Malignant spinal cord compression is a neurological emergency and early diagnosis is essential in the prevention of neurological complications
Dr Elaine Wallace, Consultant Physician in Palliative Medicine, Our Lady of Lourdes Hospital, Drogheda, Co Louth and Dr Suzanne Ryan, Specialist Registrar in Palliative Medicine, Louth Meath Specialist Palliative Care Services, Dochas Centre, Our Lady of Lourdes Hospital, Drogheda, Co Louth
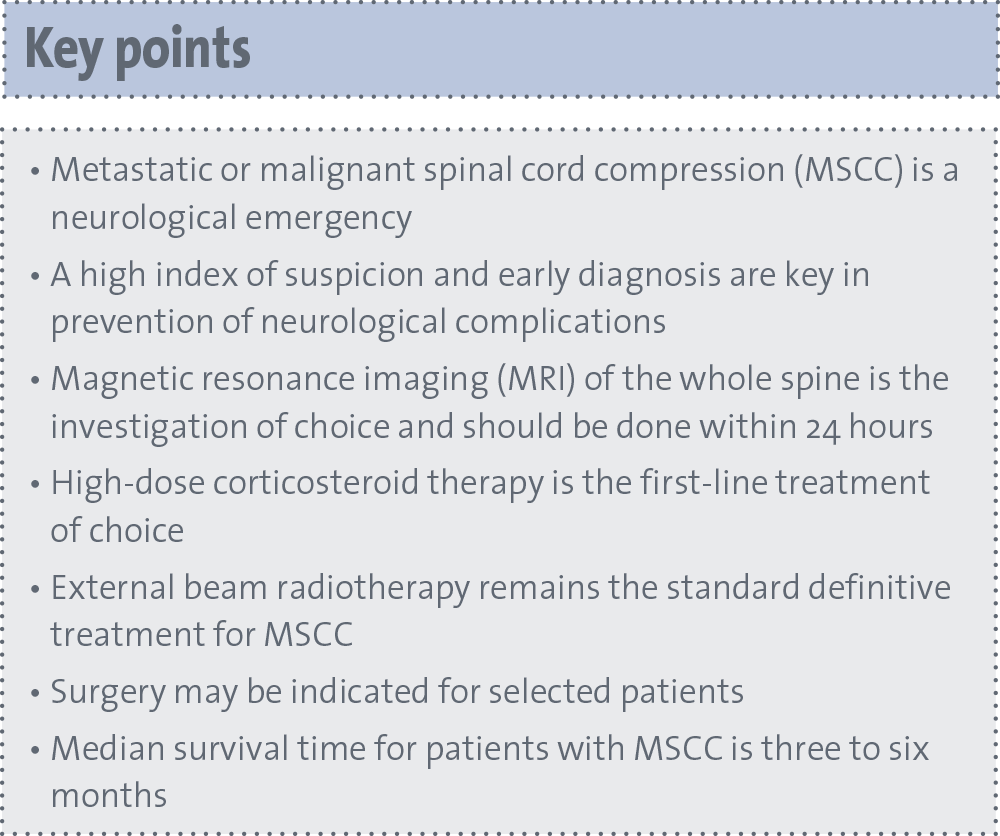
Metastatic or malignant spinal cord compression (MSCC) is defined as spinal cord or cauda equina compression by direct pressure and/or induction of vertebral collapse or instability by metastatic spread or direct extension of malignancy that threatens or causes neurological disability.1 MSCC is a neurological emergency. Early diagnosis is key in prevention of neurological complications. Treatment must be implemented early as neurological status at presentation strongly predicts functional outcome.2
Incidence
MSCC is thought to affect 4,000 patients annually in Wales and England and, from autopsy studies, it is believed to occur in 5% of all patients diagnosed with cancer.1,3 A US-based study identified an annual incidence of 3.4% of hospitalised patients with cancer.4 In reality, the true incidence of MSCC is unknown as many cancer patients have MSCC that is unrecognised. In some cases, a decision may be made that further investigation is not in the best interests of a patient.
MSCC can occur from any primary tumour site, but it is more common in malignancies that are more likely to metastasise to the spinal column. In adults, therefore, lung, prostate and breast cancer account for 15-20% of all cases of MSCC. Non-Hodgkin’s lymphoma, renal cell cancer and multiple myeloma account for a further 5-10%.3 Tumours responsible for MSCC in children differ from adults and include sarcomas, neuroblastomas, germ cell tumours and Hodgkin’s lymphoma.
Approximately 20-23% of patients present with MSCC as the initial manifestation of malignancy.5,6 This is particularly true for lung cancer, where 30% of MSCC diagnoses are made in patients without a previous diagnosis of cancer.7 The distribution of lesions causing compression within the spine corresponds to the number of vertebrae in each region, with 60% occurring in the thoracic, 30% in the lumbar and 10% in the cervical spine. Approximately 20-35% of patients, however, present with compression at multiple sites.3
Pathophysiology
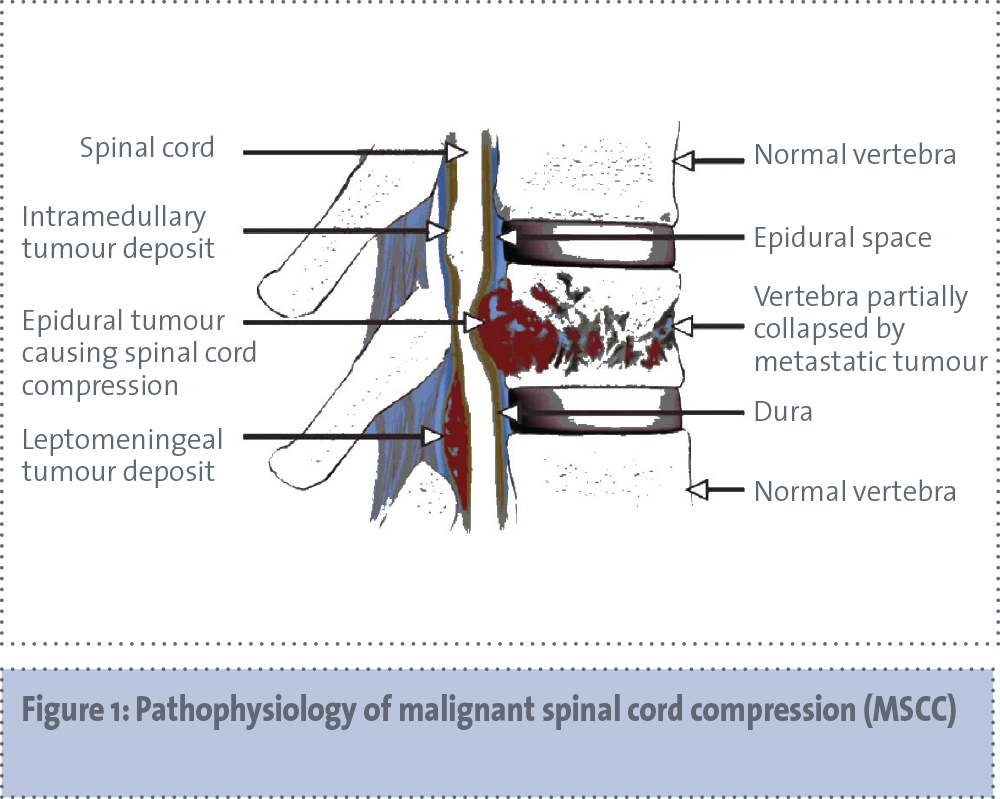
At each spinal level, nerve roots exit lateral to the spinal cord and posterior to the vertebral body. MSCC occurs when the tumour invades the epidural space and compresses the thecal sac. This can occur by two mechanisms. In 15% of cases, growth of a paravertebral tumour directly into the spinal canal causes direct compression. Most commonly, the tumour arises from the vertebral body, grows in size and causes secondary compression of the cord.3 This process is usually gradual, although it can occur acutely during vertebral collapse and sudden displacement of vertebral fragments. Direct compression of the cord causes demyelination, axonal damage and secondary vascular compromise. Obstruction of the epidural venous plexus results in vasogenic oedema. Administration of corticosteroids at this stage can reduce or reverse oedema associated neurological dysfunction. As the process progresses, with persistent compression, arterial blood supply is impaired resulting in cord ischaemia, infarction and irreversible neurological damage (see Figure 1).
(click to enlarge)
Clinical presentation
Back pain is the earliest and most common symptom of MSCC and is present in 95% of patients at diagnosis.3 The median time from onset of pain to diagnosis of MSCC is approximately two months and it has often been present for a number of weeks before the diagnosis of MSCC is made (median six to eight weeks).8 Research has shown significant delays from the time when patients first develop symptoms to when general practitioners (GPs) and hospital doctors recognise the possibility of MSCC and make an appropriate referral.9
Localised pain that is confined to the affected region, which progressively increases in severity, is generally the first symptom. This pain results from stretching of the periosteum or soft tissue invasion as the bone metastasis increases in size. Over time, radicular pain results from compression or invasion of nerve roots. This pain is typically worse at night or on straining. Unilateral pain is common from cervical and lumbar spine involvement. Thoracic involvement is frequently bilateral and characteristically wraps around anteriorly in a band-like fashion.
Weakness is the second most common presenting symptom, present in 35-75% of cases. Patients can non-specifically complain of being ‘off their feet’ or of ‘heaviness in the limbs’. Approximately 50-68% of patients are unable to walk at the time of diagnosis. The extent of motor deficit is dependant on the location of compression, but can involve upper or lower motor neurone weakness.3 The development of ataxia, loss of co-ordination or paralysis are usually late findings.8
Other clinical findings occur less frequently and are more variable. Sensory disturbances rarely occur in the absence of motor deficits.3 Parasthesia and loss of sensation may develop and typically begin distally and ascend, but can be poorly localised to the site.10 Autonomic symptoms causing constipation and/or urinary retention that progress to double incontinence occur late and are rarely the only presenting symptoms.10 Sphincter disturbance is a poor prognostic sign.3
Diagnosis
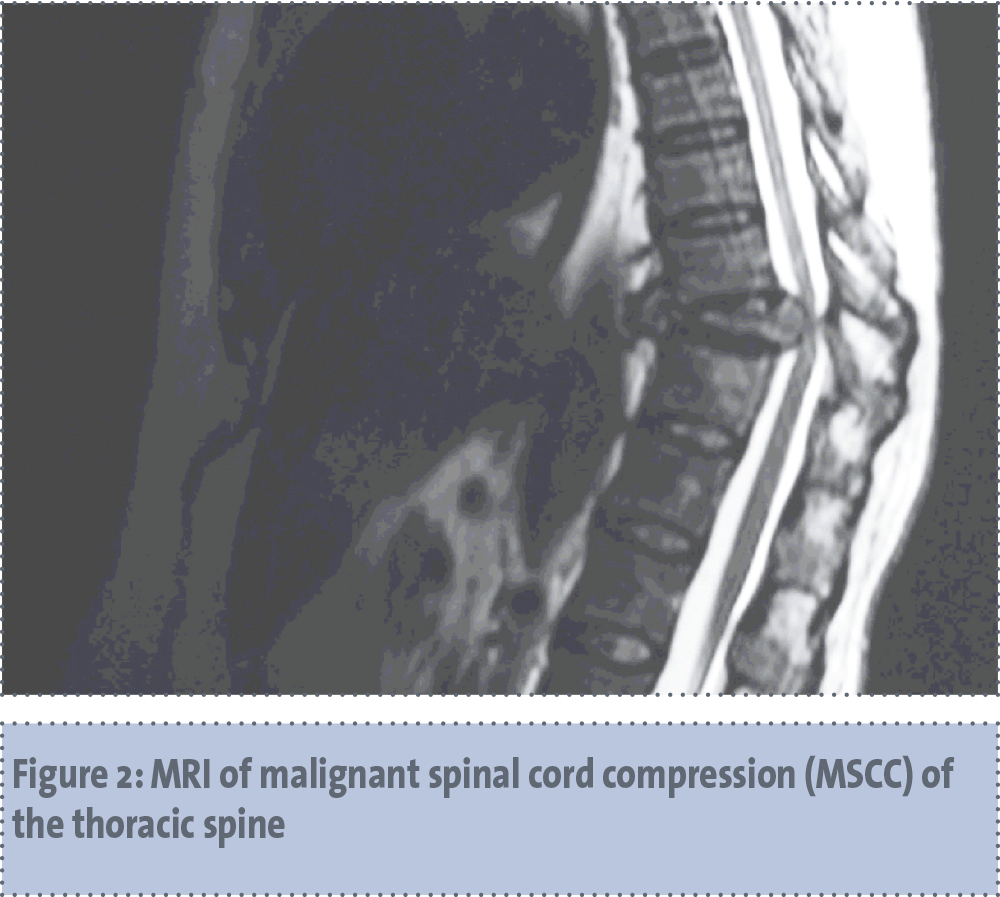
A high index of suspicion is the most effective tool in preventing the devastating consequences of this condition. Clinical suspicion should prompt a comprehensive medical history and examination, but clinical features are not sensitive enough to make the diagnosis.11 Magnetic resonance imaging (MRI) of the whole spine is the investigation of choice (see Figure 2). It is necessary to image the entire spine, as up to one-third of patients have compression present at multiple sites. MRI is 95% accurate in diagnosing MSCC, with 93% sensitivity and 97% specificity.12 NICE guidelines advise urgent MRI within 24 hours for all patients with suspected MSCC.1 Myelography was the image of choice, in the past, prior to the widespread availability of MRI.3 Several other imaging techniques do not display the accuracy of MRI and are less useful. Computed tomography (CT) does not demonstrate the spinal cord or epidural space clearly.13 Plain radiography should not be used as a screening procedure as it has insufficient sensitivity and specificity and can delay MRI.
(click to enlarge)
Management
The goals of treatment of MSCC include pain control, avoidance of complications and preservation or improvement of neurological function. Management includes immediate administration of corticosteroids to reduce oedema in nearly all patients, followed by definitive treatment of radiotherapy or surgery. Systemic therapy may be beneficial in patients with chemosensitive tumours.
Corticosteroids
High-dose corticosteroid therapy is the first-line treatment for most patients with MSCC, despite limited evidence of benefit and significant risk of serious adverse-effects. Corticosteroids are contraindicated if there is a significant suspicion of lymphoma. Sorenson et al, established the efficacy of steroids in the treatment of MSCC and demonstrated higher ambulatory rates in patients who received high-dose dexamethasone and radiotherapy compared to radiotherapy alone.14 The optimal dose remains unknown.
A Cochrane meta-analysis of three studies concluded that higher doses of corticosteroids were not associated with better outcomes, but were associated with a higher incidence of serious adverse-events.15 NICE guidelines advise a loading dose of 16mg of dexamethasone as soon as possible after assessment followed by a short course of 16mg per day until definitive treatment has been implemented. Following surgery or radiotherapy the dose should be gradually reduced and discontinued, but should be restarted if neurological function deteriorates.1 Blood glucose monitoring is advised in patients on dexamethasone.1
Radiotherapy
External beam radiotherapy has been the standard definitive treatment for MSCC since the 1950s. It is most effective in patients who have tumours that are radiosensitive and who are ambulatory when they begin treatment. Radiation is generally delivered to the involved segment as well as the level above and below. The optimal radiation dose and fractionation scheme are dependent on particular circumstances: a shorter course of treatment is preferable in patients who have a short expected survival, however, long-term local control is better with protracted schedules and is preferable for patients with a good performance status.3 NICE guidelines advise fractionated therapy to patients with a good prognosis who have radiotherapy as their first-line treatment.1
Surgery
In the past, surgery for the management of MSCC was controversial, but recent advances have established its efficacy in selected patients. Patchell et al, performed a randomised controlled trial in 2005 which established that direct decompressive surgery plus post-operative radiotherapy is superior to treatment with radiotherapy alone. Patients in the surgery arm retained ambulatory function for longer.16 Patients in this study had MSCC at one single area, were acceptable surgical candidates and had an expected survival of at least three months.
Careful selection is required to identify those patients with an adequate life expectancy and good performance status who may be candidates for surgery. Suitable patients, therefore, should be offered surgery. Surgical decompression is the preferred approach for patients with an unstable spine and for relatively radioresistant tumours.17 NICE guidelines advise that only patients with an expected survival of greater than three months should be considered for surgical treatment.1
Prognosis
The most important outcomes for patients with MSCC are ambulatory function and length of survival. MSCC usually occurs in the setting of advanced malignancy and retrospective studies have demonstrated that median survival time for patients with MSCC is three to six months.5,9 The most important prognostic indicator for the prediction of ambulatory outcome is patients’ pretreatment ambulatory status. Other factors which predict improved ambulation include radiosensitive tumours and a more gradual onset of motor symptoms. Factors associated with longer survival are: a single site of compression, absence of visceral or brain metastatic disease, radiosensitive tumours and the ability to walk before and after treatment.3
(click to enlarge)
Conclusion
Metastatic spinal cord compression is a devastating complication of cancer and, if left undetected or untreated, can lead to permanent neurology and can shorten survival. Clinical suspicion is the most important factor in diagnosing this condition and urgent MRI is required to make the definitive diagnosis. Corticosteroids are the first-line of treatment, followed by urgent radiotherapy, however, surgery may be indicated for selected patients.
References
National Institute for Health and Clinical Excellence. Metastatic spinal cord compression: Diagnosis and management of patients at risk of or with metastatic spinal cord compression. Clinical Guideline 75. London: NICE, 2008. www.nice.org.uk/CG75
Santamaria E, Schiff D. Spinal cord compression. Curr Treat Options Neurol 2012; 14: 391-401.
Loblaw DA, Laperriere NJ, McKillop WJ. A population-based study of malignant spinal cord compression in Ontario. Clin Oncol 2003; 15; 211-217.
Schiff D, O’Neill BP, Suman VJ. Spinal epidural metastases as the initial manifestation of malignancy: clinical features and diagnostic approach. Neurology 1997; 49: 452-456.
Mak KS, Lee LK, Mak RH, et al. Incidence and treatment patterns in hospitalisations for malignant spinal cord compression in the United States 1998-2006. Int J Radiat Oncol Biol Phys 2011; 80: 824-831.
Abrahm JL. Assessment and treatment of patients with Malignant Spinal Cord Compression. J Supportive Oncol 2004; 2(5): 377-407.
Rades D, Fehlauer F, Schulte R, et al. Prognostic factors for local control and survival after radiotherapy of metastatic spinal cord compression. J Clin Oncol 2006; 24: 3388-3393.
West of Scotland Malignant Spinal Cord Compression Guidelines Development Working Group. West of Scotland Guidelines for Malignant Spinal Cord Compression (v2.0); NHS UK, 2013.
Ruckdeshel JC. Early detection and treatment of spinal cord compression. Oncology 2005; 19: 81-86.
Li KC, Poon PY. Sensitivity and specificity of MRI in detecting malignant spinal cord compression and in distinguishing malignant from benign compression fractures of vertebrae. Mag Res Imaging 1988; 6: 547-56.
Schiff D. Clinical features and diagnosis of neoplastic epidural spinal cord compression, including cauda equine syndrome. www.uptodate.com (updated 30/7/12; accessed 8/12/14).
Sorenson PS, Helweg-Larsen S, Mouridsen H, et al. Effect of high-dose dexamethasone in carcinomatous metastatic spinal cord compression treated with radiotherapy: a randomised trial. Eur J Cancer 1994; 30A: 22-27.
George R, Jeba J, Ramkumar G, et al. Interventions for the treatment of metastatic extradural spinal cord compression in adults. Cochrane Database Syst Rev 2008; CD006716.
Patchell RA, Tibbs PA, Regine WF et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised control trial. Lancet 2005; 366: 643-478.
Schiff D, Brown P, Shaffery ME. Treatment and prognosis of neoplastic epidural spinal cord compression, including cauda equine syndrome. www.uptodate.com (updated Sep 22,2014; accessed 10/12/14).
 (click to enlarge)
(click to enlarge)