OBSTETRICS/GYNAECOLOGY
Labour hopscotch: Supporting physiological births
Maternity care has consistently become more medicalised with women in Ireland more likely to experience caesarean section than previously.1 Similar to international findings, Ireland has seen a decline in the rate of normal or intervention-free births.
October 31, 2015
-
The rate of women having a singleton live birth delivered spontaneously in 2012 was 57%, this represents a decrease from 61.8% in 2003.2 The National Maternity Hospital (NMH) is one of the largest maternity hospitals in Europe where 9,106 babies were born in 2014.3 Of these 9,106 women, 6,968 achieved a spontaneous vaginal birth without intervention, representing 70% of the total population. The caesarean section rate was 23% and the epidural rate was 45%. Both the rates of caesarean section and epidural are increasing annually and highlight the medicalisation of childbirth in the current context.
Active management of labour
The NMH is internationally recognised for the development of the active management of labour (AML), which is based on the premise that effective uterine action is the key to a physiological birth.4 This approach to the management of labour, introduced in Dublin in 1963,5 has had a significant influence on both obstetric and midwifery practice internationally. The success of AML in reducing the length of labour for women is apparent as it is now a feature of obstetric care internationally.
DOMINO
The National Maternity Hospital also introduced the first piloted DOMINO and homebirth service in 1999. DOMINO stands for DOMicillary IN and OUT; the midwifery care provided includes antenatal and intrapartum care in both the hospital and the home setting. In addition, women are provided with postnatal care and support in their own homes for a period of five to seven days. The philosophy of this approach to childbirth is to encourage and support normal childbirth with minimum interventions. Following positive evaluations from women and their partners in 2001,6 the service was formally established and offered as a midwifery-led service in a specific geographical area, namely south Dublin. The service was expanded further in 2008 to include north Wicklow. The driver for this expansion stemmed from recognition of an increased demand from well-informed women.
The DOMINO midwifery team provides an ethos of care that is women-centred and holistically underpinned by the following principles: supporting choice, shared decision-making, and facilitating empowerment for women during pregnancy and childbirth. A central feature of this model of care is the importance of ensuring mutuality and partnership in the relationships between women and midwives.
In response to the increased numbers of interventions reported, particularly epidural rates, senior midwifery management in the NMH encouraged midwifery practitioners to consider introducing and developing innovations that could reduce the rate of interventions and facilitate normal physiological birth for women.
Labour hopscotch
Subsequently, one of the community midwives designed and produced a visual framework entitled ‘labour hopscotch’, which is intended to inform and empower women and their birth partners about the steps that will facilitate a physiological birth.
The framework was designed as a tool to support women on their labour journey. Additionally, the framework was developed to support midwives as an alternative means of assisting women to achieve a physiological birth. The fundamental principle of the labour hopscotch is to inform both women and midwives of the importance of the steps necessary to remain active during labour and in this way possibly reduce interventions such as epidurals.
A key benefit of the framework is its transferability, because women can undertake the steps in their home environment and are provided with an opportunity to avoid early admission to a hospital setting. This is important as the setting for early labour is immensely powerful, and can be the difference between a fulfilling or a traumatic childbirth experience.7 A notable benefit is the opportunity it provides for partners to become involved during the birth experience.
This new initiative of supporting women will contribute to the ongoing education of student midwives and is being incorporated into midwifery curricula. Another benefit of the framework is that it focuses on the important role of the midwife in supporting women in labour and makes the mother-midwife relationship more visible. This is important because there is significant evidence to suggest that in the current configuration of maternity care, midwives are given little recognition or acknowledgement for either the care they provide or the autonomy of their practice.8 This results in women during pregnancy and childbirth receiving care that is fragmented and the international evidence highlights that fragmented midwifery care impacts negatively on the mother-midwife relationship.9
Promoting a physiological birth
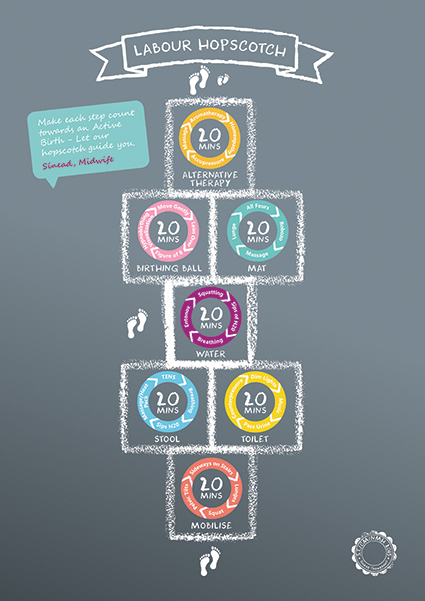
The labour hopscotch framework provides women and midwives with a visual depiction of the steps they can undertake to remain active and in this way promote optimal foetal positioning, which is paramount to achieving a physiological birth. These steps include the use of mobilisation, positioning, water-therapy and non-pharmacological methods of pain relief. An appropriate time-frame is provided for each step and is illustrated in a sequential manner that is matched with the progression of labour, as demonstrated in Figure 1. Women start at the bottom of the hopscotch as they are more active and mobile. As labour progresses, they advance towards the baby’s footprints. This is a motivational image for them to visualise and facilitates them to maintain focus during labour.
 (click to enlarge)
(click to enlarge)