Focus on treatment and management of venous leg ulcers
Dr Gerry Morrow, Medical Director, Clarity Informatics, Clayton House, Clayton Road, Newcastle Upon Tyne NE2 1TL, United Kingdom and Mr Ross Ferguson, Clinical Author, Clarity Informatics, UK
A leg ulcer is defined as the loss of skin below the knee on the leg or foot, which takes more than two weeks to heal.1 Venous leg ulceration is caused by problems of high pressure in the veins of the leg. In a normal leg vein, pressure decreases with exercise as a result of the calf muscle pump, and valves in the veins prevent reflux of blood. If these valves are incompetent, or the muscle pump is impaired, the pressure in the vein remains high, which can cause ulcers.
Venous leg ulcers are a common, chronic, recurring condition, with an estimated prevalence of between 0.12% in people under the age of 70, rising to 1.03% in people over the age of 70 in Ireland.2
Risk factors for venous leg ulcers include obesity, immobility, personal/family history of varicose veins, history of deep vein thrombosis, arteriovenous fistula, increasing age and a history of leg fracture or trauma.3 Healing rates of 70% at six months have been achieved for small venous leg ulcers managed in some specialist clinics but recurrence is common and ranges from 26-69% within 12 months.
To diagnose a leg ulcer, take the patient’s history and ask about the following:
• Symptoms of venous insufficiency, such as leg pain, aching or heaviness, skin itching, odour, exudate, swelling, hyperpigmentation and eczema
• Risk factors which suggest a venous cause for ulceration, such as immobility, obesity, varicose veins or a history of deep vein thrombosis
• Smoking, high blood pressure, ischaemic heart disease and raised cholesterol
• A history of diabetes mellitus or rheumatoid arthritis
• Previous injury at the site of the ulcer, or previous ulcers or skin malignancy
• How symptoms are affecting the person’s quality of life.
(click to enlarge)
Examination
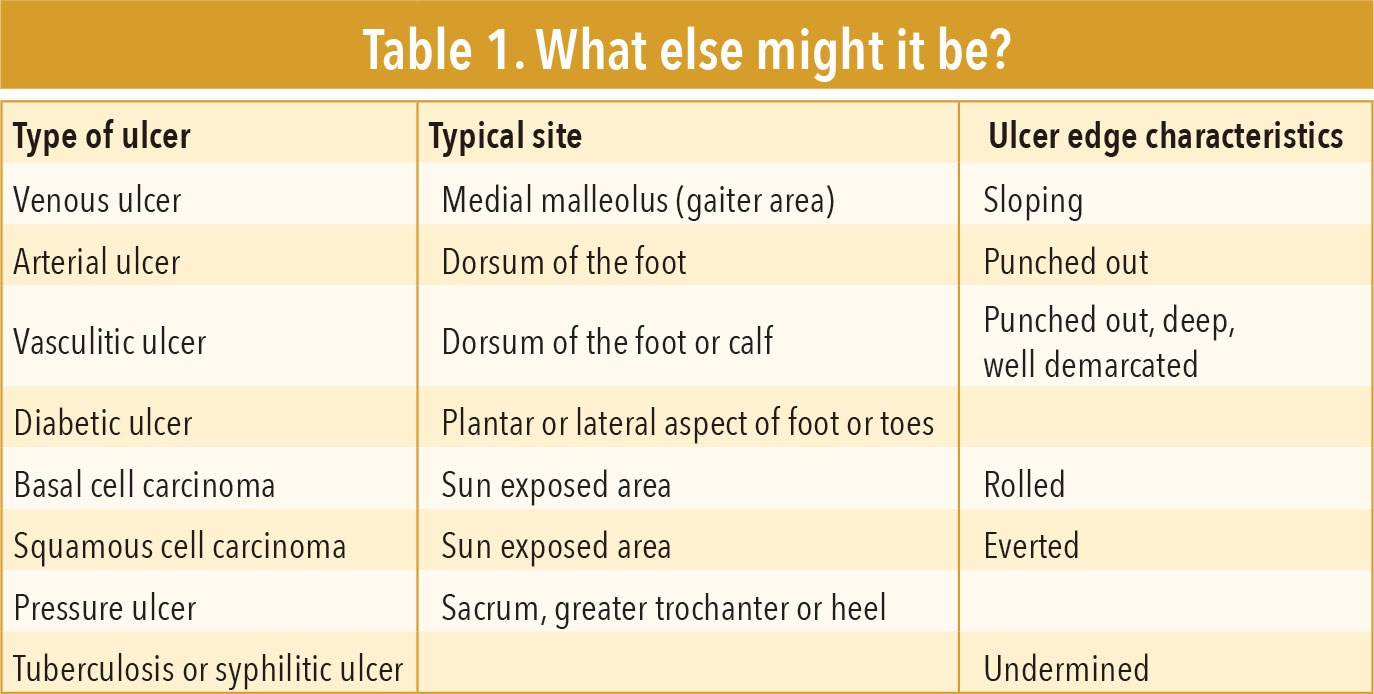
• Assess the site and edge of the ulcer
• Record details about the ulcer, to compare at follow up:
– Size and depth – trace out the ulcer margin onto a transparent sheet, or take a photograph. Take measurements of the greatest depth of the ulcer, noting any exposed underlying tissue
– Wound bed – look for granulation, fibrous or necrotic tissue and for exudate to help determine which dressing is needed
– The position of the ulcer (medial, lateral, anterior, posterior or a combination)
– Examine both legs, looking for signs of chronic venous problems, such as oedema, pigmentation and eczema.
Infection
Look for signs of infection, such as an enlarging ulcer, increased discharge or pain, raised temperature, foul odour, or cellulitis, where the surrounding skin is painful, red, hot, swollen and tender. Examine the person for evidence of varicose veins. Assess for possible arterial disease by assessing capillary refill (greater than four seconds is suggestive of arterial insufficiency) and checking peripheral pulses.
Arrange a Doppler assessment of both legs to determine the ankle brachial pressure index (ABPI) to exclude arterial insufficiency. The ABPI provides a measure of vessel competency by giving a ratio of systolic blood pressure at the ankle compared to that in the arm. A value of 1.0 is normal. A ratio of:
• <0.5 indicates severe arterial insufficiency – compression treatment is contraindicated and indicates the need for urgent referral to a vascular surgeon
• Between 0.5 and 0.8 indicates arterial disease. These people should be referred to a vascular surgeon and compression bandaging should usually be avoided. However, reduced compression can be used under strict supervision if the ulcer is clinically venous and the healthcare professional has sufficient experience
• > 0.8 indicates that compression may be safely applied.
Be aware that the ABPI may decrease with time. Arterial disease can develop in people with venous leg ulcers, and the ABPI will also reduce with increasing age, so will need to be rechecked periodically.
ABPI may not be reliable in people with diabetes mellitus, atherosclerotic disease, rheumatoid arthritis and systemic vasculitis. These conditions can give falsely high ABPI readings due to hardening of blood vessels. Arrange blood tests including a full blood count to rule out anaemia, which may delay healing; high white cell count may indicate infection.
Dressings and compression
Ensure the ulcer is irrigated at each dressing change with warm tap water or saline, then dried. Ensure slough, necrotic, fibrous or excess granulation tissue is removed by gentle washing. Debridement is not usually necessary. Ensure low-adherent dressings are applied and replaced weekly. If the wound has a heavy exudate, more frequent bandage changes may be required.
Alternative dressings may be considered to help with pain (hydrocolloid), heavy exudate (alginate) or slough (hydrogels). Ensure dressings for infected ulcers are replaced daily to assess for clinical improvement.
The most effective level of compression to overcome venous hypertension is around 40mmHg at the ankle. To achieve this pressure in a range of limb diameters, bandaging regimens must be adjusted according to ankle circumference. Ensure below-knee, graduated multi-layer high compression bandaging is applied and replaced weekly. For people who are immobile, four-layer or three-layer bandaging is more suitable. For people who are mobile, two-layer bandaging is more practical.
Do not use compression therapy if Doppler studies show an ABPI of ≤ 0.8, or if there is active phlebitis or infection, deep vein thrombosis, or cellulitis. If a venous leg ulcer becomes infected and compression bandaging is already being used, ensure the bandaging is removed, and restart compression therapy once the infection has resolved. Consider seeking advice on a prescription for pentoxifylline which may aid ulcer healing.
Provide lifestyle advice to reduce the risk of recurrence, including:
• Keep mobile with regular walking
• Elevate the legs when immobile
• Avoid injuries and wear well-fitting footwear
• Apply a non-sensitising emollient frequently
• Examine the legs regularly for broken skin, swelling or redness
• Lose weight (if necessary), eat a balanced diet (malnutrition impairs ulcer healing), only drink alcohol within recommended levels and stop smoking
• Wear the appropriate grade and type of compression stockings, ideally for a minimum of five years. Lifelong use of compression stockings may be considered in people with recurrent venous leg ulcers.
Class III (high) below-knee compression stockings should be recommended for most people but, if not tolerated, class II (medium) stockings should be used. Compression stockings should be put on first thing in the morning before getting out of bed.
Follow up
Ensure the ulcer is reassessed; uncomplicated ulcers should be assessed at least weekly for the first two weeks. If the ulcer is healing, this can be extended to fortnightly or monthly, and at three monthly intervals thereafter, depending on judgement. Ideally, people should be reassessed for skin complications within 24 to 48 hours of starting compression therapy. Check for complications related to:
• The ulcer – infection, sinus formation or fistula
• Compression bandaging – pressure damage or arterial insufficiency. Compression bandages should be removed immediately if the person experiences a change in foot colour or temperature, or increased pain. Seek further advice if there is no improvement after removing the bandages
• The dressings used – these can cause skin maceration or allergic contact dermatitis
• Ensure Doppler studies are carried out at the first sign of ulcer deterioration, ulcer recurrence, sudden increase in ulcer size or pain, or change in foot colour or temperature at three monthly intervals until the ulcer has healed and at six monthly intervals thereafter.
Management of infected venous leg ulcers involves:
• Taking a swab, ensuring that prior to this the infected ulcer is cleaned with tap water or saline
• Prescribing an antibiotic, such as flucloxacillin (or clarithromycin if the person is allergic to penicillin) for seven days, while awaiting swab results. The use of topical antibiotics is not recommended
• Ensure people with an infected venous leg ulcer are followed up daily or every two to three days until improvement is seen
• If infection is not showing signs of improvement check swab results and consider changing the antibiotic.
Pain management in venous leg ulcer
Determine the duration, nature and severity of the pain to exclude an additional underlying cause, such as arterial disease, diabetic neuropathy or cellulitis.
Venous leg ulcers are often painful, which may be constant or intermittent. Severe or worsening pain may indicate a complication. Constant pain can originate from vascular structures, pitting oedema, or infection. Intermittent pain can be related to dressing changes or debridement procedures.
Give advice about analgesia for pain relief, such as paracetamol or codeine, as needed. Advise the person that leg elevation may also help with the pain associated with oedema. To manage oedema in venous leg ulcers ensure the person is using compression bandaging, if appropriate. Advise the person to elevate their legs for 30 minutes, three to four times a day, and consider placing pillows under their feet and legs while sleeping. Exclude other causes of oedema such as medication (for example calcium-channel blockers) and heart failure.
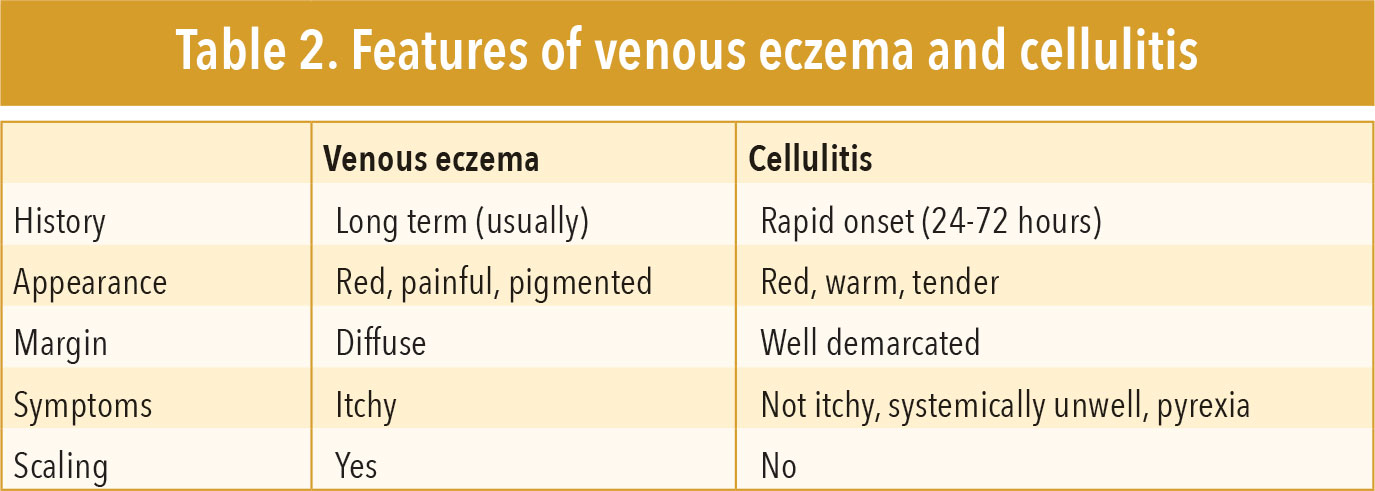
To manage eczema exclude the possibility of cellulitis if there is worsening venous eczema and signs of active infection.
Table 2 outlines the features of venous eczema and cellulitis. If there is no clinical improvement, or allergic contact dermatitis is suspected, refer the person to a skin specialist. Common skin sensitisers include wool alcohols (lanolin), topical antibiotics, topical corticosteroids, cetyl stearyl alcohols, parabens and rubber mixes.
(click to enlarge)
Consider referral to a specialist leg ulcer clinic, or to a dermatology or vascular specialist, if there is:
• An uncertain diagnosis
• A suspected alternative cause of ulceration such as arterial or mixed venous/arterial ulcer, suspected malignant ulcer, rapidly deteriorating ulcer, cellulitis, osteomyelitis or sepsis, atypical appearance or distribution of ulcers
• A complication related to the ulcer or treatment
• Uncontrolled pain
• An ulcer that has not healed after two weeks of treatment in primary care
• A recurrent ulcer.
References
Varicose veins : diagnosis and management. NICE Guidelines [CG168], July2013. Available from: https://www.nice.org.uk/guidance/cg168
O’Brien JF, Grace PA, Perry IJ, Burke PE. Prevalence and aetiology of leg ulcers in Ireland. Ir J Med Sci 2000; Apr-Jun;169(2):110-112. Abstract available from: http://www.ncbi.nlm.nih.gov/pubmed/11006665
Management of chronic venous leg ulcers. SIGN, August 2010. Available from: http://www.sign.ac.uk/guidelines/fulltext/120/
Venous leg ulcers. Royal College of Nursing 2006. Available from: https://www2.rcn.org.uk/development/practice/clinicalguidelines/venous_leg_ulcers
Grey JE, Harding KG, Enoch S. Venous and arterial leg ulcers. BMJ 2006; Feb 11; 332(7537): 347–350. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1363917/
 (click to enlarge)
(click to enlarge)