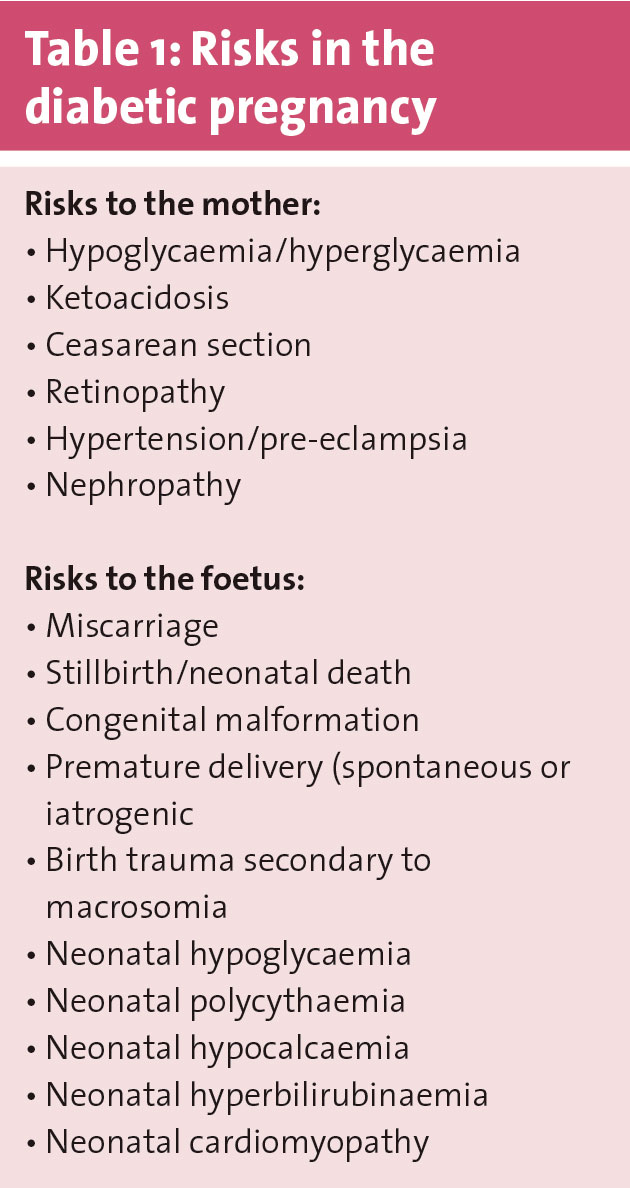
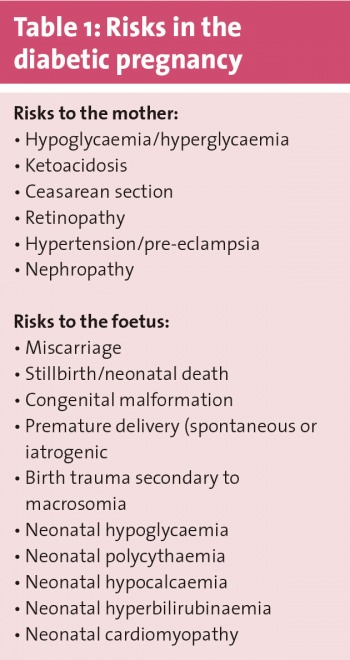
The risks of maternal and foetal complications in pregnant women with diabetes (type 1, type 2 and gestational) are significant. Complications include miscarriages, hypertension and pre-eclampsia in the mother and congenital malformations, neural tube defects and macrosomia in the baby, to name but a few. Linda Matthews, a diabetes nurse specialist, presented on the importance of pre-pregnancy care at the multidisciplinary diabetes study day earlier this year.
(click to enlarge)
“Everyone aspires to have a healthy baby and to be healthy during their pregnancy so that they can enjoy it,” she said.
“But when it comes to planning a pregnancy, some women take a day to plan, some a month and some a year,” she added.
For women with diabetes, planning the pregnancy needs to start early. Diabetes is the most common medical disorder of pregnancy and complicates four out of 1,000 pregnancies, with a 3.5-fold increased perinatal mortality rate and a stillbirth rate five times higher than in a non-diabetic pregnancy.1
But with over half of all pregnancies being unplanned, how does one even begin to tackle this obstacle?
Access to care
Ms Matthews stressed that when it comes to pre-pregnancy care and pregnancy planning, all women with type 1 and type 2 diabetes, women with a possible previous history of gestational diabetes and women with pre-diabetes need to be targeted.
“We need to ask ourselves where these women receive their care or whether they have any access point at all to pre-pregnancy care. Some of these women may not even attend their GP, they could be well and then discover that they are pregnant and that they have diabetes. We need to ask what services these women need and whether they have access,” said Ms Matthews.
“We need to raise awareness of pre-pregnancy care and planning in clinics,” she added.
Ms Matthews’ sentiment is echoed both in Irish clinical practice guidelines as well as NICE guidelines,1,2,3 where the importance of pre-pregnancy counselling for women with diabetes is stressed.
“Pre-pregnancy counselling should be part of all structured education and involves checking pregnancy intention, checking on contraceptives and educating women on the importance to plan a pregnancy,” explained Ms Matthews.
Pre-pregnancy care
Ms Matthews pointed out that pre-pregnancy care is by no means a new phenomenon, so why then are outcomes in diabetic pregnancies still so poor?
The Atlantic DIP1 and CEMACH4 studies have shown that women with diabetes run twice the risk of congenital malformations, have a 3.5-fold risk of increased perinatal mortality, six-10-fold increase in macrosomia, five-fold increase in stillbirth and a four-fold increase in neural tube defects.
“Diabetes in pregnancy is one of the key things we have to look at, and try to do better,” commented Ms Matthews.
In order to start this improvement, women of childbearing age who have diabetes (or previous gestational diabetes) need to be informed about the huge importance of pre-pregnancy care.
With 50% of all pregnancies unplanned, it is high time to tackle the information gap for women with diabetes.
The Atlantic-DIP practice guidelines state that the need for preconceptual counselling should be emphasised at every annual diabetes review with women of childbearing age.
If appropriate, advice on preconceptual care and contact details for pre pregnancy planning clinics should also be given at interim visits, whether community or hospital-based.1
Planning a pregnancy
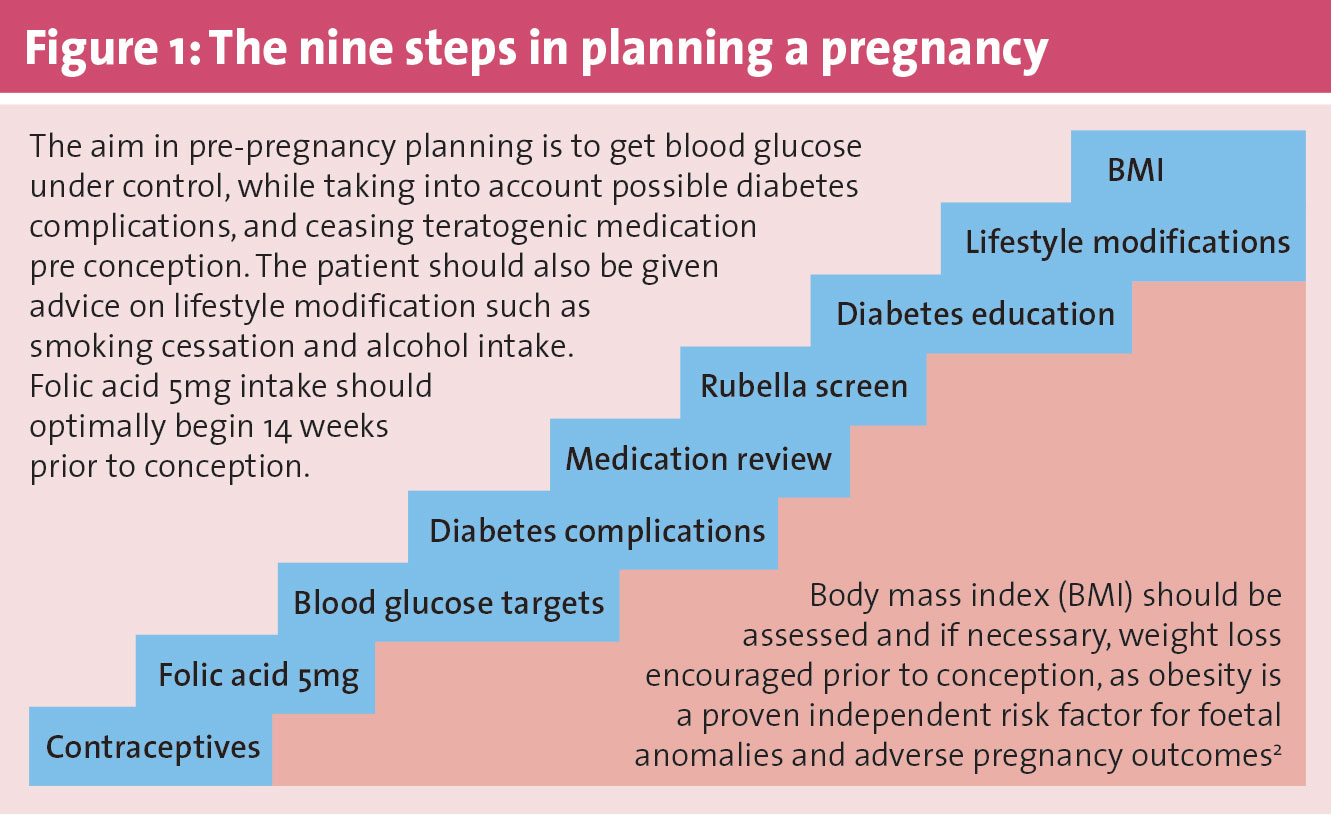
“There are nine months in a pregnancy and nine steps to planning a pregnancy,” said Ms Matthews.
The nine steps she referred to are illustrated in Figure 1 and elaborated on below.
(click to enlarge)
Contraceptives
There is a wide range of contraceptives available and Ms Matthews advised that women should visit their GP to discuss which one may suit them best.
“It is important that all women with diabetes are still on contraceptives when they are coming to a pre-pregnancy planning clinic. Women who have diabetes should either be planning a pregnancy or avoiding a pregnancy, there should be no in-between,” she said.
According to Atlantic-DIP guidelines, preparation for a pregnancy should start as early as six to three months pre conception.1
Folic acid
“Women with pre-gestational diabetes should be on high-dose folic acid (5mg), which needs to be prescribed by a doctor, and it needs to be taken 14 weeks prior to pregnancy and up through the first trimester,” said Ms Matthews.
According to Egan et al,5 there is no evidence of a clinical benefit of this higher folic acid dose compared to the normal recommendation of 400µg for pregnant women, however, several advisory groups have made this recommendation based on a theoretical benefit in reducing the increased risk of nerual tube defects associated with diabetes during pregnancy.
Blood glucose targets
According to Ms Matthews, blood glucose targets in pre-pregnancy should be reflected in pregnancy, this is the only way to really prevent harm to the foetus during the critical early stage of pregnancy (six to ten weeks) when important organs are developing (organogenesis).
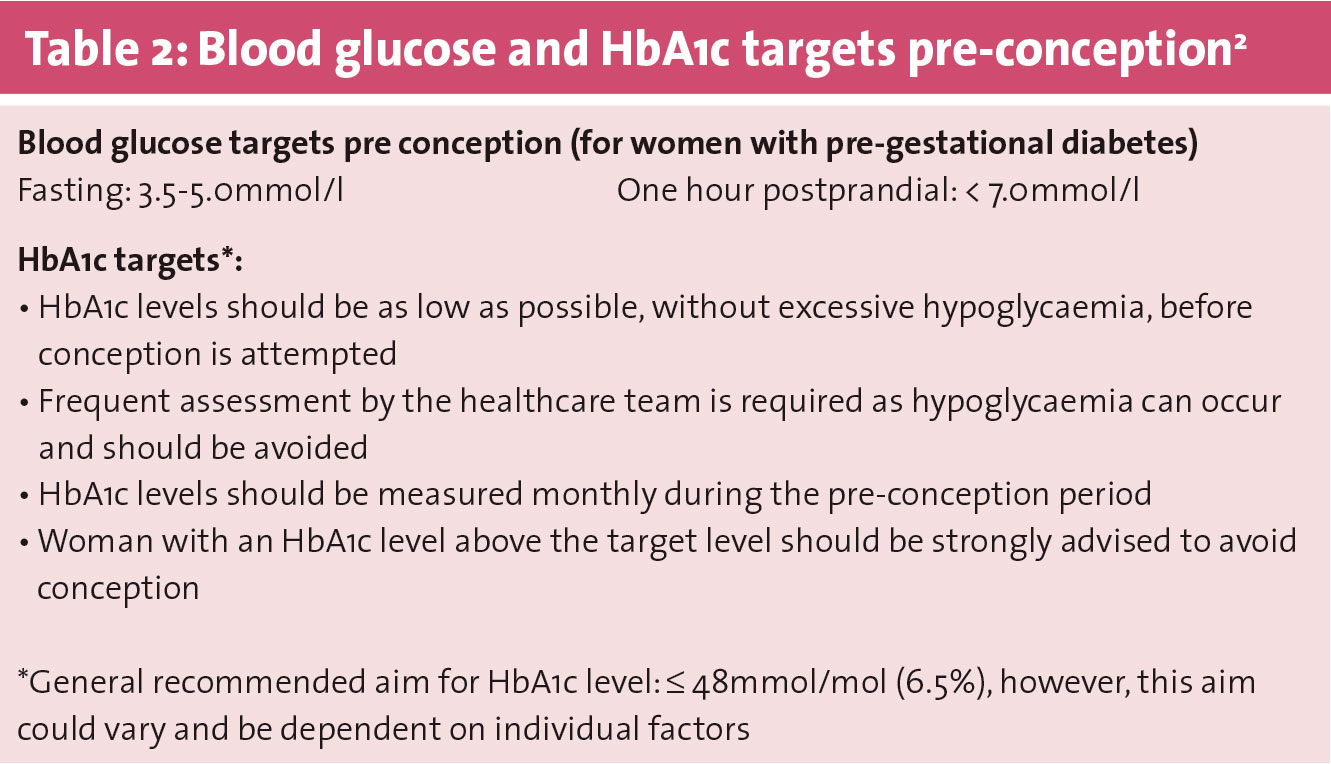
“In practice this means a blood glucose level of less than 5mmol fasting and pre meals, and less than 7mmol postprandial,” explained Ms Matthews.
Regarding HbA1c levels, HSE guidelines only says “as low as possible without excessive hypoglycaemia”,2 and other recommendations, according to Ms Matthews, go up to 53mmol/mol depending on age and other factors.
“So anything between 42-53mmol/mol is ok,” said Ms Matthews.
See Table 2 for blood glucose and HbA1c targets in the pre-conception period.
(click to enlarge)
Diabetes complications
For women without retinopathy pre-pregnancy, a fundal examination is advised prior to conception and once in each trimester thereafter.1 For those with established retinopathy pre-pregnancy, retinal examination is advised every six weeks as rapid tightening of blood glucose control can cause retinopathy to deteriorate. Vigilance is necessary.1
“Retinal and renal complications need to be screened for at the pre-pregnancy stage. If a woman comes into the pre-pregnancy clinic and hasn’t had a retinal screen in three or four years, you should see if you can fast-track her in for retinal screening. You can’t really optimise her glycaemic control until you know what the retinal situation is,” said Ms Matthews.
According to Atlantic-DIP, worsening nephropathy and superimposed pre-eclampsia are the most common causes of pre-term delivery in women with diabetes.1 Pre-existing nephropathy is also linked to poorer pregnancy outcomes, and as there is a chance of irreversible further decline in renal function as a consequence of pregnancy, women need to be advised about this.1
“In relation to renal complications, check ACR (albumin:creatinine ratio) and serum creatinine. The patient should be referred to nephrology if ACR is greater than 30[mg/mmol] and serum creatinine greater than 120[µmol/l], to seek advice,” explained Ms Matthews.
Women with established nephropathy should be referred to and managed by nephorologists, according to HSE guidelines.2
Medication review
It is vital that medications with known teratogenic effects are substituted with medications appropriate to pregnancy prior to conception.2
“The only oral hypoglycaemic agent that can be used is metformin, otherwise the patient should be switched to an insulin,” said Ms Matthews.
Blood pressure needs to be measured at an initial physical examination, and if hypertension is present, then anti-hypertensive medication suitable in pregnancy prescribed.2
“ARBs and ACE inhibitors in relation to hypertension need to be stopped pre pregnancy as do statins, as they are all teratogenic.”
Lipid-lowering agents also need to be stopped and labetalol or methyldopa can be used instead of ARBs and ACE inhibitors, explained Ms Matthews.
“In relation to someone who is on an ACE inhibitor due to renal disease, the advice would be to leave them on their ACE until their HbA1c is under control and then switch them on to other agents [eg. calcium channel blocker] pre conception.”
Rubella screen
“We do a rubella screen, because primary rubella infection can be disastrous. We advise women to vaccinate three months before trying to conceive,” said Ms Matthews.
Diabetes education
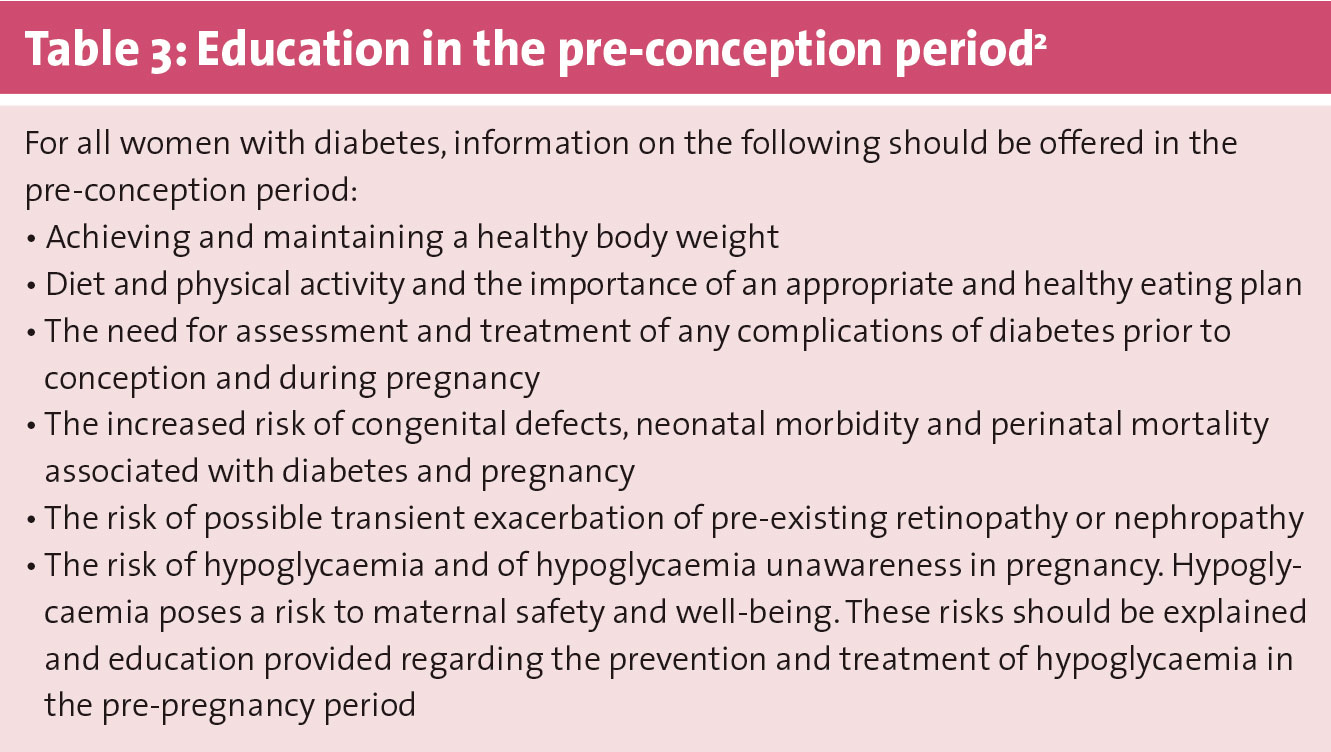
Educating women with diabetes about the possible complications of pregnancy and how best to avoid them is essential. See Table 3 for a list of recommendations on education in the pre-conception period.
(click to enlarge)
“Explain that pregnancy is associated with hypoglycaemia and why medications that they are on are teratogenic, etc,” said Ms Matthews.
“Hypoglycaemia may be important to go through, especially if a woman has been on antihypertensives at this stage, and it would be important that they correct it accurately.”
Lifestyle modification
“Smoking and alcohol consumption should be stopped, as in normal pregnancies,” said Ms Matthews.
“Diet should also be looked at for optimising glucose control.”
In some cases, women may also need referral for alcohol or drugs counselling,1 and appropriate physical activity should be advocated as it has beneficial effects on insulin resistance.2
However, for women on insulin therapy, the management of hypoglycaemic events resulting from physical activity should be discussed.2
BMI
A high BMI is an independent risk factor for pregnancy-induced hypertension and gestational diabetes. The higher the woman’s BMI, the higher the risks, explained Ms Matthews.
In general, she would recommend that all women planning on getting pregnant stay below a BMI of 30kg/m2, as a BMI over this value means that a woman runs a three times higher risk to end up with gestational diabetes.
“The best way to protect the woman’s health and the baby’s health is to lose weight before becoming pregnant.”
NICE guidelines recommend that women with diabetes and a BMI over 27kg/m2 pre-conception be offered advice on how to lose weight in line with its guidelines on obesity.3
Hopes for the future
Ms Matthews ended her presentation with a reminder that in order to prevent unplanned pregnancies in women with diabetes, and thereby avoid complications associated with same, healthcare professionals involved in diabetes care need to discuss with women of childbearing age about the importance of contraception and pre-pregnancy counselling and care at every opportunity.
She has recently developed a PPC steering group with her diabetes colleagues as a subgroup of IDNSA (Irish Diabetes Nurse Specialist Association). It is hoped that this steering group will raise awareness and promote PPC for both primary and secondary care settings in Ireland.
“Check pregnancy intention, check on contraceptives and educate them about the importance of planning a pregnancy,” she concluded.
References
Dunne f, Gaffney G. Guidelines for the management of diabetes in pregnancy. 3rd edition, August 2015. As accessed on http://atlanticdipireland.com/wp-content/uploads/2016/01/Guidelines-Atlantic-DIP-Clinical-guidelines-for-the-management-of-diabetes-in-pregnancy.pdf
HSE. Guidelines for the Management of Pre-gestational and Gestational Diabetes Mellitus from Pre-conception to the Postnatal period, as accessed on https://www.hse.ie/eng/about/Who/clinical/natclinprog/obsandgynaeprogramme/guide11.pdf
Nice guidelines 2015 – Diabetes in pregnancy: management from preconception to the postnatal period. As accessed on https://www.nice.org.uk/guidance/ng3?unlid=381907842016220155824
CEMACH, Confidential Enquiry into Maternal and Child Health. Pregnancy in women with type 1 and type 2 diabetes in 2002-2003, as accessed on http://www.bathdiabetes.org/resources/254.pdf
Egan AM, Murphy HR, Dunne FP. The management of type 1 and type 2 diabetes in pregnancy. QJM: An international Journal of medicine 2015: 923-927. doi: 10.1093/qjmed/hcv060
 (click to enlarge)
(click to enlarge)