Shoulder pain is a commonly encountered presentation in primary care, with around 1% of adults consulting their GP with new shoulder pain each year.1 Being the third most common musculoskeletal complaint in general practice, shoulder pain represents a significant burden of disease in the general population and in athletes.
Assessment of shoulder pain will necessarily begin with a thorough history of the presenting complaint. The pain may not be of musculoskeletal provenance; malignant, infectious, cardiac, respiratory and gastrointestinal aetiology must be ruled out. Red flag signs and symptoms in shoulder pain are described in Table 1. Furthermore, pain may arise from the neck and radiate to the shoulder. This article does not address muscular or neurological shoulder pain arising from the neck.
Table 1: Shoulder pain red flags
Symptom/sign
Suspected diagnosis
History of cancer; weight loss/night sweats;
unexplained soft tissue/bony swelling/lymphadenopathy
Malignancy
Erythema, pyrexia, systematically unwell
Septic arthritis
Loss of rotation, change in contour
Dislocation
Seizure, electric shock
Dislocation (posterior)
Trauma, pain, weakness, positive drop arm test
acute rotator cuff tear, fracture
Painless weakness or sensory changes
Neurological lesion
Common musculoskeletal causes of shoulder pain may be considered in terms of their anatomical origin:
Acromioclavicular joint (osteoarthritis)
Subacromial space disorders (impingement syndrome and rotator cuff tendinopathy, see Figure 1)
Glenohumeral disorders (frozen shoulder and osteoarthritis)
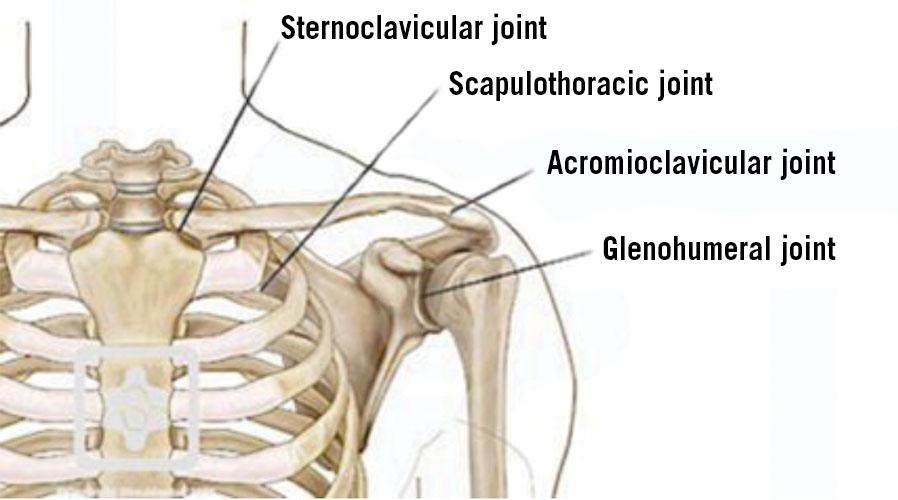
Figure1. The joints of the shoulder (reproduced with permission from Shoulderdoc.co.uk(click to enlarge)
In addition, shoulder pain can arise due to instability of the glenohumeral joint.
The age distribution of common causes of shoulder pain is shown in Table 2.
Table 2: Age distribution of causes of shoulder pain
Rotator cuff tendinopathy/impingement, AC joint OA, GH joint OA
Anatomy
The shoulder comprises four joints (see Figure 1); sternoclavicular, acromioclavicular (AC), glenohumeral (GH) and the scapulothoracic joint (the articulation of the scapula with the posterior chest).
The shallow GH joint is a ball and socket joint formed between the humeral head and the glenoid fossa of the scapula. It is reinforced by the glenoid labrum. The rotator cuff muscles (supraspinatus, infraspinatus, terres minor and subscapularis) provide a degree of stability to the GH joint in the abducted position. They also counteract the elevating force of the deltoid muscle on the humerus, preventing impingement of structures in the subacromial space between the head of the humerus and the acromion.
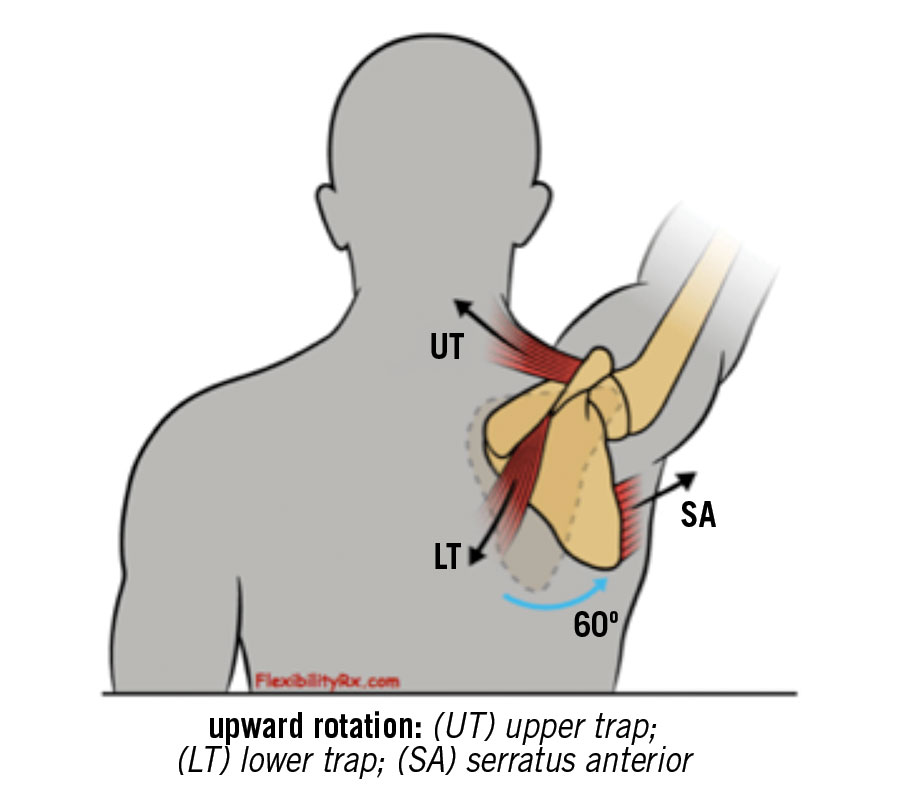
Normal shoulder movement requires coordinated interplay of the GH joint and the scapulothoracic joint using muscles as described in Table 3. By rotating the scapula, the glenoid cavity is positioned under the abducted humeral head, providing increased shoulder stability (see Figure 2).
Table 3: Muscles involved in shoulder movement
Muscle
Action
Humerous movers
Rotator cuff
- Supraspinatus
- Infraspinatus, terres minor
- Subscapularis
Abduction of humerus
External rotation of humerus
Internal rotation of humerus
Rotator cuff unit also stabilises humeral head on glenoid cavity
Deltoid
Abduction, flexion and extension of humerus
Scapula movers
Trapezius
Retraction, elevation and rotation of scapula
Serratus anterior
Protraction and lateral rotation of scapula
Pectoralis minor
Protraction and medial rotation of scapula
Levator scapulae
Elevation of scapula
Rhomboids
Retraction and medial rotation of the scapula
Figure 2. Muscles involved in scapulothoracic movement (reproduced with permission from injuryactive.com)(click to enlarge)
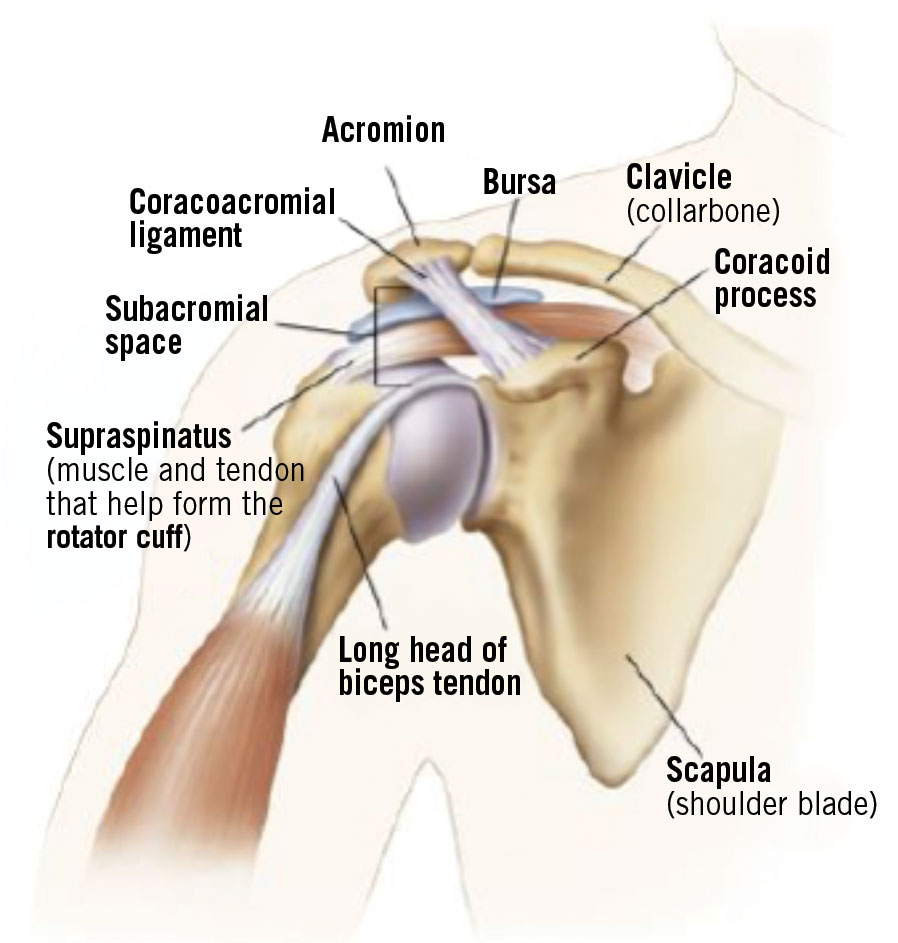
Between the humeral head and the AC joint is the subacromial space (see Figure 3). This contains the supraspinatus muscle and the subacromial bursa.
Figure 3. The AC joint, subacromial space and associated structures(click to enlarge)
The AC joint is formed by the articulation of the lateral clavicle with the acromion of the scapula. It allows for additional scapulothoracic range of motion.
Clinical assessment
History
A focused history is the most important aspect of the assessment of shoulder pain. Important elements to be covered include:
Dominant or non-dominant arm
Onset – acute, subacute, recurrent
Site of the pain
Exacerbating and relieving factors; specifically, relation of pain to movement
Nocturnal pain?
Difficulty sleeping on the affected side?
Neck pain?
Comorbidities such as diabetes, thyroid dysfunction
Cardiac, respiratory and gastrointestinal symptoms
Work and sporting activities
Impact on activities of daily living
Red flags (see Table 1).
Examination
Systematic examination of the shoulder comprises inspection, passive, resisted and active movements and special tests for impingement, AC joint OA and GH stability. The neck, shoulders, thoracic spine and scapulae should be visible.
The patient is inspected for muscle wasting, asymmetry (the dominant shoulder is usually lower than the non-dominant), scapular position (winging), spinal curvature (the ears and shoulders should be in vertical alignment) and other abnormalities such as ecchymosis, swelling, scars and colour changes.
The joint is then moved passively to assess for pain, range of motion and end feel. Passive movement allows the examiner to determine if a capsular pattern of joint restriction is present. Loss of active movement with full passive movement suggests a problem with the muscles, tendons or nerves rather than in the joint. Reduced power against resistance suggests muscle or tendon injury.
AC joint disorder
OA of the AC joint is a common finding in patients over 50 years old, with patients complaining of insidious onset pain, localised to the joint.2 The intraarticular disc of the AC joint degenerates progressively. High axial loads through the joint, eg. in bench-pressing or overhead lifting, may compound joint degeneration leading to OA. Athletes who engage in activities that result in falls onto the shoulder are also susceptible to developing OA.
On examination, the joint may be tender. Pain may also be elicited with the arm forward flexed to 90 degrees and adducted across the chest, under the chin, with passive overpressure provided by the examiner (the scarf test). Paxinos test involves moving the joint by translating the acromion anteriorly with respect to the clavicle. With the patient sitting, the examiner holds the acromion between the thumb posteriorly and the fingers anteriorly. With the other hand, the examiner holds the middle clavicle and translates the acromion anteriorly. Pain in the region of the AC joint constitutes a positive test. Diagnostic intra-articular local anaesthetic injection is possible. The joint can be appreciated by palpating a dip at the distal clavicle. Using a superior, vertical approach, it can be infiltrated with a small volume (0.5ml) of 1% or 2% lignocaine. A significant reduction in symptoms is diagnostic.
Radiographs are an appropriate initial diagnostic test.2 CT may also be used. MRI may also demonstrate degenerative changes.
Conservative management is preferred initially. This comprises activity modification, physiotherapy, NSAIDs and corticosteroid injection. The patient should avoid repetitive activities that reproduce the pain. Physiotherapy includes exercises to maintain active range of motion. Rehabilitation is focused on movements, especially retraction, that strengthen scapular muscles and stabilise the scapula. Corticosteroid injection is appropriate after failed trial of NSAIDs and physiotherapy. Care should be taken only to insert the tip of the needle into the joint space to avoid entering the GH capsule.
Referral for surgical evaluation is appropriate where at least six months of conservative measures fail to control symptoms satisfactorily.2
Subacromial disorders
Impingement syndrome
Subacromial impingement syndrome (SAIS) occurs due to mechanical compression of the subacromial structures between the acromial arch and the humerus.3 Patients have reduced subacromial space during shoulder elevation (flexion and abduction). This can be a structural or a functional issue or a combination of the two. Structural impingement arises due to the shape of the acromion or due to osteophyte formation at the AC joint or at the acromion.4 Functional narrowing of the subacromial space may occur due to glenohumeral and/or scapulothoracic muscle imbalances.
Classically, patients will complain of gradual onset pain in the lateral, proximal upper limb occurring with overhead activities.4 Degenerative changes causing structural narrowing of the subacromial space are more likely over the age of 35. Younger patients involved in repetitive overhead activities such as swimming and tennis may experience a functional narrowing of the subacromial space.
On examination, the patient may experience a ‘painful arc’ whereby pain occurs between 60 and 120 degrees of active shoulder abduction, easing after 120 degrees. This test may also be positive with RC tendinopathy.
The Hawkins test compresses all structures in the subacromial space, ie. supraspinatus and the subacromial bursa. The patient’s arm is placed in 90 degrees of forward flexion, with the elbow flexed to 90 degrees. The shoulder is then passively internally rotated. The test is positive if symptoms are reproduced with internal rotation of the shoulder.
In the older patient, AP x-ray is the imaging modality of choice for demonstrating degenerative AC joint changes.2 It may also show a narrow subacromial space. In the younger patient, MR arthrogram will reveal partial RC tears and any GH joint capsule ligamentous changes.
Management of SAIS will involve a period of relative rest where the patient will avoid aggravating activities. Simple analgesia and NSAIDs may be prescribed. Physiotherapist assessment is appropriate for addressing muscle imbalances involving the scapula and for management of RC imbalances (and GH joint tightness). If symptoms are not adequately controlled by analgesia, a corticosteroid injection into the subacromial space may be appropriate. Surgical intervention may be appropriate after failure of conservative measures.
Rotator cuff tendinopathy and tears
Rotator cuff tendinopathy is the most common cause of shoulder pain.1 It is an overuse condition, resulting from failure of regeneration of tendons. This may arise due to an intrinsic disorder of the tendon due to the ageing process, due to impingement of the tendon in the subacromial space or a combination of the two.5 It typically occurs in sports requiring repetitive overhead movement of the shoulder.
Patients typically complain of gradual onset shoulder pain, worsened by overhead activities.6 They may also experience weakness and stiffness of the shoulder. On examination, resisted testing of the external rotators and supraspinatus may reveal weakness and pain.
RC integrity is tested by resisted movements as follows:
Supraspinatus – resisted abduction
Infraspinatus, terres minor – resisted external rotation
Subscapularis – resisted internal rotation.
Supraspinatus pathology can also be tested using the ‘full can’ test. The arm is elevated to 90 degrees in the scapular plane, with the thumb pointing upwards. Pain and/or weakness against resistance suggest supraspinatus pathology.
Patients with RC tendinopathy also tend to present symptoms and examination findings consistent with subacromial impingement.
References
Murphy R, Carr A. Management of Shoulder Pain in General Practice. InnovAIT. 2009;2(7):402-407
Docimo S, Kornitsky D, Futterman B, Elkowitz DE. Surgical treatment for acromioclavicular joint osteoarthritis: patient selection, surgical options, complications, and outcome. Curr Rev Musculoskelet Med. 2008; 1:154-160
Page P. Shoulder Muscle Imbalance and Subacromial Impingement Syndrome in Overhead Athletes. IJSPT. 2011;6:51-58
Funk L. Shoulder Impingement in Athletes. Shoulderdoc.co.uk. Undated. [updated 2018 May 5th; cited 2018 May 13th]. Available from https://www.shoulderdoc.co.uk/article/1602
Factor D, Dale B. Current Concepts of Rotator Cuff Tendinopathy. IJSPT. 2014;9(2): 274-288
Leung R. Common Sports Related Shoulder Injuries. InnovAIT. 2017; 10(1): 20-38
Brukner P, Khan K. Brukner & Khan’s Clinical Sports Medicine (5th ed.). Sydney: McGraw-Hill Education; 2017
Sigh H, Goyal M. Physiotherapeutic Management of Adhesive Capsulitis: A Review of Literature. Int J Physiother Res. 2016;4(6):1719-27
Mitchell C, Adebajo A, Hay E, Carr A. Shoulder pain: diagnosis and management in primary care. BMJ. 2005;331(12):1124-8
GP Notebook. Frozen Shoulder. Undated. Available from http://www.gpnotebook.co.uk/simplepage.cfm?ID=x20060119003135725580&linkID=69021&cook=yes
 Figure1. The joints of the shoulder (reproduced with permission from Shoulderdoc.co.uk(click to enlarge)
Figure1. The joints of the shoulder (reproduced with permission from Shoulderdoc.co.uk(click to enlarge)