A team from Trinity College Dublin describes the protocol involved in the assessment of elderly patients for transcatheter aortic valve implant (TAVI) and the role of the cardiology CNS
Ms Sinéad Teehan, Cardiology Clinical Nurse Specialist, St James’s Hospital, Dublin, Prof Gabrielle McKee, Associate Professor of Biological Sciences, School of Nursing and Midwifery, TCD and Dr Orla Dempsey, Quantitative Healthcare Lead, Centre for Practice and Healthcare Innovation, TCD
Aortic stenosis (AS) is the most prevalent valvular heart disease and the third most common cardiovascular condition, after coronary artery disease and hypertension.1 Severe AS has been documented in 2-7% of patients greater than 65 years of age with incidence higher in men than in women.2 Transcatheter aortic valve implant (TAVI) was introduced for patients with severe AS in 2002,3 as the shift from surgery for highly symptomatic elderly patients, to less invasive procedures reached the field of heart valves.
This new innovative cardiology procedure is rapidly evolving to treat inoperable AS patients and has been introduced into some hospitals in Ireland. This article describes the protocol and algorithms involved in the assessment of older patients for TAVI and the role of the clinical nurse specialist (CNS) in this.
Background
The number of Irish people over the age of 65 is expected to increase by almost 50% between 2011 and 2026.4 As a result, the burden of cardiac disease among older people who are highly symptomatic will continue to rise. Older age is an independent risk factor for higher mortality and morbidity in cardiac populations.
Aortic valve replacement (AVR) in otherwise fit octogenarians can be performed with a relatively low mortality and morbidity rate. Elderly patients who have a heavy burden of co-morbid diseases, which are likely to lead to complications and an increased risk of adverse outcomes, are not offered this option. However, AS is progressive and will not improve without treatment.
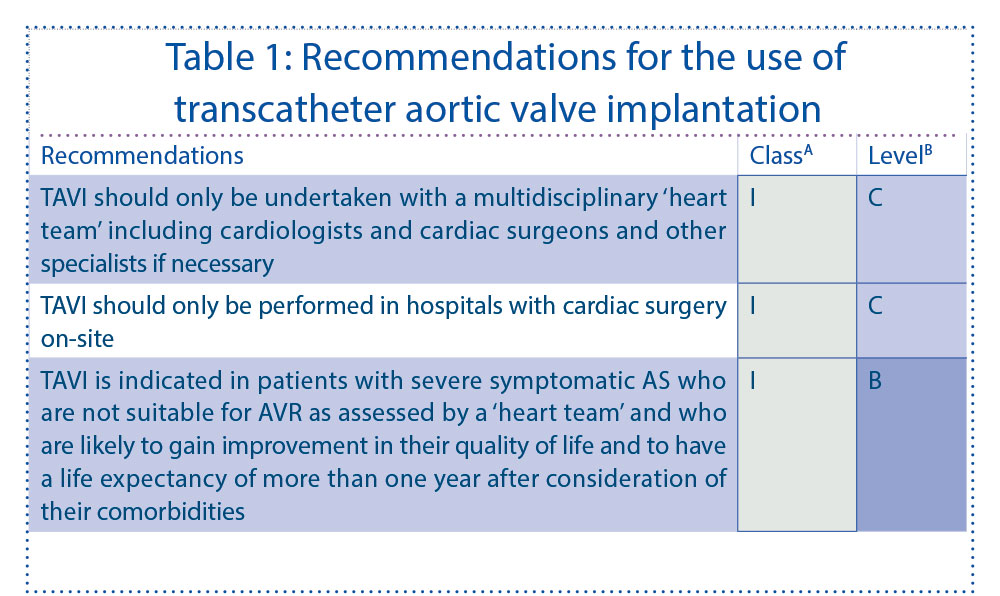
Untreated AS can lead to pulmonary hypertension, arrhythmias, endocarditis, myocardial infarction, congestive heart failure and sudden death.5 Elderly AS patients who do not have AVR intervention, have a >12 fold increase in mortality risk.6 TAVI is recommended under current ESC 2012 Guidelines for these patients, who have been deemed unsuitable for conventional open heart surgery due to multiple comorbidities.
The first TAVI case performed in an Irish healthcare setting took place in December 2008, with 93 TAVI procedures performed in St James’s Hospital, Dublin since then.
(click to enlarge)
TAVI procedure
Prior to TAVI, patients undergo thorough assessment and preparation to determine their suitability for the procedure and to ensure an informed decision is made by the patient and family. One of the first roles of the cardiology CNS is to partake in patient education to assist the patient and their family make an informed decision about their care.
Clinical decision making should be a shared process between the patient and the multidisciplinary team. As this is a relatively new treatment option in Ireland the CNS should have a good level of knowledge regarding severe AS, TAVI risks, type of procedures, benefits, perioperative and post procedural complications to sufficiently inform the patient.
There are a number of inclusion and exclusion criteria for TAVI patients.
TAVI inclusion criteria:
Symptomatic native aortic valve stenosis with an aortic valve area < 1cm2
Contraindications for surgery because of comorbidities including chronic pulmonary disease; chronic kidney disease; peripheral vascular disease; prior cardiac surgery (as agreed with cardiologist and cardiac surgeon); liver cirrhosis; hostile thoracic/chest radiation; severe cardiothoracic disease; and porcelain aorta (for femoral and subclavian approach)
Surgical Risk Score - EuroSCORE.
TAVI exclusion criteria:
Femoral, iliac or aortic pathologies
Aortic aneurysm
Carotid/vertebral artery obstruction >70%
Co-agulopathy
Cognitive impairment
MI or CVA previous month
Left ventricular thrombus
Uncontrolled atrial fibrillation
Sepsis or active endocarditis.
The work-up assessment for TAVI is performed by the multidisciplinary team; which currently includes two interventional cardiologists, a cardiothoracic surgeon, a cardiology Imaging consultant and a cardiology CNS.
Patients undergo a comprehensive work-up prior to TAVI with a full comprehensive health history, comprehensive physical examination; full blood screen including FBC, U&E, coagulation and liver profile; MRSA screen; ECG; transoesphageal ECHO; CT coronary angiogram; transthoracic ECHO; coronary and peripheral angiogram; aortogram; pulmonary function test and carotid doppler.
The CNS currently plays a major part in collating the patient history, performing a full physical examination, assessing their quality of life and level of frailty. Centres in Ireland and across Europe have dedicated advanced nurse practitioners (ANPs) for patient screening, assessment and ANP clinic evaluation. Clinical history taking is the first step in assessing AS severity. Severity is indicated by progressive symptoms such as decreased exercise tolerance or shortness of breath on exertion,7 which will need to be assessed.8 Heart failure, angina and syncope are late manifestations of this challenging disease process and may also be present.
Additional symptoms associated with underlying co morbidities, which are also important to note, need also to be assessed. Tailoring individual patient assessment, planning and intervention can be enhanced by ensuring the CNS/ANP has a good understanding of TAVI clinical outcomes. Once the full work-up is completed and patients are deemed suitable and agree to TAVI, the procedure is performed using the technique most appropriate for the patient. There are multiple access routes whereby a transcatheter valve can be deployed: transfemoral, transapical, trans-subclavian and transaortic.
Direct transaortic insertion by way of a mini-thoracotomy is the latest method over transapical approach. Percutaneous TAVI is mainly performed using a retrograde transfemoral route under local anaesthetic. In cases where there is evidence of diseased, tortuous, calcified femoral and iliac arteries the trans-subclavian, transapical, transaortic routes are assessed for suitability. All three of these methods of insertion require general anaesthetic. There are two valves currently on the market; CoreValve and Edwards Sapien. The CoreValve is a nitinol stent with porcine pericardium leaflets. The Edwards Sapien stent has a balloon expandable cobalt chromium frame with bovine pericardial tissue.
TAVI procedure requires a dedicated expert cardiac catheterisation laboratory team including nurses, doctors and cardiac technicians and in addition, coronary care unit (CCU) nurses for post procedural care.
TAVI patient outcomes
The first multicentre prospective randomised control trial of TAVI patients, the Placement of AoRtic TraNscathetER Valves (PARTNER) trial, took place in 2010. The PARTNER trial compared TAVI patient outcomes to either conventional AVR or standard medical therapy, both for severe symptomatic elderly patients. TAVI was identified as reducing mortality, when compared to surgical patients; 30-day mortality: 3.4% versus 6.5% respectively and one-year mortality 24.2% versus 26.8% respectively.9 After one year, there was no significant difference between TAVI and AVR in relation to cardiovascular death 14.3% versus 13%.10
Following this, the German Aortic Valve Registry (GARY Trial, 2011) was designed to review and govern current outcomes and to evaluate safety and effectiveness of TAVI.11 The GARY trial did not observe a significant difference in mortality between TAVI patients and CABG but it did observe a reduction in cerebrovascular complications. Similarly of the 93 patients undergoing TAVI in this Irish centre none of the patients had a complicated cerebrovascular accident, which is consistent with the experience of the GARY Registry.
Throughout the literature, the periprocedural stroke rate ranged between 0%-8%.8,12,13 It is important to note although AVR stroke rate occurred in 3% of octogenarians,14 TAVI patients have multiple co-morbidities including atherosclerosis which predisposes these patients to stroke. TAVI procedural success currently in the literature is achieved in 86-100% of cases using the transfemoral approach.12,15,16 Presently procedural mortality rates account for <10% for transfemoral implant and <14% for transapical approach.11 The Irish procedural mortality rate of 2% was in line with international findings.
Improvement in HRQOL is recognised as a therapeutic benefit specifically for elderly valve surgery patients, particularly when increased survival may be neither likely nor sought by the patient.17 There is a demonstrable lack of research focusing on HRQOL and no consensus on the definition and measurement of QOL despite Macduff highlighting the need to assess health care outcomes using HRQoL in addition to mortality and morbidity.18 The PARTNER trial, Cohort A, highlighted a remarkable improvement in HRQoL within one month of TAVI when compared to AVR; however, similar benefits occurred over the one year follow-up in both groups.
References
Baumgartner H. Aortic stenosis: medical and surgical management. Heart 2005; 9: 1483-1488
Lung B, Cachier A, Baron G et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. European Heart Journal 2003; 24(13): 1231-1243
Cribier A, Eltchaninoff H, Bash Assaf P et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human cases description. Circulation 2002; 106(24): 3006-3008
Central Statistics Office (CSO). Population and Labour Force Predictions, 2011-2041. Available at http://www.cso.ie/newsevents/pr_poplabfor2011.htm
Freeman R. Otto CM. Spectrum of calcific Aortic Valve Disease: Pathogenesis, Disease Progression and Treatment Strategies. Circulation 2005; 111(24): 3316-3326
Kojodjojo P, Gohil N, Barker D et al. Outcomes of elderly patients aged 80 and over with symptomatic, severe aortic stenosis: impact of patient’s choice of refusing aortic valve replacement on survival. Quality Journal of Medicine 2008; 101(7): 567-573
Cohn L, Narayanasamy N. Aortic valve replacement in elderly patients: what are the limits? Current Opinion in Cardiology 2007; 22(2), 92-95
Cope S, Hawley R. Needs of the older patient in the Intensive Care Unit following heart surgery. Progress in Cardiovascular Nursing 2001; 16(2): 44-48
Leon M, Smith CR, Mack M et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. New Engl JMed 2010; 363: 1597-1607
Smith CR, Leon MB, Mack MJ et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. New England Journal of Medicine 2011; 364 (23): 2187-98
Beckmann A, Hamm C, Figulla HR et al. The German Aortic Valve Registry (GARY); a nationwide registry for patients undergoing intensive therapy for severe aortic valve stenosis. Journal of Thoracic Cardiovascular Surgeon 2012; 60(5): 319-325
Rodés-Cabau J, Webb JB, Anson , et al. Transcatheter aortic valve implantation for the treatment of severe symptomatic aortic stenosis in patients at very high or prohibitive surgical risk. Acute and late outcomes of the multicenter Canadian experience. J Am Coll Cardiol 2010; 55: 1080-1090
Gotzmann M, Hehen T, Germing A et al. Short-term effects of transcatheter aortic valve implantation on neurohormonal activation, quality of life and 6-minute walk test in severe and symptomatic aortic stenosis. Heart 2010; 96: 1102-1106
Di Eusanio M, Fortuna D, De Palma R et al. Aortic valve replacement: Results and predictors of mortality from a contemporary series of 2256 patients. Journal of Thoracic Cardiovascular Surgeon. 2011; 141: 940-947
Ussia GP, Massililiano M, Barbanti M et al. Quality of life assessment after percutaneous aortic valve implantation. Eur Heart J 2009; 30 (5): 1790-1796
Piazza N, Grube E, Gerckens U et al. Procedural and 30-day outcomes following transcatheter aortic valve implantation using the third generation (18 Fr) corevalve revalving system: results from the multicentre, expanded evaluation registry 1-year following CE mark approval. Euro Intervention 2008; 4(2): 242-249
Rector TS, Cohn JN. Assessment of patient outcome with the Minnesota Living with Heart Failure questionnaire: reliability and validity during a randomized, double-blind, placebo-controlled trial of pimobendan. Am Heart J 1992; 124(4): 1017-1025
Macduff C. Respondent-generated quality of life measures: useful tools for nursing or more fool’s gold? Journal of Advanced Nursing 2000; 32(2): 375-382
Cohen DJ. Health-related quality of life after transcatheter vs. surgical aortic valve replacement in high-risk patients with severe aortic stenosis results from The PARTNER Trial (Cohort A). On behalf of PARTNER Investigators. Transcatheter Cardiovascular Therapeutics Conference; November 7, 2011. San Francisco, US
 (click to enlarge)
(click to enlarge)