Herpes zoster (commonly referred to as ‘shingles’) results from reactivation of the varicella-zoster virus which is acquired during primary varicella infection, or chickenpox. Herpes zoster is a transient illness characterised by a dermatomal rash which is often associated with significant pain. Whereas varicella is usually a disease of childhood, herpes zoster is more common in adulthood as a sporadic disease with an estimated lifetime incidence of 10-20%.1 The incidence of herpes zoster appears to increase with age, roughly doubling in each decade past the age of 50 years.1
Acute herpetic neuralgia refers to the pain preceding or accompanying the eruption of the herpes zoster rash that persists up to 30 days from its onset. Subacute herpetic neuralgia refers to the pain that persists beyond healing of the rash but which resolves within four months of onset. Pain persisting beyond four months from initial onset of the rash is known as post-herpetic neuralgia (PHN). PHN is classified as a type of neuropathic pain (NP), defined as “pain arising as a direct consequence of a lesion or disease affecting the somatosensory system”.2
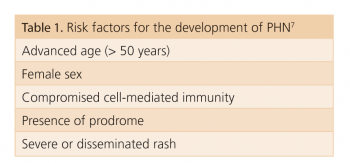
PHN is reported to develop in between 9-34% of individuals following herpes zoster and it is a debilitating complication of herpes zoster infection.3 Though the pathophysiology of PHN is unclear, studies suggest that peripheral and central demyelination, as well as neuronal destruction, is involved.4 Several clinical and laboratory parameters have been suggested and evaluated as risk factors predicting PHN5,6 (see Table 15-7). PHN can significantly impact on psychosocial functioning, resulting in impaired sleep, decreased appetite and reduced overall quality of life.8,9
Clinical manifestations of PHN
Typically herpes zoster is unilateral and is localised to a single dermatome of a single sensory ganglion. The thoracic, cervical and trigeminal nerves are most commonly affected by herpes zoster and PHN.
The pain of PHN is often intermittent and not correlated with external stimuli. Patients will often describe the character of the pain as ‘burning’.3,8 The majority of patients with PHN will also have allodynia, defined as pain evoked by normally non-painful stimuli such as light touch.10 Patients with PHN frequently describe areas of anaesthesia, along with deficits of thermal, tactile, pinprick and vibration sensation within the affected dermatomes.10 These sensory deficits may extend beyond dermatomal margins (see Table 2).
(click to enlarge)
(click to enlarge)
Treatment of PHN: Pharmacological options
Evidence suggests that antivirals used for acute herpes zoster infection may help to reduce the duration of PHN, although they do not prevent it occurring.11-13 Evidence also suggests that tricyclic anti-depressants (TCADs) used for the acute phase of herpes zoster may reduce the prevalence of PHN.14 Treatment of PHN is directed at the pain while waiting for the condition to resolve. Once PHN develops there is no cure, but a variety of medications are effective in providing pain relief. Spontaneous resolution of pain is common in patients with PHN of less than six months duration and there is little evidence to guide treatment decisions in such patients.15
For PHN of longer duration, a complex regime of oral and topical agents may be required in order to achieve effective pain relief. The choice of medication for each patient depends on a number of factors, including the potential for adverse effects, treatment of comorbidities (eg. depression and sleep disturbances), drug interactions, risks of misuse and abuse, and cost.1
Antidepressants
TCADs are effective agents in the treatment of PHN and are often thought of as the mainstay of therapy, with multiple studies demonstrating the efficacy of nortriptyline and amitriptyline.15,17
These agents work through the reuptake of noradrenaline and serotonin in the central nervous system. TCADs are limited by a slow onset of action (analgesia in days to weeks), anticholinergic side-effects (eg. dry mouth, blurred vision and urinary retention) and potential cardiac toxicity. They are, however, inexpensive and have the convenience of being administered once daily. TCADs should be started with low doses and titrated to effect and should be used with caution in the elderly.
Selective serotonin-noradrenaline reuptake inhibitors (SNRIs), such as venlafaxine and duloxetine, have also been used in the management of PHN and offer efficacy for both pain and depression with fewer adverse effects reported.18
Anti-convulsants
Sodium-channel blockers, such as carbamazepine and sodium valproate, were initially used in the treatment of PHN. Newer agents such as gabapentin and pregabalin acting via calcium-channels appear to be more effective, have a better adverse effect profile and thus are more commonly used.19,20
Pregabalin is dosed on a twice-daily schedule but may require three-times-daily dosing, similar to gabapentin, and it appears similar in terms of adverse effects, actions and efficacy. Dose-related dizziness and sedation are adverse effects of pregabalin and gabapentin that can be ameliorated by starting with low doses and titrating cautiously.21 Both require dose reduction in patients with renal insufficiency.16
Opioids
Studies have confirmed the efficacy of opioids in patients with PHN.19, 22 In one study, treatment with morphine or methadone or TCADs (desimipramine or nortriptyline) for eight weeks was significantly better than placebo.22 There was a trend towards greater pain relief with opioids, with more patients preferring opioids to TCADs.22 Opioids are associated with fewest cardiac adverse effects and may also help with sleep disturbance.18
The response of NP to opioids may be incomplete and the extent to which pain responds varies depending on both patient and pain characteristics.23 Common opioid adverse effects include constipation, nausea and sedation. Initiating treatment with low doses and titrating gradually can reduce nausea and sedation. Individualised dose titration must be employed. Tramadol, an atypical opioid analgesic, also appears effective in PHN.24
Topical agents
Topical application of capsaicin appears to be effective in the management of PHN.15,25 One study showed a 21% reduction in pain scores in those receiving capsaicin when applied four times per day, versus a 6% reduction in those receiving placebo.26
Capsaicin can cause burning, stinging and erythema and thus can be intolerable to a number of patients. The topical lidocaine 5% patch has also been shown to be effective in the management of PHN and allodynia.27,28 The patch is applied to the area over which the pain is experienced and because of the small amounts of lidocaine absorbed, systemic side-effects do not occur. Topical reactions to the patch are generally mild. Lidocaine 5% gel is also effective in PHN and allodynia.27,28
Combination therapy
In randomised controlled trials assessing efficacious medications for NP, typically < 50% of patients experience satisfactory pain relief.21 Burdensome side-effects (including inability to tolerate treatment) are also common.16 Monotherapy may be desirable for both ease of administration and reduction of potential side-effects, but this approach may not achieve satisfactory analgesic control.
A combination of medications may provide greater analgesia than monotherapy. The combination of two or more agents with different mechanisms of action at lower doses to achieve synergistic pain efficacy is not uncommon.
Treatment of PHN: Non-pharmacological
Non-drug options, including transcutaneous electrical nerve stimulation (TENS) and acupuncture, have also been evaluated in PHN and are reported to be effective.7
Prevention of herpes zoster and PHN
Much research has been conducted on the use of a vaccine against herpes zoster.29,30 Recent evidence suggests that among immunocompetent adults aged 60 years and older, receipt of the herpes zoster vaccine is associated with a lower incidence of herpes zoster.30 Evidence has also suggested lower incidence of PHN following vaccination.29 The vaccine is not recommended for immunocompromised individuals.31
Conclusion
Herpes zoster and PHN are common conditions, particularly in the elderly and in immunocompromised patients. The treatment of PHN can be extremely challenging. NP and PHN treatments have improved over the last number of years, thus presenting the clinician with many different treatment options which include anti-convulsants, antidepressants, opioids and topical agents.
Effective management of PHN may require several trials with different types of analgesics before effective pain relief can be achieved.
References
Stankus SJ, Dlugopolski M, Packer D. Management of herpes zoster and postherpetic neuralgia. Am Fam Physician 2000; 61(8): 2437-2444.
Treede RD, Jensen TS, Campbell JN et al. Neuropathic pain: redefinition and a grading system for clinical research purposes. Neurology 2008; 70: 1630-1635
Dworkin RH, Portenoy RK. Pain and its persistence in herpes zoster. Pain 1996; 67: 241-251
Christo PJ, Hobelmann G, Maine DN. Post-herpetic neuralgia in older adults: evidence-based approaches to clinical management. Drugs Aging 2007; 24(1): 1-19
Jung BF, Johnson RW, Griffin DR, Dworkin RH. Risk factors for postherpetic neuralgia in patients with herpes zoster. Neurology 2004; 62: 1545-1551
Scott FT, Leedham-Green ME, Barrett-Muir WY et al. A study of shingles and the development of postherpetic neuralgia in East London. J Med Virol 2003; 70: S24-30
Wareham DW, Breuer J. Herpes zoster. BMJ 2007; 334: 1211-1215
Johnson RW, Bouhassira D, Kassianos G et al. The impact of herpes zoster and post-herpetic neuralgia on quality-of-life. BMC Med 2010; 8; 37
Drolet M, Brisson M, Schmader KE et al. The impact of herpes zoster and postherpetic neuralgia on health-related quality of life: a prospective study. CMAJ 2010; 182: 1731
Bowsher D. Pathophysiology of postherpetic neuralgia: towards a rational treatment. Neurology 1995; 45: S56
Beutner KR, Friedman DJ, Forszpaniak C et al. Valacyclovir compared with acyclovir for improved therapy for herpes zoster in immunocompetent adults. Antimicrob Agents Chemother 1995; 39: 1546-1553
Tyring SK, Beutner KR, Tucker BA et al. Antiviral therapy for herpes zoster: randomized, controlled clinical trial of valacyclovir and famciclovir therapy in immunocompetent patients 50 years and older. Arch Fam Med 2000; 9: 863-869
Wood MJ, Johnson RW, McKendrick MW et al. A randomized trial of acyclovir for 7 days or 21 days with and without prednisolone for treatment of acute herpes zoster. N Engl J Med 1994; 330: 896-900
Bowsher D. The effects of pre-emptive treatment of postherpetic neuralgia with amitriptyline: a randomized, double-blind, placebo-controlled trial. J Pain Symptom Manage 1997; 13: 327
Alper BS, Lewis PR. Treatment of postherpetic neuralgia: a systematic review of the literature. J Fam Pract 2002; 51:121.
Dworkin RH, O’Connor AB, Audette J et al. Recommendations for the Pharmacological Management of Neuropathic Pain: An Overview and Literature Update. Mayo Clin Proc 2010; 85(3): S3-S14
Wu CL, Raja SN. An update on the treatment of postherpetic neuralgia. J Pain 2008; 9(1[1]): S19-S30
Sampathkumar P, Drage L, Martin D. Herpes zoster and postherpetic neuralgia Mayo. Clin Proc 2009; 84 (3): 274-280
Rowbotham MC, Reisner-Keller LA, Fields HL. Both intravenous lidocaine and morphine reduce the pain of postherpetic neuralgia. Neurology 1991; 41: 1024
Sabatowski R, Gálvez R, Cherry DA et al. Pregabalin reduces pain and improves sleep and mood disturbances in patients with post-herpetic neuralgia: results of a randomised, placebo-controlled clinical trial. Pain 2004; 109(1-2): 26-35
O’Connor AB, Dworkin RH. Treatment of neuropathic pain: an overview of recent guidelines. Am J Med 2009; 122, S22-S32
Raja SN, Haythornwaite JA, Pappagallo M et al. Opiods versus antidepressants in postherpetic neuralgia: a randomised, placebo-controlled trial. Neurology 2002; 59: 1015
Watson CP, Watt-Watson JH, Chipman ML. Chronic non-cancer pain and the long term utility of opioids. Pain Res Manage 2004; 9: 19-24
Boureau F, Legallicier P, Kabir-Ahmadi M. Tramadol in post-herpetic neuralgia: a randomized, double-blind, placebo-controlled trial. Pain 2003; 104: 323
Bernstein JE, Korman NJ, Bickers DR et al. Topical capsaicin treatment of chronic postherpetic neuralgia. J Am Acad Dermatol 1989; 21(2[1]): 265-270
 (click to enlarge)
(click to enlarge)
