Metronomic chemotherapy in advanced metastatic breast cancer
Symptomatic relief with a favourable side-effect profile is possible with the use of metronomic chemotherapy in patients with advanced metastatic breast cancer
Prof Seamus O'Reilly, Consultant Medical Oncologist, Cork University Hospital, Cork, Dr Jodie Battley, Medical Oncology Registrar, Cork University Hospital, Cork and Ms Louisa Jane McSweeney, Graduate Entry Medical Student, University College Cork, Cork
A 57-year-old woman with metastatic breast cancer demonstrated a prolonged response to metronomic chemotherapy without significant toxicity. This is a potentially novel approach for controlling advanced cancer.
Case report
In 2010 the patient was diagnosed with a multifocal grade 3, node-positive, hormone-sensitive, HER2-negative right breast cancer and treated with neo-adjuvant chemotherapy. Pre-operative imaging revealed pathological left axillary adenopathy. A re-staging computed tomography (CT) scan demonstrated small volume mediastinal lymphadenopathy and a left upper lobe lung nodule of indeterminate significance. The patient underwent right mastectomy and bilateral axillary clearance with subsequent adjuvant radiotherapy followed by endocrine therapy with letrozole. A surveillance scan performed in February 2011 demonstrated no convincing evidence of metastatic disease.
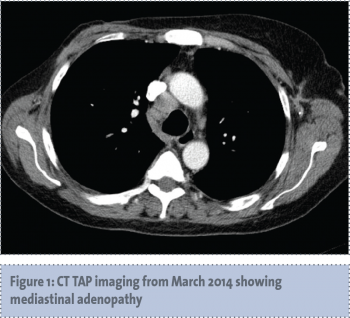
Three years later, in March 2014, the patient re-presented with symptomatic anaemia, and 13kg weight loss over the preceding five months. A restaging CT scan demonstrated recurrent mediastinal lymphadenopathy, multiple liver lesions and extensive bony metastases (see Figures 1-3).
(click to enlarge)
(click to enlarge)
(click to enlarge)
A liver biopsy confirmed moderately differentiated oestrogen receptor-positive metastatic adenocarcinoma consistent with a breast primary. Tumour markers were elevated with a CA 15-3 of 1236 and CEA of 71. Elevated hepatic enzymes precluded paclitaxel chemotherapy; in May 2014 the patient was commenced on metronomic chemotherapy with cyclophosphamide 50mg and capecitabine 500mg three times daily given on a continuous basis along with monthly zoledronic acid. Within a month the patient reported significant improvement in fatigue, pain and appetite with associated weight gain. She had no significant chemotherapy-related side-effects. Tumour markers had fallen, indicating a serological response with significant improvement in liver enzymes (see Figures 4 and 5). The patient remains on this regimen; she is clinically well with ongoing improvement in tumour markers and no evidence of treatment-related toxicity.
(click to enlarge)
(click to enlarge)
Discussion
Standard chemotherapy regimens are titrated to the maximum tolerated dose (MTD), the dose at which tumour regression can be achieved with acceptable levels of toxicity. While standard MTD regimens target rapidly dividing cancer cells, they also destroy the endothelial cells forming the lining of the new vessels that support tumour growth.1 The toxicity of the standard MTD regimens necessitates chemotherapy-free periods for the mitigation of collateral damage to healthy cells. These drug-free periods, however, also allow endothelial cells to generate and tumour angiogenesis to occur.2
Tumour cells depend on the presence of vascular endothelial growth factor (VEGF), a key mediator of angiogenesis, for the production of vessels comprising their blood supply.1 VEGF must bind to specific receptor tyrosine kinases in order to initiate the signalling pathway that ultimately results in new vessel formation. By targeting these receptor proteins or VEGF itself, the signalling pathway can be disrupted thereby preventing the formation of new vessels required by the tumour to sustain its growth.
This effect is achieved with MTD regimens, however, the VEGF-mediated signalling cascade is believed to re-commence during the periods between treatment cycles.2 Metronomic chemotherapy is defined as ‘the frequent, even daily, administration of chemotherapeutics at doses significantly less than the maximum tolerated dose, with no prolonged drug-free breaks’.3 Metronomic chemotherapy halts tumour angiogenesis by maintaining this disruption of VEGF-mediated angiogenesis. The lower doses used in metronomic dosing and administered daily without break, are not strong enough to target tumour cells specifically, but are sufficient to cause a sustained inhibition of VEGF mediated angiogenesis.4
The notion of daily low-dose use of chemotherapeutic agents was first raised at the turn of the millennium.5,6,7 In recent years, multiple studies have demonstrated clinical benefit without significant toxicity in patients with advanced metastatic breast cancer.4,7 Such toxicity as is experienced with metronomic chemotherapy is considerably milder than with MTD, and does not occur in all cases.
In 2011, Lobna et al examined the effect of metronomic capecitabine 500mg twice daily and cyclophosphamide 50mg daily on VEGF levels in 60 patients with metastatic breast cancer. They reported a response rate of 21.7%, and an overall disease control rate of 56.71%. The median time to progression was reported as 7 ± 2.59 months, with an overall survival of 16 ± 8.02 months.8 Considerable falls in levels of VEGF from baseline were observed in all cases, and the magnitude of the decrease in circulating VEGF was in line with the clinical response, ie. those who achieved complete response or stable disease had lower VEGF levels than those with progressive disease. Disease progression occurred in all four patients in the study with similar metastatic disease to our patient, ie. liver, lung, bone and soft tissue metastases. Statistically significant decreases in VEGF levels from baseline were, however, observed within these patients.
The patient described in this case report, despite having a similar pattern of metastases to the four patients referred to in the Lobna study, achieved a very significant response from the metronomic treatment regimen. It should be noted that where Lobna et al described the use of capecitabine 500mg twice daily and cyclophosphamide 50mg daily,8 our patient received cyclophosphamide 50mg and capecitabine 500mg three times daily.
Conclusion
This case report demonstrates that symptomatic relief with a favourable side-effect profile is possible with the use of metronomic chemotherapy in patients with advanced metastatic breast cancer, and offers such patients a promising opportunity for substantial improvements in quality of life and may be associated with several months progression-free survival.
References
Folkman J. Angiogenesis in cancer, vascular, rheumatoid and other disease. Nat Med 1995; 1(0): 27-31.
Bocci G, Tuccori M, Emmenegger U, et al. Cyclophosphamide-methotrexate ‘metronomic’ chemotherapy for the palliative treatment of metastatic breast cancer. A comparative pharmacoeconomic evaluation. Ann Oncol 2005; 16: 1243-1252.
Dellapasqua S, Bertolini F, Campagnoli E, et al. Metronomic cyclophosphamide and capecitabine combined with bevacizumab in advanced breast cancer. J Clin Oncol 2008; 26(30): 4899-4905.
Emmenegger U, Man S, Shaked Y, et al. A comparative analysis of low-dose metronomic cyclophosphamide reveals absent or low-grade toxicity on tissues highly sensitive to the toxic effects of maximum tolerated dose regimens. Cancer Res 2004; 64: 3994-4000.
Browder T, Butterfield CE, Kraling BM, et al. Antiangiogenic scheduling of chemotherapy improves efficacy against experimental drug-resistant cancer. Cancer Res 2000; 60: 1878-1886.
Eberhard A, Kahlert S, Goede V, et al. Heterogeneity of angiogenesis and blood vessel maturation in human tumors: implications for antiangiogenic tumor therapies. Cancer Re 2000; 60: 1388-1393.
Man S, Bocci G, Francia G, et al. Antitumor and anti-angiogenic effects in mice of low-dose (metronomic) cyclophosphamide administered continuously through the drinking water. Cancer Res 2002; 62: 2731-2735.
Lobna R, El-Arab E, Swellam M, et al. Metronomic chemotherapy in metastatic breast cancer: Impact on VEGF. J Egypt Nat Cancer Inst 2012; 24: 15-22.
 (click to enlarge)
(click to enlarge)



