigative methods and management, and then to propose recommendations regarding appropriate diagnostic and therapeutic strategies supported by current best available practice.
Methods
From June 2005 to June 2007, all patients with the diagnosis of diverticular disease were reviewed retrospectively. The diagnosis may have been performed either by colonoscopy, radiology or intra-operatively. Patients were assessed as to age, sex, presenting symptoms, diagnostic method and extent of disease, management and outcome.
Introduction
Colonic diverticulosis was first mentioned by Alexis Littré (a French surgeon) in the 17th century, although in the medical literature it was first described in 1920.1 Over the course of time the prevalence of diverticular disease has increased in developed countries. Therefore it has been termed a disease of Western civilisation.2
Diverticular disease affects 50% of the population over the age of 60 years in the US, Europe and Australia.3 The exact incidence is not known but the incidence increases as the population ages.4 There is no apparent gender-specific predilection.
Most people with diverticular disease remain asymptomatic,5 and only 10-20% develop symptoms and need admission.6 Of these, 15% will develop significant complications7 and of the latter only 1-2% of these patients require surgery.8 Complications can arise from the perforation of a diverticulum either at a microscopic or a macroscopic level.9 The clinical manifestation of this event will depend on a number of factors, including the size of the perforation, the level of extra-colonic contamination and the body’s ability to contain this contamination. The clinical features of perforation range from peridiverticulitis and small pericolic abscesses to large intra-abdominal or pelvic abscesses and purulent or faecal peritonitis. The significance of perforated diverticular disease lies in the marked mortality associated with the severe manifestation of the condition. Most large-case series show an overall mortality rate for patients requiring operative intervention of 12-36% concomitant with a considerable morbidity rate.10,11
One of the aims of the study is to assess retrospectively the safety of colonoscopy in patients with acute diverticulitis. This study has been approved by the Institutional Medical Ethics Committee.
Patients and methods
A retrospective review of 305 patients who were admitted to the Mercy University Hospital, Cork, with a diagnosis of a diverticular disease was undertaken between June 2005 and June 2007. The diagnosis was made either in the day ward or general surgical ward between their admission and their hospital discharge. We used clinical, radiological, endoscopical and pathological data in computerised form. A single investigator reviewed all records to reduce interpretative errors.
A pro forma was collated with 15 different characteristics for each case, including patient demographics, clinical presentation, significant past medical and surgical history, investigations performed and types of treatment undergone. If surgery had been performed, the type of procedure, either open or laparoscopic, along with its outcome, was noted. We also assessed whether stoma was created or not, and what the final pathology revealed. In addition, mortality, morbidity and length of stay were recorded.
Results
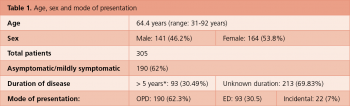
The mean age of all patients was 64.4 years, a median of 66 and mode of 75. The range was 31-92 years. Of those patients who took part, 164 (53.8%) were females and 141 (46.2%) were males. Six (2%) patients were below 40 years of age. Of 305 cases in total, 93 (30%) with a course of the disease of more than five years were first diagnosed as diverticular disease either through a colonoscopy or radiologically.
Some 190 (62.3%) patients who presented in the outpatient department (OPD) were booked as day cases for a colonoscopy and barium enema. Ninety-three cases (30.5%) were admitted through the emergency department (ED) and were clinically diagnosed with diverticular disease or diverticulitis, which was later confirmed radiologically, endoscopically and intra-operatively. While being investigated for conditions other than bowel problems, 22 cases (7%) were diagnosed with diverticular disease incidentally.
The most common patient presentation was abdominal pain.
At the time of presentation, the mean duration of symptoms was 14 days (ranging between one and 180 days). Ninety-two cases (30%) displayed more than two symptoms. Of 305 patients, 16 (5.2%) had a family history of bowel cancer. Ten patients were on non-steroidal anti-inflammatory drugs (NSAIDs)/steroids.
In this study, 260 patients (85%) had a colonoscopy carried out. The findings on colonoscopy were:
Diverticulosis in 191 cases (73.5%)
Associated polyps in 80 (26%)
Acute diverticulitis in 34 (13%)
Associated colitis in 21 (8%)
Stricture in 10 (3.8%)
Bowel cancer in four (1.5%).
A barium enema was performed in 49 patients (16.1%). Undoubtedly, a barium enema provides good information on the number and location of colonic diverticula, albeit with an error factor of up to 25% on the reporting of barium enema.12 Therefore, 10% of patients who were classified high-risk and had a positive family history had a colonoscopy later. The authors recommend a routine colonoscopy in all patients with symptomatic diverticular disease, particularly to exclude bowel cancer.
Six of the cases (< 2%) had small bowel studies. This investigation yields very little in patients with diverticular disease. A CT scan was performed in 64 patients (21%) with the following findings:
Abscess in 18 (28%)
Diverticulitis in 20 (31.25%)
Free air in 12 (18.75%)
Diverticulosis in eight (12.5%)
Fistula in five (7.8%).
*At first presentation/diagnosis in chart(click to enlarge)
(click to enlarge)
Left-sided diverticular disease
In this study, 266 patients (87.2%) had left-sided diverticular disease predominantly involving the sigmoid colon. Only two (< 1%) presented with right-sided diverticular disease. Right-sided diverticular disease is commonly congenital and often gets confused with acute appendicitis.13 It is common in Asians but rare in Caucasians.14 Thirty-six (11%) were diagnosed as pan-diverticular disease while one patient had a diverticular disease also of the small bowel (jejunum).
In our series, 190 of the patients (62%) with anatomic diverticular disease remained asymptomatic or mildly symptomatic. The most common clinical complication of patients with diverticular disease was diverticulitis in 53 cases (17.4%). Common presentations included pain in the left lower quadrant associated with a change in bowel habits in the form of either diarrhoea or constipation.
The second most common complication of diverticular disease was an abscess formation. Twenty-two patients (7.2%) presented with a diverticular abscess and eight with a free perforation into the peritoneum. In this context it should be mentioned that 10 patients were on NSAIDs/steroids, which are contributing risk factors for diverticular perforation.15
An abscess formation occurs as a result of a micro or macro perforation which can lead to either a confined pericolic abscess or to faecal peritonitis. Hinchey et al described a grading system reflecting the degree of perforation. In our series, six patients showed a Hinchey type 1 abscess (see Table 4). Another important endoscopic complication of segmental colitis associated with diverticular disease (SCAD) was seen in 21 patients (6%). In these patients the mucosa between diverticula was abnormal, ie. erythematous, granular and friable, similar to colonic mucosa in inflammatory bowel disease.16
Six patients showed strictures during colonoscopic examination. In this study, five cases (2%) had fistula (three colovesical, one colovaginal and one coloenteric); of these, two patients presented in the ED with pneumaturia. Most patients with a relatively mild form of diverticular disease responded well to conservative management. Patients were advised to adopt a high-fibre diet (vegetables, bran, bread, juices and one to two litres of water every day).
A large US cohort study proved that a high-fibre diet helps to control diverticular disease and to protect against a perforation by increasing stool weight and water content, thus reducing colonic segment pressure and transit time.17 Selected patients with query mild diverticulitis, but with good oral intake and a supportive social structure, were treated as outpatients with broad-spectrum oral antibiotics. Some 93 patients presented in the ED with severe or complicated diverticular disease. Of these, 53 were diagnosed with acute diverticulitis and hospitalised. They were treated with bowel being rested with clear fluid or nil by mouth.
(click to enlarge)
Recommended combination
The recommended combination regimen18 of metronidazole, augmentin (ampicillin + clavulanic acid) with or without an aminoglycoside (gentamicin) were initiated. In case of improvement, patients were discharged and were advised to complete a course of antibiotics for seven to 10 days.
Forty patients presented in the ED with a complicated diverticular disease, ie. generalised peritonitis, perforation, abscess, bleeding or colonic obstruction. They underwent various surgical interventions. In six patients with localised abscess (Hinchey stage I) a CT-guided drainage was performed. One failure was observed with CT-guided procedure. This patient, along with four others, was offered laparoscopic lavage, employed to drain multiple abscesses.
A good outcome was observed in the patients who had undergone this minimally invasive procedure.
(click to enlarge)
Discussion
This study documents the experience of a large single institution with the epidemiology and management of colonic diverticular disease in 305 patients. In addition, the study also highlights the issue of safety of colonoscopic procedure in patients with incidental endoscopic findings of acute diverticulitis.
In this study the incidence of diverticular disease is slightly higher in females than in males (53.8: 46.2). Young patients under 40 years of age made up only 2% of the total number. Most people with diverticular disease remained asymptomatic. Only 20-30% developed symptoms, of which 11% developed significant complications.
These patients with various complications underwent surgical intervention with an overall mortality and morbidity rate of less than 2%. These statistics are comparable with other retrospective and prospective reports discussed in the medical literature.19,20
The large majority of patients with diverticulosis remain asymptomatic. There are no data available to support any therapeutic recommendations or routine follow-up for these patients.21
Patients usually come to clinical attention because of non-specific abdominal complaints and are only subsequently found to have diverticulosis. Most patients (in this study 51%) present with abdominal pain, typically in the lower abdomen and more frequently, but not invariably, left-sided.
By definition these patients do not manifest signs of inflammation such as pyrexia or leukocytosis which might indicate diverticulosis. Patients may also report other symptoms of colonic dysfunction, including bloating, constipation, diarrhoea or the passage of mucus.
Consider alternative diagnoses
One must carefully consider alternative diagnoses before attributing the symptoms solely to diverticulosis. These non-specific symptoms obviously overlap considerably with those of IBS and IBD. In a patient with non-specific symptoms of colonic dysfunction, the demonstration of diverticula either radiologically or colonoscopically adds little to the diagnostic probabilities and management because of a high prevalence of these findings in the general population. In addition, the question why certain patients with diverticula experience symptoms and others do not remains a mystery.22 Complications of a diverticular disease have generally been associated with advancing age.
However, many authors suggest that acute diverticulitis is more virulent in young patients under 40 years of age. In our study, most patients were elderly. Only six (less than 2%) of the patients who developed significant complications were young, which is also in accordance with the literature.23 Various therapeutic strategies exist for the management of acute complicated diverticulitis. Small abscesses do not require drainage. Most of these regress with antibiotics.24 A CT-guided percutaneous drainage in conjunction with adequate antibiotic cover is the standard treatment for a peridiverticular abscess (HIN I) which is more than 5cm in diameter.25 The advantage is the rapid control of sepsis and patient stabilisation without a need for general anaesthetics.
The indications26 for emergency colonic resection include generalised peritonitis, uncontrolled sepsis, visceral perforation, acute clinical deterioration and colonic obstruction. The optimal surgical approach to complicated diverticular disease remains controversial.27
Hartmann procedure
We performed 16 sigmoid colectomies followed by a primary anastomosis with or without a protective colostomy. Out of 16 patients, 10 had an open resection and six underwent laparoscopic-assisted sigmoid colectomies. Of the 16, six patients were offered a transverse loop colostomy and one had a loop ileostomy. Currently, resection anastomosis with or without colostomy has become the gold standard with the lowest associated mortality and morbidity rates.32
The question of whether or not to perform primary anastomosis needs to be addressed by a large randomised trial with a proper risk stratification of patients. Most recently, the laparoscopic approach for sigmoid resection for selected groups of patients with diverticulitis has been advocated.33 Compared to open procedure it has important short-term advantages with fewer complications, a short hospital stay and faster recovery,34 besides avoiding midline laparotomy and a protective stoma.35
In cases of Hinchey II or III diverticulitis where there is either localised or free intra-abdominal pus present, a limited laparoscopic procedure in terms of lavage and drainage of the abdominal cavity without bowel resection or stoma formation is recommended. Once the acute inflammation has settled a delayed definitive laparoscopic procedure is performed, thereby completing the totally invasive management for such patients.36 On the other hand, the laparoscopic approach for emergency resection remains controversial because of the associated significant conversion rate of 38-84%,37 as there is a risk of early reoperation if the initial intervention fails to control the abdominal sepsis.
Previously the presence of diverticulosis was felt to be a relative contraindication for a colonoscopic procedure for fear of an increased likelihood of perforation.38-40 By this approach a definite colonic resection is performed in a non-emergency situation. In our series we successfully performed six sigmoid colectomies with good results.
Conclusion
This study has documented the relative safety of colonoscopy in patients with acute diverticulitis. Out of 260 patients, 34 (11%) had an incidental finding of acute diverticular disease (erythema, oedema, a submucosal bulge or pus emanating from a diverticular orifice),41 which raised the possibility of unrecognised diverticulitis, especially in patients with abdominal pain. To our knowledge this is the first study with the highest number of patients (34, ie. 11%) who have undergone a colonoscopy for unsuspected diverticulitis and in whom the diagnosis was based on colonoscopic findings. To date, only two other studies have reported the use of colonoscopy for diagnostic purposes in acute diverticulitis.42,43 No doubt the diverticular colon may be difficult to examine colonoscopically because of spasm, but also because of a confusion between luminal and diverticular openings.44 The use of a smaller diameter colonoscope may be helpful in this situation.45,46
The results show that colonoscopy performed by experienced people is safe in patients without clinical acute diverticulitis, but who have been found to have diverticular inflammation. However, further prospective studies are necessary to determine the safety of colonoscopy in patients with uncomplicated diverticulitis.
References
Telling WHM. Discussion on diverticulitis. Proc R Soc Med 1920; 13: 55-64
Painter NS, Burkitt DP. Diverticular disease of the colon, a 20th century problem. Clin Gastroenterol 1975; 4: 3-21
Huihui Y, Losada M al. Diverticulosis coli – update on a “Western” disease. Adv Anat Pathol 2005; 12: 74-80
Watters DA, Smith AN et al. Mechanical Properties of the colon: comparison of the features of the African and European colon in vitro. Gut 1985; 26: 384-392
Morris CR, Harvey IM et al. Epidemiology of perforated colonic diverticular disease. Postgraduate Medical Journal 2002; 78: 654-658
Ryan P. Two kinds of diverticular disease. Annals of the Royal college of Surgeons of England 1991; 73: 249-261
Parks TG. Natural history of diverticular disease of the colon. Clin Gastroenterol 1975; 4: 53-69
Roberts Pl, Veidenheimer MC. Current management of diverticulitis. Adv Surg 1994; 27: 189-208
Wong WD, Wexner SD, Lowry A et al. Practice parameters for the treatment of sigmoid diverticulitis - supporting documentation. The Standards Task Force. The American Society of Colon and Rectal Surgeons. Dis Colon Rectum 2000; 43: 290-297
Elliott TB, Yego S, Irvin TT. Five- year audit of the acute complications of diverticular disease. Br J Surgery 1997; 84: 535-539
Corder AP, William JD et al. Optical operative treatment in acute septic complications of diverticular disease. Ann R Coll Surgery Eng 1990; 72: 82-6.
Stollman NH, Raskin JB et al. Diagnosis and management of diverticular disease of the colon in adults 1999; 94: 3110-3121
Wong SK, Ho YH, Leong AP et al. Clinical behaviour of complicated right sided and left sided diverticulosis. Dis Colon Rectum 1997; 40: 344-348
Beranbaum SL, Zausner J, Lane B. Diverticular disease of the right colon. AJR Am J Roentgerol 1972; 115: 334-348
Aldoori WH, Giovannucci EL, Rimm EB et al. A prospective study of diet and the risk of symptomatic diverticular disease in men. Am J Clin Nutr 1994; 60: 757-764
Harpaz N, Sachar DB. Segmental colitis associated with diverticular disease and other IBD look-alikes. J Clin Gastroenterol 2006; 40(3): S132-S135
Morris CR, Harvey IM et al. Epidemiology of perforated colonic diverticular disease. Postgrad Med J 2002; 78: 654-658
Chow AW. Appendicitis and diverticulitis. In: Hoeprich PD,Jordan MC et al. Infectious disease: A treatise of infectious processes. Philadelphia: JB Lippincott 1994; 878-881
Boulos PB. Complicated diverticulosis. Best Practice and Research Clinical Gastroenterology 2002; 16: 649-662
Berry AR, Tumer WH et al. Emergency surgery for complicated diverticular disease. A five year experience. Dise Colon Rectum 1989; 32: 849-854
Simpson J, Scholefield JH et al. Pathogenesis of colonic diverticula. Br J Surg 2002; 89: 546-554
West SD, Robinson EK, Delu AN et al. Diverticulitis in younger patients. The Am J Surg 2003; 186: 743-746
Ambrosetti P, Robert J, Witzig JA et al. Incidence, outcome and proposed management of isolated abscesses complicating acute left-sided colonic diverticulitis: A prospective study of 140 patients. Dis Colon Rectum 1992; 35: 1072-1076
Stabile BE, Paccio E, Van Sonnenberg E et al. Prospective percutaneous drainage of diverticular abscess. American Journal of Surgery 1990; 99-105
Kaiser AM, Jiang J-K et al. The management of complicated diverticulitis and the role of computed tomography. Am J Gastroenterol 2005; 100: 910-917
Abcarian H, Pearl RK. A safe technique for resection of perforated sigmoid diverticulitis. Dis Colon Rectum 1990; 33: 905-906
Mutter D, Bouras G, Forgione A et al. Two-stage totally minimally invasive approach for acute complicated diverticulitis. Colorect Dis 2006; 8: 501-505
Pearce NW, Scot SD, Karran SJ. Timing and method of reversal of Hartman’s procedure. Br J Surg 1992; 79: 839-841
Desai DC, Brennan EJ Jr, Reilly JF et al. The utility of Hartman’s procedure. Am J Surg 1998; 175: 152-154
Anil M, Kathy S et al. Spectrum of disease and outcome of complicated diverticular disease. Am J Surg 2003; 186: 696-701
Scheidbach H, Scheider C, Rose J et al. Laparoscopic approach to treatment of sigmoid diverticulitis: Changes in the spectrum of indications and results of a prospective, multicentre study on 1,545 patients. Dis Colon Rectum 2004; 47: 1883-1888
Dwivedi A, Chahin F, Agrawa S et al. Laparoscopic colectomy vs open colectomy for sigmoid diverticular disease. Dis Colon Rectum 2002; 45: 1309-1315
Scheidbach H, Schneider C, Rose J et al. Laparoscopic approach to treatment of sigmoid diverticulitis: changes in the spectrum of indications and results of a prospective, multicentre study on 1,545 patients. Dis Colon Rectum 2004; 47: 1883-1887
Gonzalez R,Smith CD,Matter SG, et al. Laparoscopic vs open resection for treatment of diverticular disease. Surg Endosc 2004; 18: 276-280
SSAT Patient Care Guidelines. Surgical Treatment of Diverticulitis Board Approved 10/08/07
Douglas K. Rex, MD et al .New Guidelines for Evaluating and Managing Diverticulitis. [Clinical Practice Guideline Watch] Gastroenterology August 18, 2006.
Ferozoco LB, Raptopoulos V, Silon W. Acute diverticulitis. N Engl J Med 1998; 338: 1521-1526
Goldstein NS, Ahmad E. Histology of the mucosa in sigmoid colon specimens with diverticuar disease. Observation for the interpretation of sigmoid colonoscopic biopsy specimens. Am J Clin Path 1997; 107: 438-444
Ghorai S, Thomas M et al Endoscopic findings of Diverticular Inflammation in colonoscopy patients without clinical acute diverticulitis: Prevalence and Endoscpic Spectrum. Am J Gastroenterol 2003; 98: 802-809
Lee JG, Joseph W et al. Colonoscopic diagnosis of unsuspected diverticulosis. (American Society for) Gastrointestinal Endoscopy 2002; 55(6): 746-748
William CB, Saunders BP. Technique of colonoscopy. In: Raskin JB,Nora HJ, eds. Colonoscopy: principles and techniques. New York: Igaku-Shoin Medical Publishers Inc 1995: 12-42
Kozark RA, Botoman VA, Patterson DJ. Prospective evaluation of a small calibre upper endoscope for colonoscopyafter unsuccessful standard examination. Gastrointest Endosc 1989; 35: 333-335
 *At first presentation/diagnosis in chart(click to enlarge)
*At first presentation/diagnosis in chart(click to enlarge)


