LARC methods have several differentiating features from other forms of contraception which can make them particularly suited to certain groups of women
Dr Deirdre Lundy, Family Planning Course Co-Ordinator, Irish College of General Practitioners, Dublin
Long-Acting Reversible Contraception (LARC) is the term used to describe types of contraception that provide protection for an extended period and involve little user effort. As a result of this lack of need for compliance, they have been shown to be the most effective options for women who want to avoid pregnancy.
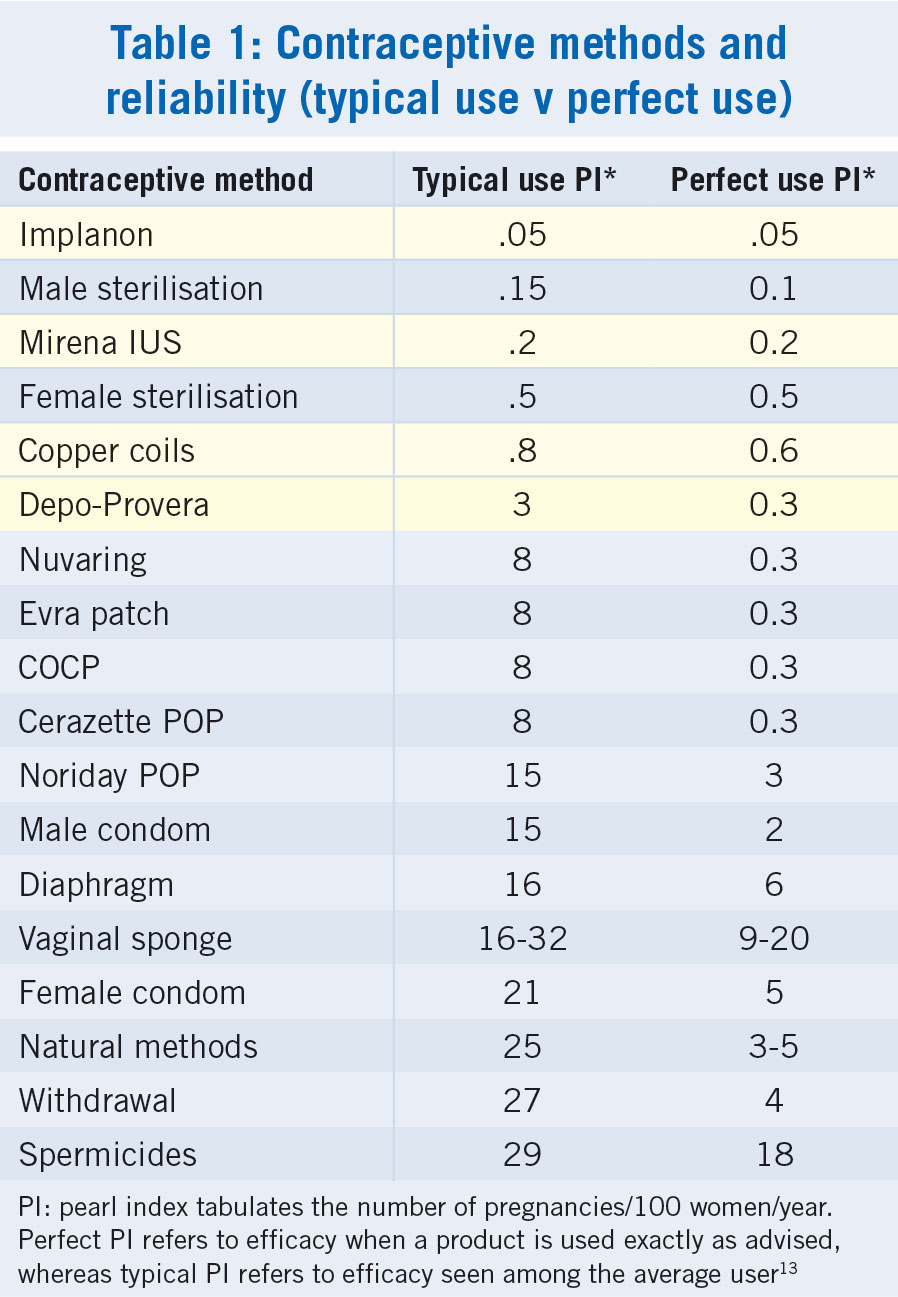
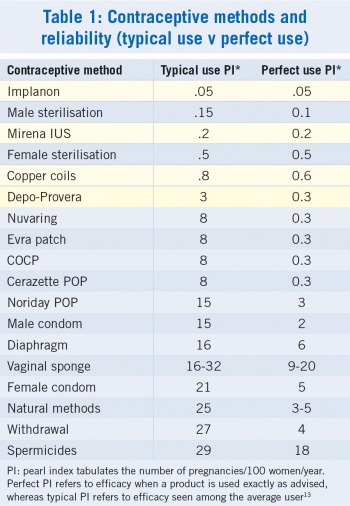
In Ireland, most women opt for condoms or an oral contraceptive unless prompted to consider a LARC.1 However, condoms and the pill are among the least reliable alternatives (see Table 1) as both require significant user compliance.2 If used ‘perfectly’ the combined oestrogen/ progestagen pill should allow as few as 0.3 pregnancies for every 100 women per year of use – a very small failure rate. In actuality, the failure rate of the combined pill is closer to eight pregnancies per 100 women/years.
(click to enlarge)
PI refers to the ‘pearl index’ of contraceptive efficacy. It tabulates the number of pregnancies per 100 women per year of use. The ‘perfect’ PI refers to efficacy when a product is used exactly as advised, where the ‘typical’ PI refers to the efficacy that is seen among the average user.
Can healthcare providers make a difference?
A US study asked just that question: would women choose LARC methods over pills and condoms if given the choice (and if access to LARC was facilitated)? The answer was positive.3 The 2008 contraceptive ‘CHOICE’ project was conducted in various university and community-based health centres all over St Louis in Missouri, US.
Interestingly, among the women who chose an IUD, almost half were nulliparous, even though this is often perceived as a barrier to IU contraception by Irish GPs and patients alike.
Barriers to successful contraception include: forgetting to take a tablet at a critical time; vomiting after taking a pill; or being on a course of liver enzyme inducing medications.3 Younger women are often less disciplined in pill taking than their older counterparts. LARC is particularly well suited for sexually active young women.
While LARC methods may be expensive initially, they are more cost-effective than the pill after as little as 12 months.
Depo-Provera
Medroxyprogesterone acetate has been available as the 150mg deep IM injection Depo-Provera for decades in Ireland. The large bolus of progestagen delivered to the gluteus or deltoid muscle has a strong impact on the hypothalamic-pituitary-ovarian hormone axis causing anovulation. It can be started at any time of the cycle with or without a period, as long as a current pregnancy can be ruled out.
It begins to work almost immediately and is one of the most effective contraceptives available, with a PI of 0.3 pregnancies per 100 women/year. Typical efficacy is closer to three pregnancies per 100 women/year (late attenders and not managing to find deep muscle when administering the injection are possible explanations).
Impact, benefits and potential side-effects
The impact on ovarian activity can sometimes be so profound that circulating oestrogen levels may drop and a transient reduction in bone mineral density can result. This phenomenon has never been linked to an increase in fracture risk and recovers within weeks of discontinuing the Depo-Provera. It is for this reason that women under 18 (who have yet to achieve their maximal bone density) and women over 45 (who are starting to lose bone density more rapidly) might benefit from a fracture risk assessment before commencing this product.
If they are already high risk for fracture with a multiplicity of lifestyle risks (eg. very low BMI, heavy smoking, sedentary lifestyle, high-dose steroid use, etc.) then Depo-Provera may not be the wisest option for them. If they have considered and then rejected other options, even these women may use the Depo-Provera injection, but a two-yearly reassessment is recommended.4
For most healthy young women, the benefits of Depo-Provera contraception far outweigh any risk and it is an excellent option for women who need highly reliable contraception but aren’t prepared to commit to the cost of an implant or IUD.
The anovulation lasts for at least 12 weeks; the UK Faculty of Reproductive and Sexual Health advises that Depo-Provera can be protective for up to 13 or 14 weeks (although this is outside the product licence of 12 weekly injections). For women on liver enzyme-inducing medications there is no need to shorten the injection intervals as was previously thought (the large dose of progestagen is fully cleared by the liver in the first pass).
The relatively high dose of synthetic progestagen may have some unwanted side-effects, however. Some women complain of acne, bloating, headache, alopecia, flushes, decreased libido or moodiness but causation has never been established. A small but significant proportion of women experience rapid weight gain (Depo-Provera is the only form of contraception proven to do this). Weight gain is more likely to be an issue for women under 18 years of age with a body mass index (BMI) ≥ 30kg/m² and if this is an issue it is likely to get worse. Alternatives should be considered.
Use of Depo-Provera usually results in a much lighter or non-existent PV bleed after the first or second injection. While this is reversible it may interfere with conception for 6-12 months after the injections are discontinued so forward planning is suggested. Being amenorrhoeic on Depo-Provera does not imply low fertility and in fact the amenorrhoea may be beneficial for women who suffer from menorrhagia or endometriosis, are HIV positive, suffer from severe dysmenorrhoea or who are homeless.
Use with combined pill
Before becoming amenorrhoeic, some users experience unscheduled bleeding in the first three to six months. For those who are medically eligible, a three-month prescription of the combined pill (COC) may be offered to help resolve this annoying side-effect.
The pill can be taken in the usual cyclic manner or continuously without the pill-free interval (this too is outside the product license). Longer-term use of the Depo-Provera with additional COC has not been studied and is a matter of clinical judgement. Alternatively, unscheduled bleeding can be controlled with 500mg mefenamic acid up to three times daily for five days. Persistent unscheduled bleeding should be investigated and STIs and other pathologies ruled out.
Depo-Provera is suitable for breastfeeding mothers and women who have been told to avoid oestrogen-containing pills because of obesity or smoking. It is only UK Medical Eligibility Criteria (UKMEC) Category 2 (benefits outweigh risks) for women who currently have or have had a deep vein thrombosis or suffer from migraine with aura.
Mirena intra-uterine system
Since its launch in Ireland in 1998 the Mirena intra-uterine hormonal contraceptive system (IUS) has revolutionised the concept of in-utero contraception. Prior to the development of Mirena, the only IU contraceptives in Ireland were all copper-bearing. Copper devices are reliable contraceptives but copper usually creates longer and heavier periods for wearers. Since it is often the older, parous women who typically opt for IU contraception and since many of those are already struggling with menorrhagia, only a limited selection of women were suitable for IU products.
Mirena has a good ‘period improving’ effect and helps ease menorrhagia and dysmenorrhoea. These effects are derived from the hormone-bearing frame on the Mirena device. Mirena is made up of a plastic frame similar to many copper IU devices but unlike those devices Mirena has a levonorgestrel progestagen reservoir running down its vertical shaft.
The levonorgestrel hormone is a good contraceptive. It alters cervical mucus, rendering it hostile to sperm. It also alters the endometrium making it less receptive to implantation. These, among other contraceptive effects, prevent pregnancy. Occasionally, enough of the progestagen hormone is absorbed into the uterine vasculature (and then on into the systemic circulation) to cause anovulation.
The most novel effect of IU levonorgestrel is that it causes significant endometrial depletion. The microscopic features seen within the endometria of Mirena wearers are similar to those expected to be seen in the presence of a foreign body (eg. surface undulations, inflammatory cell infiltration, and stromal haemosiderin deposition) as well as features seen as a result of progestagen exposure (eg. glandular atrophy and stromal decidualisation).5
Initially this may create longer or more frequent PV bleeding (while the womb lining is being shed) but eventually the thinner, lighter endometrium should mean shorter, lighter periods for most women. It is the only IUD available in Ireland that does this. Its smaller, sister brand Jaydess will not lighten periods and copper devices usually make them worse.6
Mirena was licensed for the treatment of menorrhagia in 2001 and swiftly became a much more popular option for that condition than hysterectomy. Multiple studies exist exploring the decline in hysterectomy rates in communities where Mirena became available.
A Mirena is made of a plastic membrane reservoir containing 52mg of levonorgestrel wrapped around a T-shaped, polyethylene frame. There are two, thin nylon threads or strings at the base of the device that are designed to extend through the cervical canal and into the top of the vagina to aid removal. The membrane only allows 20µg of the hormone to escape over 24 hours in the first few years, dropping down to 12µg and then 10µg in the fourth and fifth years of use respectively. This gives the device long-term effectiveness for at least five years.
If a woman using Mirena that is less than five years in situ chooses to take hormone replacement therapy (HRT) she only requires an oestrogen product, as the Mirena’s levonorgestrel will protect her endometrium from unhealthy proliferation that unopposed oestrogen might cause.
If a women over 50 requires HRT and is keeping a Mirena beyond the five-year license for contraception (as is allowed by the Faculty of Sexual and Reproductive Healthcare, FSRH www.fsrh.org) she must use a combination oestrogen plus progestogen HRT product. Sometimes a new device may be inserted for women over 50 either for HRT or if menorrhagia is starting to return.
Placement can be offered at any time of the cycle as long as pregnancy can be reasonably outruled. The Faculty of Sexual and Reproductive Healthcare (FSRH) has guidelines on how this can be established.7 The ICGP LARC insertion counselling and fitting protocols include information on many aspects of LARC insertion. They can be downloaded from the women’s health section of www.icgp.ie
Mirena is expensive at the outset although cost-effective over the five or more years of use. It is covered by the Drugs Payment Scheme and currently non-medical card holders will pay €144 for it and other medications they require in that calendar month. Insertion charges vary. The Mirena insertion is covered by the GMS.
All GPs should be familiar with the exclusion criteria, advantages, disadvantages, likely side effects, cost, etc. of all contraceptives. It’s most important that a woman can make an informed choice about her method before spending money on something costly like Mirena or one of the other expensive devices.
Contraindications to Mirena
Contraindications to Mirena include recent septic abortion, CVA, MI, trophoblastic pregnancy with continued elevated β-HCG levels, current breast, ovarian or endometrial cancer, uterine fibroids that distort the uterine cavity, current pelvic inflammatory disease (PID), chlamydia or gonorrhoea, pelvic TB, severe liver disease, SLE with antiphospholipid antibodies and/or severe thrombocytopaenia.
Nulliparity, multiple Caesarean sections and a past history of ectopic pregnancy or PID are not contraindications to any IU device.
Risks and rare adverse events
These include pain on insertion, insertion failure, vasovagal reactions, bleeding, perforation, migration, expulsion and failure of the device. Overall, ectopic pregnancy rates are reduced by using efficacious contraception including a Mirena. Unfortunately though, when a rare failure with a Mirena in situ does occur, that pregnancy is more likely to be ectopic and requires urgent referral.
Infection is a rare complication of Mirena placement. For the first 20 days after insertion a woman is more vulnerable to ascending infection as the cervical mucus plug has been breached by instrumentation and placement of the foreign body. If the inserting doctor uses asceptic technique and if the patient is free from an STI at the time of placement the risk of infection thereafter is the same for any other sexually active woman. This is true for all IUD wearers.
Perforation of the uterus is a rare but important known risk and is much more likely to occur with inexperience and if performed too soon post-partum. Women should wait at least six to eight weeks after spontaneous vaginal delivery and 8-12 weeks after uncomplicated C section for this reason. Bridging contraception with non-oestrogen hormones like the POP or Depo-Provera can be offered immediately post partum while arranging IUD insertion.
Systemic absorption of the levonorgestrel while minimal may still cause noticeable side-effects, eg. headache/migraine, nervousness, dizziness, nausea, vomiting, bloating, breast tenderness or pain, weight gain, changes in hair growth, acne, depression, changes in mood, loss of interest in sex, itching or skin rash, and puffiness in the face, hands, ankles or feet. Return to fertility is immediate after the device is removed.
In addition to counselling, women considering a Mirena insertion should have a bimanual and speculum exam by the GP who is prescribing the device. This will establish if the patient has gynaecological issues that prevent her from using an IUD.
Nucleic acid amplification test (NAAT) screening for vaginal STIs can be offered if necessary (young patients and women with new partners are particularly at risk). The more occult infections like chlamydia and gonorrhoea are most important to outrule. Bridging contraception should be advised, but if the women does not wish to take this she should be advised to abstain from intercourse for three weeks prior to insertion.
Once inserted, the device may take up to an additional seven days before it becomes fully effective and a six-week post insertion check-up is recommended to confirm the nylon strings of the device are still present and that the patient is well.
There are various opportunities available to learn Mirena insertion techniques. Insertion technique can be observed and learned during gynae training or by GP trainees in a training practice where IUDs are offered. GP colleagues may offer training to one another.
Jaydess
Jaydess may be described as ‘Mirena-lite’. It is an effective IU contraceptive but smaller in size and lighter in hormone load. It doesn’t last as long and won’t help menorrhagia but it does deliver effective contraception for three years.
Jaydess comprises a plastic membrane reservoir of 13.5mg of levonorgestrel wrapped around a small, T-shaped, polyethylene frame. Unlike the Mirena, Jaydess’s vertical stem contains a silver ring located close to the horizontal arms so you can identify one from the other on ultrasound scan or x-ray. It’s a smaller device than a Mirena
(28 x 30 x 1.55mm) and insertion tends to be easier and less uncomfortable.
Unlike Mirena, Jaydess is not recommended as a first-line contraceptive for nulliparous women. But after discussion of alternatives, Jaydess may be inserted into women under 18 years. The counselling and pre-insertion preparation for Jaydess are similar to that of Mirena.
According to FSRH guidance, use of Jaydess in women under 18 years of age should not generally be restricted (UKMEC 2) and it can be used from menarche to menopause.6
The SPC for Jaydess quotes an ectopic rate of 0.11 per 100 women/year, and it quotes an ectopic rate of 50% with failures. Therefore, women who become pregnant while using Jaydess are advised to seek advice and immediately exclude ectopic pregnancy. The FSRH has explained why differences in the absolute and relative risks of ectopic pregnancy between Mirena and Jaydess should be interpreted with caution until more pregnancy data are available.7
Copper IUDs
Throughout the world the most popular choice of intrauterine contraception is still a coil with copper on it. For example the majority of fertile, sexually active Chinese women use a copper device.8 In Ireland copper devices were popular until the Mirena became available. These devices are not expensive, may last up to 12 years or more and are free of hormone-related side-effects. Copper bearing devices are the only LARC option that can be inserted as a form of emergency or post-coital contraception and are much more efficacious than either oral ulipristal acetate or levonorgestrel for this purpose. They maintain this high post-coital efficacy for more than five days after the episode of unprotected sex.
Intrauterine copper devices come in many different shapes and sizes but only the ones that are T-shaped and have 380mm² of copper on both the vertical shaft and the horizontal arms are recommended by the FSRH. The greatest amount of data exists on these devices.
The average cost is under e30 and if inserted after a woman is 40 years of age, the FSRH does not recommend routine replacement.
Copper is toxic to both ovum and sperm, therefore a copper coil works primarily by inhibiting fertilisation.7 In addition, the endometrial inflammatory reaction has an anti-implantation effect. The copper ions in the cervical mucus inhibit sperm penetration. The efficacy of copper devices are similar to that of Mirena and Jaydess
The pre-insertion counselling and assessment are the same for IUCD as Mirena/Jaydess but some eligibility criteria are different. Unlike a hormone containing coil, a copper coil is recommended for use in women with current VTE (on anticoagulants), ovarian cancer, ischaemic heart disease, current or past history of breast cancer, active viral hepatitis, severe decompensated cirrhosis or liver tumours (benign or malignant).
Some women prefer a non-hormonal version of an IUD even though they have no medical reasons to avoid an IUS and that should be their choice.
Those women who should not routinely be offered a copper device (but may be offered an IUS) include those with heavy or prolonged bleeding, endometriosis; severe dysmenorrhoea or anaemias such as thalassaemia, sickle cell disease and uncorrected iron deficiency anaemia. Wilson’s disease and copper allergy are also contraindications for copper devices.
Placement procedures are identical for hormone coils and copper coils but copper devices require a two-handed technique to get the device out of the insertion tube (as opposed to the innovative, one-handed ‘Evo-inserter’ device used with Mirena and Jaydess).
The most common side-effect of a copper coil is extra bleeding. This is occasionally a reason for discontinuation so must be addressed at counselling. Although copper IUDs do not have any effect on ovulation they can be associated with shorter luteal phases and therefore shorter cycles. Heavier or longer menstrual periods are common in the first three to six months following Cu-IUD insertion but additional dysmenorrhoea doesn’t seem to be an issue.
These longer and heavier bleeding patterns are not harmful unless so severe as to cause distress or anaemia; they usually decrease with time. Discontinuation due to bleeding is similar for the different types of Cu-IUDs.10
Implanon NXT
Over the past 17 years, Implanon has proven to be an effective and popular LARC, particularly among younger, nulliparous women. Implanon NXT, the current version, is a 4cm radiopaque, non-biodegradable implant that contains 68mg of etonorgestrel, a progestagen.
Etonorgestrel is a strong anovulant progestagen and so its primary mode of action is prevention of ovulation; thickening of the cervical mucus and alteration to the endometrium are also observed, adding to its contraceptive activity.9
In the 2007 American review of contraceptive failure, the etonorgestrel implant had the lowest failure rate; as few as 0.05% pregnancies in the first year of use.2 Despite this, the return to fertility appears to be almost immediate after removal of the implant.
Etonorgestrel’s suppressive action on ovulation and endometrial development gives it non contraceptive benefit for dysmenorrhoea and to some degree endometriosis.
The impact of etonorgestrel on the endometrium is variable and as a result so are the PV bleeding patterns that emerge. This may be the biggest challenge for Implanon NXT users and the doctors who care for them. On the one hand you are offering a supremely reliable and fully reversible contraceptive product, but on the other hand you have to contend with a variety of possible bleeding patterns
Approximately 25% of users will become mostly amenorrhoeic but this may take up to six months to establish. Irregular, ‘unscheduled’ bleeding is not uncommon immediately after insertion. For an unfortunate 33% or so of users, this troublesome bleeding won’t settle on its own and may need further medication to control it.
Various treatments have been investigated for the management of bleeding problems with progestagen-only implant users. Mefenamic acid and/or the combined pill have been shown to reduce bleeding. The FSRH guidelines recommend a three-month trial of the combined pill (where not contraindicated) taken either as usual or continuously (ie. omitting the pill-free interval).11
Doxycycline alone or in combination with the combined pill has also been shown to be effective at resolving this spotting but it may return quickly after discontinuing the support medication.
Prof John Guillebaud has suggested trying a form of endometrial ‘preemptive strike’ by offering an injection of Depo-Provera prior to inserting the implant.12 This often reduces the incidence of disruptive bleeding and improves user satisfaction. If the bleeding is unresponsive within three to four months, consider the possibility of an underlying pathology such as an STI, polyp, cervical carcinoma, etc.
Few conditions prevent the use of an implant as etonogestrel does not appear to have any impact on the cardiovascular system. Age is not an issue; it can be offered from menarche to menopause and can be used by smokers or women who are breastfeeding. Women who experience migraine with aura may use the implant (as they can any other non-oestrogen product) but should discontinue if the migraines worsen.
Possible reasons not to use Implanon NXT include current or recent breast cancers and serious liver disease such as severe cirrhosis, malignant hepatomata and benign hepatocellular adenomata. SLE with positive or unknown antiphospholipid antibodies is also a precaution. The most common conflict arises from the impact that liver enzyme inducers (LEI) inflict on the metabolism of Implanon NXT. Women using rifampicin, some anticonvulsants (including topiramate as used for migraine) or taking certain anti-
retrovirals must avoid the implant until they are 28 days free from the LEI.
Pharmacokinetic studies of progestagen-only implants have shown an inverse relationship between body weight and etonogestrel serum levels. There are concerns about the duration for which the method is effective in ‘heavier’ women. Although licensed for use up to 149kg (regardless of BMI) it is advisable to change those implants earlier than the full three years. Side-effects include weight change, low mood and low libido. Acne may occur, improve or get worse. Headache has been reported as a possible side-effect.
Insertion of Implanon NXT
The device should be inserted on the inner aspect of the upper arm, 10cm proximal to the medial epicondyle; avoiding the biceps groove and the structures buried in there. A marking guide is supplied by the manufacturer to assist accurate placement. The non-dominant arm is suggested but this is a matter of patient choice.
A local anaesthetic should be applied or instilled (cryogesic spray is effective as is subcutaneous lignocaine). An aseptic but not necessarily sterile technique is required for insertion. The device should be inserted fully under the skin avoiding the structures below. When correctly placed it should be easily palpable under the dermis.
Practice under supervision is required to gain confidence and although the new insertion device is designed to minimise the risk of placing the implant too deep, this may still occur. Placement too deep in muscle or fat doesn’t impair the efficacy of the hormone but it makes removal very difficult. Very deep placements have been reported and injury to the vasculature or nervous system is possible and should be counselled about. If a device is not palpable at any stage – even immediately after insertion, the patient must be put on alternative contraception until the device has been located (x-ray or ultrasound).
Removal of a device requires some expertise and should not be undertaken without experience and never in cases where a device is impalpably deep. A sterile technique must be used for removals and efforts made to minimise the size of the removal puncture wound. A new device may be inserted through the removal wound but the new device should be inserted at an angle to the tract made by the previous device. The wound can be closed with steri-strips rather than sutures to improve cosmetic outcome.
Skin atrophy has been reported after placement which may be an adverse effect of local exposure to the steroid hormone. All of this must be discussed at the pre-insertion counselling. Printable consent forms can be found in the women’s health section of www.icgp.ie
Conclusion
LARCs have been shown to be very reliable and can have other, non-contraceptive benefits. In practice we have found that suitable patients are often either unaware of these options or believe themselves (wrongly) to be unsuitable. As part of the new GMS deal on special items, the fee for LARC will be e70 for insertion and e50 for removal. Forthcoming ICGP courses and events related to LARC can be found at www.icgp.ie
References
McBride O, Morgan K, McGee H. Irish contraception and crisis pregnancy Study 2010 (ICCP-2010) A Survey of the General Population
Trussell J. Contraceptive efficacy. In: Hatcher RA, Trussell J, Stewart F, et al. Contraceptive Technology: Nineteenth Revised Edition. New York, NY: Ardent Media, 2007
Secura GM, et al. The Contraceptive CHOICE Project: Reducing barriers to long-acting reversible contraception. Am J Obstet Gynecol. 2010; 203(2): 115.e1-115.e7 doi:10.1016/j.ajog.2010.04.017.
Faculty of Sexual and Reproductive Healthcare Guidance. Progestagen-only injectable contraception. Clinical Effectiveness Unit December 2014 (Updated March 2015)
Phillips V et al. The effects of the levonorgestrel intrauterine system (Mirena coil) on endometrial morphology. J Clin Pathol 2003; 56: 305-307
Faculty of Sexual and Reproductive Healthcare Guidance. Clinical Effectiveness Unit. Jaydess Levonorgestrel Intrauterine System, April 2014
Faculty of Sexual and Reproductive Healthcare Guidance. Intrauterine Contraception. Clinical Effectiveness Unit, April 2015 (Updated October 2015)
Wang D, Altmann DR. Fertility Control: Socio-demographic determinants of intrauterine device use and failure in China. Hum Reprod. 2002; 17(5): 1226-1232 doi:10.1093/humrep/17.5.1226
Faculty of Sexual and Reproductive Healthcare Guidance. Progestagen-only implants. Clinical Effectiveness Unit, February 2014
Hormonal Contraception. National Medicines Information Centre, St James’s Hospital, Dublin. Volume 16, Number 4, 2010
Faculty of Sexual and Reproductive Healthcare Guidance. Progestagen-only implants. Clinical Effectiveness Unit, February 2014
The pill and other forms of hormonal contraception. Seventh Edition. John Guillebaud and Anne MacGregor. Oxford
Pearl R. Factors in human fertility and their statistical evaluation. Lancet, 1933; 222(5741): 607-611 http://www.sciencedirect.com/science/article/pii/S0140673601186484
NICE guideline on long-acting reversible contraception, October 2005 (rev. April 2014) https://www.nice.org.uk/guidance/cg30
 (click to enlarge)
(click to enlarge)