Migraine is the most common headache disorder seen in general practice. Patients may experience episodic or chronic symptoms, the latter associated with significant disability and a major impact on quality of life. There can be a component of overuse of painkillers or analgesics in patients with more chronic symptoms. There is an increased risk of certain medical comorbidities in patients with chronic migraine including depression, anxiety, fibromyalgia and obesity. In this module we focus on migraine prevention strategies.
Each patient can play a vital role in helping themselves. It is important to emphasise to patients the value of conservative management strategies in conjunction with preventative medication. These include:
Healthy lifestyle
Daily exercise (moderate intensity for a minimum of 20-30 minutes at least five days a week),
Balanced diet, good hydration, moderate caffeine intake (which should not exceed two or three 300ml cups daily),
Good sleep hygiene
Appropriate stress management.
Lifestyle modifications may include practical issues, for example not getting up for 5am flights on holidays. As many migraine sufferers know, any change in their daily routine can precipitate a migraine. Stress is a trigger in over 70% of migraine sufferers.
Dietary management of migraine should include a regular eating pattern. Patients should be advised to avoid skipping meals. Vitamin and mineral supplementation: riboflavin (vitamin B2, 400mg daily), magnesium and CoQ10, may be effective in reducing migraine frequency but evidence has not been substantiated by randomised double-blind clinical trials. A review of magnesium trials suggested that using high levels of magnesium dicitrate (600mg) seems to be a safe but results are anecdotal.
Improving lifestyle factors alone may improve headaches and severity. The patient organisation, the Migraine Association of Ireland (MAI), provides very helpful information and support in this regard. The MAI website www.migraine.ie also has a section specifically for health professionals and organises training and research days for healthcare professionals on an annual or bi-annual basis.
Oral therapies for prevention
Prophylactic oral therapies are usually indicated for the treatment of migraine when migraine symptoms occur on at least 8-10 days per month and are of moderate to severe intensity. Acute medications can be taken on average four to six days per month, but preferably not more often due to the risk of medication overuse.
Pain freedom at two hours is considered to be a good response to acute treatment and is the standard measure used for efficacy in clinical trials. A pragmatic management approach needs to be taken with patients who experience an intermediate frequency of migraine symptoms (on average six to eight days per month).
Prophylactic therapies should be started after the patient has been assessed to determine an appropriate agent. However, patients should be advised that most preventative medications do not work effectively in the presence of medication overuse.
For optimal efficacy, it is recommended that for each preventative agent:
Start at a low dose
Increase the dose in small increments every two to eight weeks
Give an adequate trial for two to three months at the maximum tolerated dose
Avoid overuse of analgesics or painkillers
Discuss contraception with women of childbearing age and the potential risk of these preventative medications, primarily during pregnancy and breastfeeding
Consider comorbid medical conditions and aim to use a single medication that may treat multiple disorders if possible (for example, candesartan for hypertension and migraine)
Re-evaluate therapy at a reasonable interval of three to six months, preferably with the help of a migraine diary.
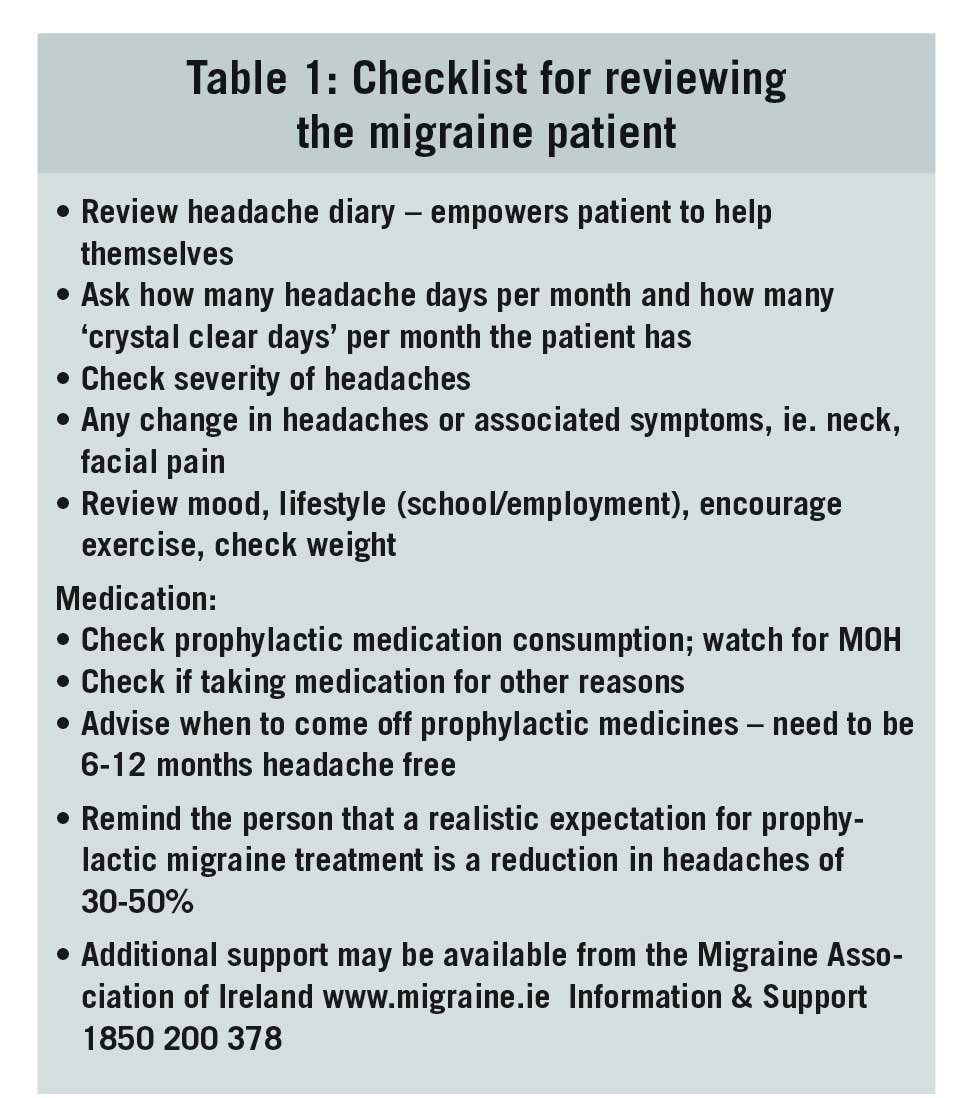
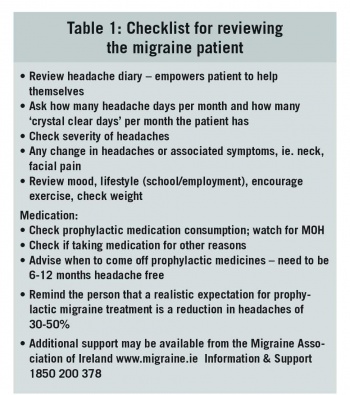
A realistic goal is that a preventative drug should give at least a 30-50% improvement in headache disability overall, without having significant side-effects. If this level of improvement is not achieved at the maximum tolerated dose, strong consideration should be given to weaning off the medication after a three to six-month period (see Table 1 for pro-forma for follow-up of the patient with migraine).
(click to enlarge)
It is recommended that patients should be involved in the decision regarding the choice of preventative treatment to improve medication compliance. This discussion should include the realistic benefits and possible side-effects of the proposed treatment.
The headache impact test (HIT-6) is a patient questionnaire used at the three-to six-monthly review. It gives the patient an opportunity to describe and communicate the way they feel and how the headaches impact on their daily lives. It was developed from SF-36 health assessment tool. It can be accessed http://neurohealth.info/wp-content/uploads/2010/10/hit6.pdf
Most of the current preventative agents used in Ireland were identified by chance, having been used to treat other medical conditions including epilepsy, depression and hypertension.
First-line options
Topiramate (25-400mg daily), beware of teratogenicity, can be used in the presence of medication overuse
Amitriptyline (2.5-150mg daily) or less sedating, nortriptyline
Propranolol (20-160mg daily)
Candesartan (4-32mg daily).
These are the most frequently prescribed preventative agents in Ireland. Medications used may vary from country to country, and are strongly influenced by personal experience.
Second-line options
Sodium valproate (200-2,000mg daily) beware of teratogenicity
Pizotifen (3-4.5mg daily)
Metoprolol (50-100mg daily); bisoprolol, atenolol
Venlafaxine (37.5-225mg daily)
Gabapentin (300-3000mg daily)
Physiotherapy
Acupuncture
Menstrual-related migraine – offer long-acting triptan on days -2 to +3.
With these therapies it is helpful if patients are given a trial of at least three of the above first-line or second-line prophylactic medications in general practice before considering referral to a specialist hospital-based headache clinic. It is interesting to note that studies have shown that more than 80% of chronic migraine patients discontinued prophylactic treatment within one year. A sizeable decrease in adherence was observed after the first month.
Epilepsy medications for prevention
Topiramate (25-400mg daily) has been found to significantly improve migraine in randomised controlled trials (RCTs). The usual starting dose is 25mg once-daily, titrated upwards in 25mg increments every two to eight weeks up to a maintenance dose of between 25-200mg BD. The dose of topiramate used in epilepsy can be up to 700-800mg daily. However, the maximum dose routinely used in migraine is 400mg daily. The maintenance dose achieved depends on tolerability and efficacy.
Common side-effects of topiramate include weight loss, tingling of fingers and toes, cognitive dysfunction, worsening of depression/anxiety and insomnia. As migraine is most common in women of childbearing years, female patients should be strongly advised to avoid pregnancy while taking topiramate due to the risk of foetal abnormalities.
The combined oestrogen contraceptive (which should usually only be prescribed for migraine patients without aura) may be rendered less effective (and may cause breakthrough bleeding and result in pregnancy) when the dose of topiramate is increased above 200mg daily.
Sodium valproate (200-2,000mg daily) may be effective for migraine prophylaxis and is reasonably well tolerated in both episodic and chronic migraine patients. However, valproate can cause birth defects and should not be used in female patients of childbearing age. Studies have shown that patients were more than twice as likely to have their headache frequency reduced by 50% or more with sodium valproate than they were with placebo.
The most common starting dose is 200mg once or twice daily. The typical maximum maintenance dose for migraine is 1,000mg twice daily. Potential side-effects include tremor, weight gain and hair loss. Side-effects are normally dose dependant.
Gabapentin (300-3,000mg) has not been found to be effective for prophylaxis of migraine in adults. Side-effects include dizziness, weight gain and somnolence.
Pregabalin does not have strong evidence for prophylactic use in migraine, although it is frequently prescribed. Common side-effects include dizziness and weight gain. It should be prescribed with caution, due to its current value as a ‘street’ drug.
Zonisamide (100-200mg daily) has showed benefit in an open label study in refractory patients. It was mainly used in patients who responded to topiramate, but could not tolerate the side-effects. Like topiramate, zonisamide used at a dose greater than 200mg daily may cause breakthrough bleeding and result in pregnancy.
Anti-epileptics other than those mentioned above have been used in migraine prophylaxis. They include acetazolamide, carbamazepine, clonazepam, lamotrigine, oxcarbazepine and vigabatrin. Overall, they were no more effective than placebo in reducing headache frequency.
Antidepressant medications
Amitriptyline (2.5-150mg nocte) is widely used for migraine prophylaxis. It is a first-line agent in many international headache clinics. However, the evidence in episodic migraine is relatively weak; it was found to be no more effective than placebo in one RCT. The evidence in chronic migraine is more robust.
As it may also be an appropriate medication for central pain conditions, fibromyalgia, insomnia and depression, it may be helpful in those patients where these conditions co-exist with migraine. The most common side-effects include drowsiness (often in the morning), dry mouth, constipation, weight gain and vivid dreams. If side-effects are a significant problem, a trial of nortriptyline is worthwhile.
Amitriptyline is not available in an elixir form in Ireland and the dose of the smallest tablet available is 10mg. However, the tablet can be halved or further divided.
Nortriptyline (2.5-150mg) has been found to be effective for migraine prevention by a consensus of headache experts. There are no randomised controlled trials of nortriptyline in migraine prophylaxis. It appears to have fewer anticholinergic adverse effects than amitriptyline.
Patients who experience side-effects may tolerate smaller doses of nortriptyline (or amitriptyline). Nortriptyline is not available in an elixir form in Ireland and the dose of the smallest tablet available is 10mg. Again, the tablet can be halved. It is available as an elixir in some countries.
Venlafaxine (37.5-225mg daily) is a serotonin-norepinephrine reuptake inhibitor (SNRI) that is sometimes prescribed for migraine prophylaxis. The evidence is not robust. In one RCT, it was found to be no better than placebo or amitriptyline for reducing migraine frequency, intensity and duration over two to three months of treatment.
The participants treated with venlafaxine suffered fewer side-effects than those who took amitriptyline. However, the number of people who stopped taking one or the other drug due to side-effects was approximately equal.
Selective serotonin reuptake inhibitors (SSRIs) may be used for migraine prophylaxis. However, the evidence is weak. Fluoxetine and paroxetine have been shown in RCT to be no more effective than placebo or amitriptyline in reducing migraine frequency and intensity. However, there may be clinical benefit in some patients who have comorbid anxiety, depression or other chronic pain symptoms including fibromyalgia.
Hypertensive medications
Candesartan (4-32mg daily), an angiotension 2 receptor blocker, is commonly used for hypertension and was found to be an effective migraine preventative agent in a Norwegian study in 2003. More recently, candesartan 16mg daily has been shown to be as effective as propranolol 160mg daily in migraine prevention in RCTs with somewhat different and more tolerable side-effects.
Side-effects include dry cough, respiratory tract infections, dizziness/vertigo and headache. It does not usually cause weight gain, drowsiness or mood disturbance.
Propranolol (80-160mg daily, long-acting formula) has been shown to be more effective than placebo in the prevention of migraine attacks in RCT. It is one of the most commonly used migraine agents in Ireland. Multiple studies using beta-blockers, in migraine, have been reported since 1984. The ideal beta-blocker should be cardio-selective to reduce side-effects (such as cold extremities) and hydrophilic (therefore less likely to provoke nightmares and hallucinations).
Propranolol is not cardio-selective, but it is still commonly used as many patients find it helpful. It is best taken with fluids that will help minimise a significant blood pressure drop. Taking it in the morning helps to reduce the occurrence of nightmares and hallucinations.
Metoprolol (50-100mg daily) is cardio-selective and has been shown to be as effective as propranolol in migraine prevention in evidence obtained from a non-RCT.
Atenolol (25-100mg daily) is cardio-selective and hydrophilic, but is unlicensed in Ireland for migraine.
Bisoprolol (5-10mg daily) has been used for migraine prophylaxis, but there is limited data.
Flunarizine (5-15mg daily) is a calcium channel blocker and has been shown to reduce migraine frequency more than placebo and to a similar degree as the active comparators, propranolol and topiramate in an RCT. It is often helpful in children, adolescents and those with hemiplegic migraine.
It is usually taken at night. It may cause weight gain, low mood and anxiety. It is contraindicated in people with recent or current depression, and pre-existing Parkinsonism and other extra-pyramidal disorders. It should not be used in patients with second-or third-degree atrioventricular block and left ventricular failure.
Verapamil (80-480mg daily) is another calcium channel blocking agent and is sometimes used for migraine prevention with evidence from one RCT. It is relatively safe and well tolerated. The typical side-effects include constipation, dizziness, bradycardia, nervousness or headache.
Other oral medications
Pizotifen has been used in migraine prophylaxis since 1977. It is a potent 5-HT2 antagonist with antihistaminic effects. It was not found to be as effective as propranolol in a study carried out in India. The evidence was not based on an RCT. Currently, pizotifen is licensed in Ireland, but not in the US. It is frequently used in children. Common side-effects include weight gain and sedation.
Mini-prophylaxis for pure menstrual migraine
Mini-prophylaxis has been recommended for episodic migraine predominantly associated with menstruation in the most recent NICE guidelines from 2015. Triptans are used prophylactically in those with predictable menstrual-related migraine as in pure menstrual migraine (PMM), that does not respond adequately to standard acute treatment, ie. pain freedom at two hours post-ingestion of acute therapy.
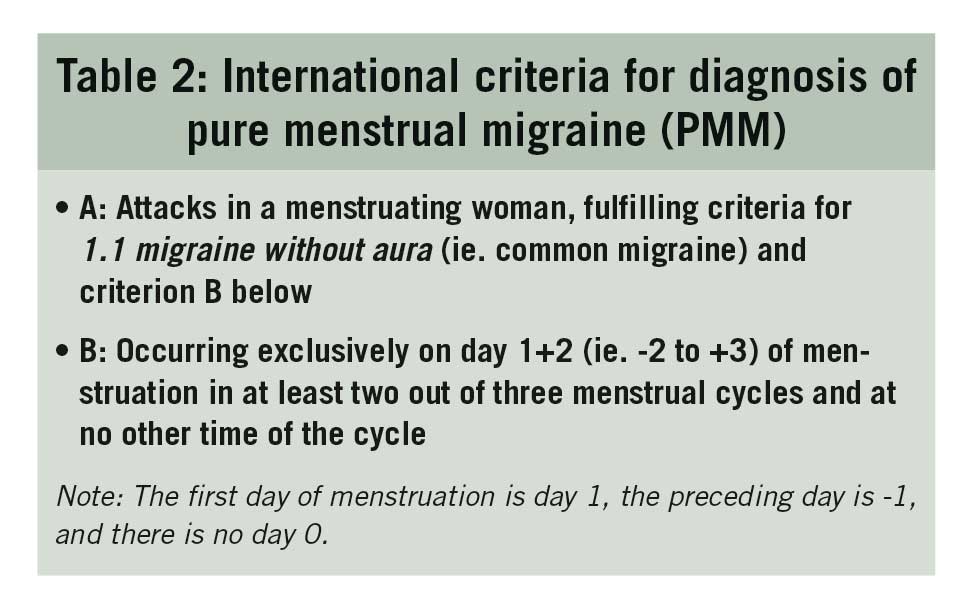
Pure menstrual migraine (PMM) is present in 7-14% of migraneurs and its occurrence is wholly confined to a strict period around menstruation, and very rarely at other times. It is important that diary-documented evidence, over a minimum of three cycles, is present to confirm the diagnosis of PMM (see Table 2).
(click to enlarge)
PMP attacks are usually of longer duration and are more severe than migraine at other times in the cycle. In general, treatment is the same for menstrual migraine as non-menstrual migraine. If migraine is infrequent, NSAIDs alone (or with paracetamol) or in combination with a triptan, may be particularly helpful. NSAIDs are also beneficial for treating menstrual cramps.
If migraine is frequent, predictable, prolonged or poorly responsive to therapy, consideration should be given to what is known as mini-prophylactic treatment. In this situation, the long-acting triptans, frovatriptan or naratriptan 2.5mg twice a day, are recommended for continuous use over three to five days. This should not significantly contribute to medication overuse as long as these latter agents are limited to no more than six to eight days per month. The triptan may be started in combination with an NSAID two days before the expected date of menstruation (in patients with regular cycles) or during the prodrome.
The predictability of PMM makes these headaches more amenable to planned treatment. The importance of distinguishing between PMM and menstrual-related migraine (MRM) is that hormone prophylaxis is more likely to be effective for the former.
Mini prophylaxis for menstrual-related migraine
Menstrual-related migraine (MRM) occurs in two-thirds of female patients. This is where attacks occur during menstruation two-thirds of the time and the rest at other times.
Menstruation is considered to be endometrial bleeding resulting from either:
Normal menstrual cycle
Withdrawal of exogenous progesterone when using the combined oral contraceptive pill
Withdrawal of cyclical hormone replacement therapy.
MRM with aura, in the age group 15-49 years, usually has a different hormonal response than those who get PMM or MRM without aura. MRM with aura is most often seen in high oestrogen states such as combined hormonal contraception or hormonal replacement therapy.
It has been suggested that one could increase the dose of their regular preventative medication, such as topiramate or amitriptyline, five days before menstruation but the evidence for this is mostly anecdotal. Adding magnesium 500mg starting at ovulation and continuing until after menstruation may prevent or decrease the severity of migraine attacks but again the evidence basis for this approach is poor and mostly anecdotal.
For those with PMM and MRM, a possible approach is to suppress ovulation using the following:
Progesterone-only pill (POP) desogestrel, as other POPs act primarily through their effects on cervical mucosa and are unlikely to suppress ovulation. The POP is safe in those with migraine with aura.
Progesterone injection ie. Depo-provera given 12-weekly
Progesterone implant ie. Implanon, which lasts three years.
The Mirena coil also contains progesterone. It acts at a local level on cervical mucosa and results in thinning of the uterus. It usually does not supress ovulation, so it may not prevent PMM or MRM for some women.
A further approach is to supplement oestrogen during the days when oestrogen levels drop significantly with an oestrogen-containing gel. It is possible to partly or completely supress the menstrual cycle by using the combined oral contraceptive pill (COCP) without a break for 63-84 days (three or four 21-day packs without a break). It is acceptable to continue this 63-84 day cycle for a number of years. Women need to be mindful of weight gain when taking hormonal contraception as it is a risk factor for headaches.
Other preventative strategies
Physiotherapy
Physiotherapy may be helpful for those migraine patients with significant vestibular features and/or neck pain. Disequilibrium or vertigo symptoms are often experienced by migraine sufferers. Manual mobilisation therapy and trigger point treatments of the cervical spine and scalp may be helpful.
Acupuncture
Acupuncture had been shown in a Cochrane review to help some patients with migraine with evidence coming from an RCT. The available trials suggest that acupuncture may be at least as effective as prophylactic treatment with oral sodium valproate or metoprolol.
GON nerve blocks
Greater occipital nerve (GON) blocks are sometimes used to treat chronic migraine sufferers. Many patients will improve significantly for a number of months after a single GON block. Other patients may require a number of GON blocks for sustained improvement.
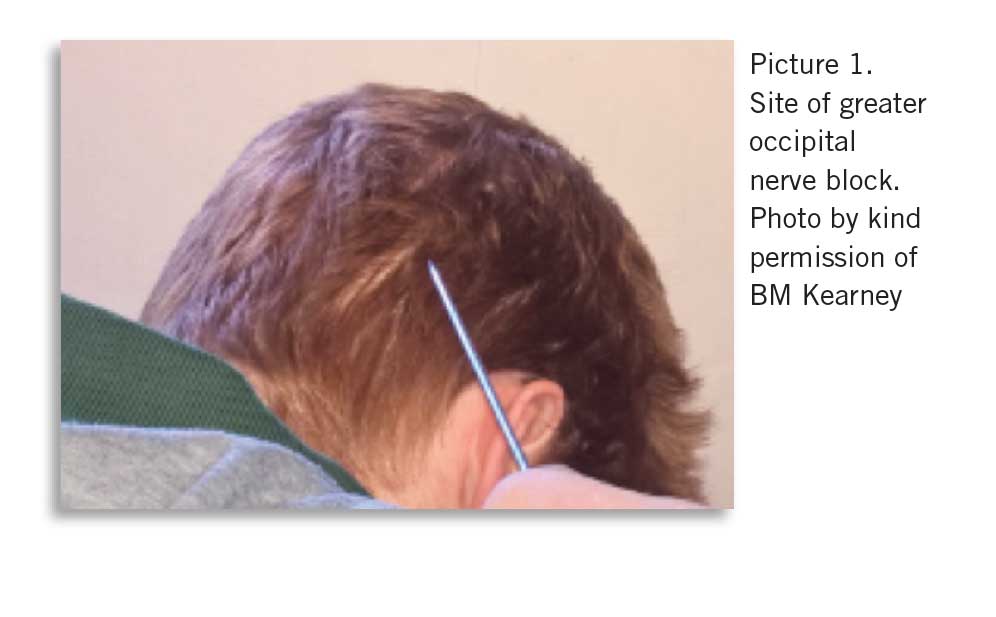
In Ireland, a combination of steroids and lidocaine is injected into the greater occipital nerve (see Picture 1). In the US and increasingly commonly in Europe, they are performed with lidocaine and saline.
(click to enlarge)
GON blocks using steroids should not be performed more frequently than every four to six months on each side due to the risk of local tissue damage. In a recent RCT, a GON block with steroid and lidocaine or normal saline with lidocaine were equally effective up to two months after intervention.
There is a limit as to the total number of GON blocks using steroids that one can undertake in an individual patient, due to the risk of systemic side-effects. GON blocks have been shown to reduce pain severity and frequency as well as the use of analgesia up to two months after intervention.
The greater occipital nerve can be found superficially, approximately 2.5-5cm infero-lateral to the occipital prominence. The patient is positioned sitting with the head either vertical or slightly flexed. The nerve is located and felt along the superior nuchal line. Depo-mederone 40mg/ml is used. The 2ml amp is diluted with 3ml sterile water and injected into the tender GON.
Some GPs undertake this procedure in their surgeries, but to date, no research on its usage in general practice has been undertaken. This therapeutic procedure gives short-term relief of two to three months. Rare side-effects (less than 1%) include lipoatrophy at the injection site with loss of hair growth.
GON blocks may improve the headaches and associated symptoms in the short- to medium-term.
Botox
Botulinum neurotoxin (BoNT) or ‘Botox’ is a protein complex produced by the anaerobic bacterium Clostridium botulinum. Two types are currently in clinical use: Botox type A and Botox type B.
Botox type A was shown to be effective in prophylaxis of chronic migraine in an international, multi-centre, double blind, randomised, placebo-controlled trial in 2010; the Phase 111 Research Evaluating Migraine Prophylaxis Therapy (PREEMPT) trial.
In Ireland, access to Botox is very limited via the public hospital system and private health insurers do not usually reimburse patients for this treatment. In the UK, the National Institute for Health and Care Excellence (NICE) recommends its use in patients with chronic migraine who have not responded to at least three prior pharmacological prophylactic therapies and whose condition is appropriately managed for medication overuse.
Neuromodulation
Neuromodulation is a novel treatment approach for patients with episodic and chronic migraine. There are several different devices available and the evidence for their use is variable. However, some patients respond very well and there are usually limited side-effects. The exact mechanism of action is unclear for many of these treatments.
The most simple and non-invasive devices are handheld. They are used daily by the patient for short periods (typically less than an hour each day).
More invasive neuromodulation approaches include hypothalamic deep brain stimulation, occipital nerve stimulation, sphenopalatine ganglion and cervical spinal cord stimulation. These are very specialised clinic treatments – usually overseas – and they should only be considered for the most refractory patients.
Alternative migraine therapies including biofeedback, mindfulness, reflexology, and TENS machines, may be helpful for some migraine patients.
Reviewing the patient with chronic migraine
A six-month review is adequate for those with well-controlled migraine. If the person has more than 10 headache days per month, a three-month review should be undertaken using the proforma in Table 1.
If a person has persistent symptoms of migraine disorder despite maximum tolerated prophylactic treatment for two to three months, one should consider a change in prophylactic medication. It is always important to remind patients that a regular lifestyle will help their migraine remain well controlled and may even improve their symptoms.
The future for migraine management
There is a clear clinical need for specific acute and preventative migraine treatments. The most promising new preventative treatments are the calcitonin gene-related peptide (CGRP) monoclonal antibodies, which have been developed after significant research initiated in 1985 in Sweden. It is known that CGRP levels are raised in migraine patients, and it is believed that the CGRP system plays a fundamental role in the migraine attack. CGRP is one of the most potent naturally occurring vasodilators.
Four different CGRP agents have been developed. These agents bind to either the CGRP receptor or the ligand. The first three agents; erenumab, fremanezumab and galcanezumab are licensed in the US and Europe.
These new anti-CGRP treatments are mainly for prophylaxis and are delivered by IM or IV injection once every 4-12 weeks. They appear to block the CGRP pathway and results in clinical trials are very promising. The future for those with migraine is brighter now than ever.
This module is based on the 2019 ICGP Quick Reference document on ‘Migraine – diagnosis and management from a GP perspective’ which is available on the ICGP website www.icgp.ie, click ‘Quick Reference Guide’ under the Library headline
 (click to enlarge)
(click to enlarge)