The multidisciplinary MS team must help and encourage patients to manage their condition effectively
Ms Sinead Jordan, Clinical Nurse Specialist in MS, St Vincent's University Hospital, Dublin, Dr Cristopher McGuigan, Consultant Neurologist, St Vincent's University Hospital, Dublin and Dr Michael Hutchinson, Consultant Neurologist, St Vincent's University Hospital, Dublin
Multiple sclerosis (MS) is the most common cause of non-traumatic neurological disability in young adults. It is an inflammatory disease of the central nervous system, characterised by T-cell and B-cell mediated demyelination and neurodegeneration. It is typically diagnosed in people between 20 to 45 years of age and follows an unpredictable course. The prognosis can vary considerably from one person to the next.
MS typically presents with a history of acute onset of neurological symptoms or with progressive neurological impairment. The disease involves an initial relapsing-remitting course (RRMS) in 80-90% of patients, although relapses are not always followed by complete recovery. The majority of RRMS patients develop, within 10-20 years, secondary progressive MS, characterised by irreversible and relentless accumulation of disability leading not only to personal and caregiver burden but also to high societal and economic costs.
MS affects 1.1 to 2.5 million people worldwide. Environmental and genetic factors contribute to its aetiology and genetic factors contribute to MS susceptibility.
Areas with high MS prevalence include North America, Northern Europe and Australasia with a prevalence of 1:1,000 adults. Ireland has reported prevalence rates of 120-180-240 per 100,000.1,2 MS affects women more than men, at a ratio of 2:1, and is diagnosed in Caucasians more often than in any other racial/ethnic group.3
Clinical courses of MS
Four clinical courses have been described:
• Clinically isolated syndrome is the first neurological episode experienced by a patient that is caused by inflammation or demyelination in the CNS. According to the MS Trust,4 85% of MS patients will experience an initial symptom lasting for at least 24 hours. Typical symptoms include optic neuritis, diplopia and numbness
• Relapsing-remitting multiple sclerosis (RRMS): Approximately 85% of patients who are diagnosed with MS present with RRMS. A relapse is an acute episode of neurological symptoms that gets worse over a few days and improves or subsides over time. A period of 30 days should separate the onset of two relapse events for them to be distinguished as two attacks5
• Primary progressive multiple sclerosis is characterised by progression of disability from the onset (usually as a progressive spastic paraparesis) without remissions or with occasional plateaus and temporary minor improvements
• Secondary progressive multiple sclerosis (SPMS) begins with an initial RRMS course, followed by remission of variable rate that may also include occasional relapses and minor remissions. The transition from RRMS to SPMS is often gradual and sometimes only detectable in retrospect.
Diagnosis
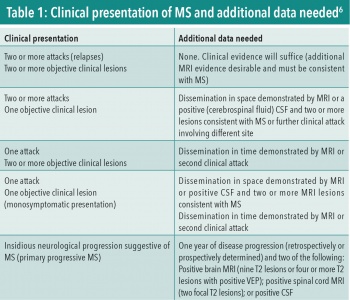
The McDonald revised criteria 2010 are generally regarded as the gold standard for the diagnosis of MS. There is no single diagnostic test for MS. The diagnosis is reliant on the patient’s history and examination, the interpretation of an MRI, the presence of CSF oligoclonal bands, visual evoked potentials and neuroinflammatory bloods (ANA, ENA, ACE, Lyme serology, NMO). It is necessary to exclude other central nervous system disorders and MS-mimics such as Lyme disease (an infectious disease), neuromyelitis optica or acute disseminated encephalomyelitis.
The McDonald revised criteria 2010 have been developed and refined over the past 20 years (a recent revision is presently underway). While it is possible to diagnose MS by clinical criteria alone, all patients should have an MRI scan of the brain and spinal cord to confirm the characteristic features and to exclude MS mimics such as an Arnold-Chiari malformation. Table 1 outlines the clinical presentation and the requirement for additional data.
(click to enlarge)
An attack or relapse is defined as the recurrence of previous symptoms or the manifestation of new symptoms lasting for at least 48 hours.
Acute relapses are usually treated with a three-day course of intravenous methylprednisolone 1g daily. Steroids have been shown to reduce the time taken to recover from a relapse. Oral steroids can also be prescribed on a reducing dose over three weeks.
Symptoms and signs of MS
MS lesions plaques are found in the brain and spinal cord. Most plaques are asymptomatic. The myelin sheath that facilitates the conduction of impulses along the nerve axons becomes damaged by the autoimmune process and this causes the impulses to be delayed or completely blocked. This in turn can result in any of the numerous symptoms reported by people with MS. The symptoms are determined by where the MS lesion is located within the CNS.
Specific signs and symptoms are taken as confirmation of lesions in certain functional systems of the CNS – the following are examples of the symptoms that the patient may present with or report:
• Optic nerves : sub-acute onset of unilateral visual blurring with reduced acuity often associated with pain
• Oculomotor/brainstem: double vision, nystagmus
• Spinal cord: limb weakness and/or numbness, spasticity, sexual dysfunction, bowel and bladder dysfunction
• Cerebral: mood issues/depression, cognitive impairment and fatigue
• Sensory: numbness and pain.
Symptomatic therapy
The treatments available for MS include managing symptoms with both symptom specific medications (anticholinergics for urinary urgency). Non-drug treatments include physiotherapy, occupational therapy and speech and language therapy.
Disease-modifying therapies
Perhaps the most important development in managing patients with MS was the development of consensus guidelines recommending regular, at least yearly clinical assessments, and annual MRI assessments in patients with relapsing MS.7 These criteria emphasised the importance of classifying patients (by both clinical and MRI measures) as to having ‘not active’ or ‘active’ disease and assessing whether there was, or was not, evidence of increased neurological disability.
Disease-modifying therapies are not a cure for MS but they can reduce how many relapses someone has and how serious they are. They have been shown to reduce the risk of progressive disability. The goal of treatment should be to slow the irreparable damage to the axons and therefore delay progression of the disease to irreversible SPMS.
There has been a remarkable development in the number of disease-modifying therapies available for patients with relapsing MS in the past 20 years. Unfortunately, convincing evidence for an effect of these drugs in SPMS is not available. We are now at the stage where, with active management involving regular review, annual MRI scans and escalation of therapy, we can contemplate controlling disease activity in patients with RRMS with the aim of preventing the development of SPMS.
Given the increasing complexity of disease management in MS, patients are best managed by neurologists with a special interest in this disease. All patients with RRMS should be seen at least annually with review immediately after an annual MRI scan (even if their disease appears to be stable to them and their neurologist).
There are several factors for the clinician and patient to consider when choosing a disease-modifying therapy that best suits the patient’s needs.
Firstly, consider the patient and their disease profile, age, gender, comorbidities, the level of disease activity – clinically and/or MRI – treatment history and biomarkers, ie. JCV-antibody status.
Secondly, the patient’s preferences must be considered and can be determined by their lifestyle. Is the patient working? Does the patient have a busy life, young children, can this affect adherence?
The risk/benefit of the treatment to the patient must also be considered including tolerability, side-effects and the impact this may have. Frequency of treatment and mode of administration, safety and the safety monitoring that is required which may include frequent blood samples and MRI scans.
The availability and access to some disease-modifying treatments can be limited. Often, health providers have a restricted financial budget for such therapies and therefore it can be extremely difficult to get access to them.
First-line therapies are available in Ireland for people diagnosed with CIS and RRMS. They are usually well tolerated, have a good safety profile, reduce relapse by approximately one-third and may often be the only treatment necessary for many people with MS.
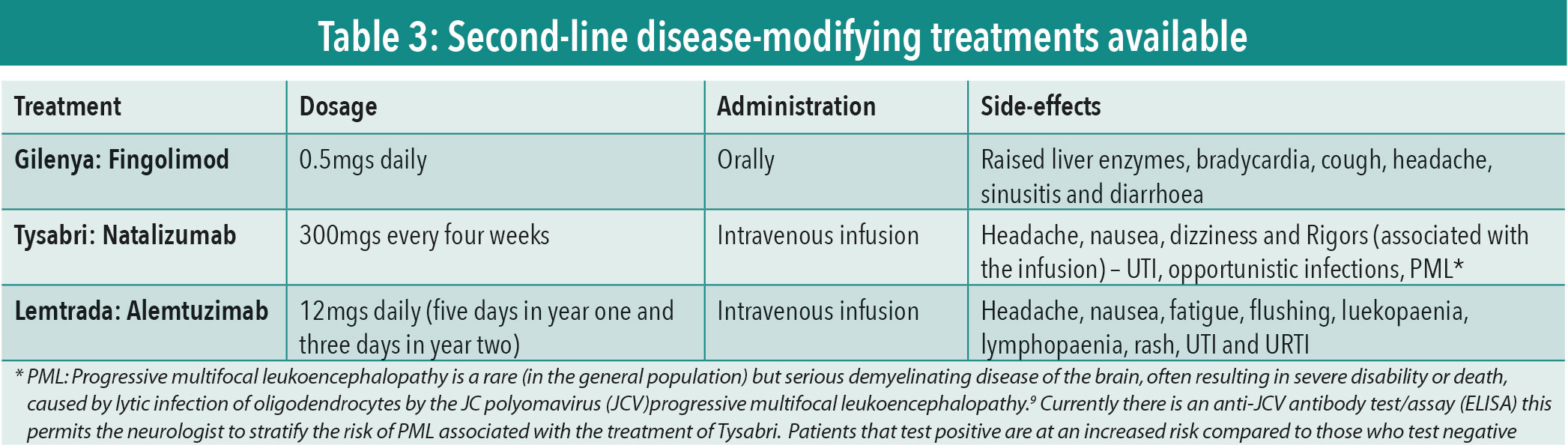
Second-line therapies are treatments that are licensed for use in Ireland in patients with RRMS. If they have failed a first-line treatment (their disease has continued to progress while on treatment), this can be determined by MRI changes, new symptoms or increase in previous symptoms and the expanded disability scale score (EDSS).
The EDSS is a standardised assessment tool that was developed by Kurtzke in 1983,8 it is used by neurologists to measure disability caused by MS in eight functional systems; pyramidal, cerebellar, brainstem, sensory, bladder and bowel, visual, cerebral and other. This score allows the neurologist to determine if the patient’s MS has progressed.
Second-line therapies are indicated when a patient reports new symptoms, disease is actively progressing (by clinical or MRI criteria) and treatment needs to be escalated to a more effective treatment. The decision for accelerating treatment is that of the neurologist and the patient.
Table 2 outlines the second-line disease-modifying treatments currently available, the dosage, the method of administration and very common side-effects.
(click to enlarge)
Monitoring
Everyone treated with a disease-modifying treatment, regardless if it is first or second-line, should adhere to a strict monitoring regime. This may vary from centre to centre but generally involves regular blood tests to monitor LFTS and urine tests. Some therapies require the patients to have regular MRI scans performed. These are in place to ensure the safety of the patient.
Breaking bad news
It is never an easy task when you are required to confirm a diagnosis that will certainly cause the patient distress. There are however certain things that should be considered at such times. Bad news ideally should always be given in person, it may help if you ask the patient to bring a relative with them for the consultation as it forewarns a patient that a serious conversation is about to take place.
It is essential that you use language that the patient will understand and have in-depth knowledge of the clinical course the patient has been diagnosed with. It helps to establish what the patient already knows about MS and allow time for the patient to confirm they understand what you are talking about and to ask questions if they wish.
At this initial consultation, it is important to try and gauge how much information the person would like to know as it will vary significantly from one person to the next. Stay mindful of how the patient is coping with the information.
Finally, a plan should be put in place, including a follow-up appointment with the consultant neurologist or the MS nurse specialist. Written information should be provided including contact details of the MS Ireland.
MS management and support networks
People living with MS will acquire coping strategies to deal with their diagnosis. How useful these strategies are will depend on the patient’s outlook, their personality and the support network they have in place.
The multi-disciplinary team (MS nurse, neurologist and GP) should try to help and encourage the patient to manage their disease effectively, allowing them to live their life as normally as possible.
There are very useful supports available to people with MS in the community.
Patients on disease-modifying treatments may have access to homecare nurses who are specially trained in the administration of specific treatments. They have a huge knowledge base with regards to the expected side-effects and management of these.
MS Ireland is another excellent resource for patients and their families. It is a national organisation that provides information, support and advocacy services to the entire MS community. It provides a wide range of MS programmes (including physiotherapy, symptom management and information forums). MS Ireland runs workshops and activities throughout the country that are aimed at different groups such as newly diagnosed people, carers, children of parents with MS and health professionals.
The positive factor for people diagnosed with MS at the moment is that there are so many treatments available to them compared to 20 years ago. The volume of research being done for MS is huge, research shows that early treatment with a disease-modifying treatment is essential. There are many exciting therapies currently in clinical trials that hopefully will be available in the next few years.
(click to enlarge)
References
McGuigan C, McCarthy A, Quigley C et al. Latitudinal Variation in the prevalence of Multiple Sclerosis in Ireland, an effect of genetic diversity. J Neurol Neurosurg Psychiatry 2004, 75: 572-576
Lonergan R, Kinsella K, Fitzpatrick P et al. Multiple Sclerosis prevalence in Ireland: relationship to vitamin D status and HLA genotype. J Neurol Neurosurg Psychiatry 2011, 82(3): 317-322
Richman S & Schrub E. Multiple Sclerosis. Cinahl Information Systems; Ipswich 2011
MS Trust. Multiple Sclerosis Information for Health and Social Care professionals, 4th ed. Hertfordshire 2011
McDonald WI, Compston A, Ebers G et al Recommended diagnostic criteria for Multiple Sclerosis: Guidelines for the international panel on the diagnosis of Multiple Sclerosis. Annals of Neurol.2001, 50: 121-127
Polman CH, Reingold SC, Banwell B et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Annals of Neurol. 2011, 69(2):292-302
Lublin FD, Reingold SC, Cohen JA et al. Defining the clinical course of Multiple Sclerosis: the 2013 revisions. Neurology 2014, 15; 83(3):278-86
Kurtzke, JF. Rating Neurologic Impairment in Multiple Sclerosis: An Expanded Disability Status Scale (EDSS). Neurology 1983, 33: 1444-1452
Brew BJ, Davies NW, Cinque P et al. Progressive multifocal leukoencephalopathy and other forms of JC virus disease. Nature Reviews, Neurology 2010, 6: 667-679
 (click to enlarge)
(click to enlarge)