An overview of the therapies used in advanced breast cancer
Dr Megan Greally, Oncology Specialist Registrar, St Vincent's University Hospital, Dublin and Dr Janice Walshe, Consultant Medical Oncologist, St Vincent's University Hospital, Dublin
Advanced breast cancer (ABC) is a heterogeneous disease that includes several biological subtypes with varying treatment approaches and outcomes. Although meaningful improvements in survival have been achieved, ABC is still considered an incurable condition. Median survival now exceeds two years but outcomes range from months to several years with some prospect of durable remission in certain patient populations.1 The objectives of therapy continue to be prolonged survival but this must be achieved at an acceptable quality of life. To achieve this, treatment strategies in ABC are increasingly underpinned by a focus on developing biomarkers to tailor therapies appropriately.
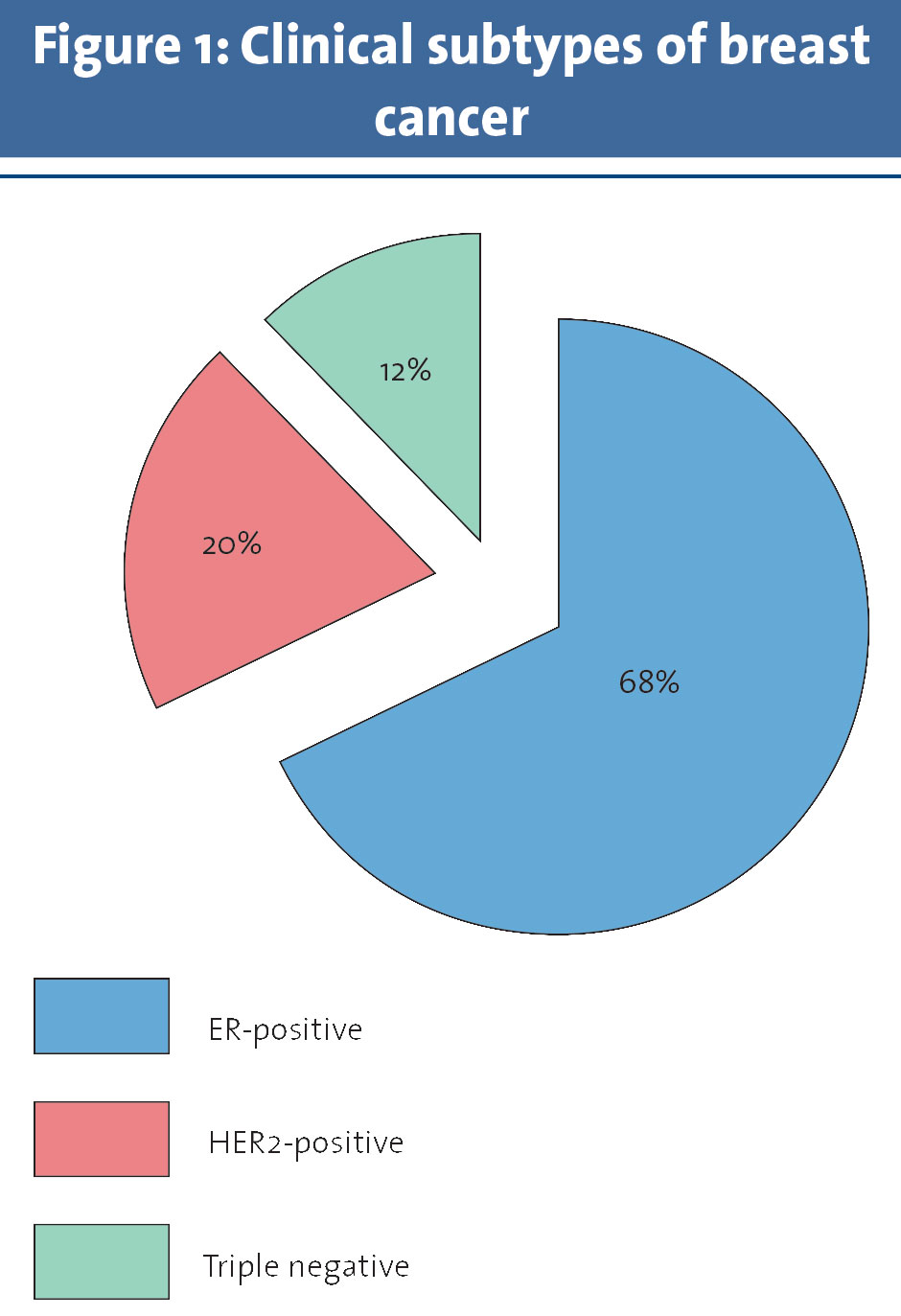
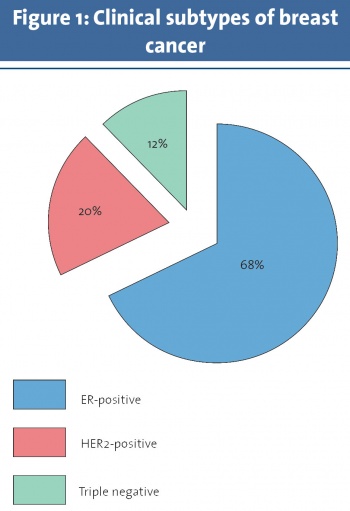
The medical approach of patients with ABC can be stratified according to whether a tumour is oestrogen receptor (ER) positive or negative, and HER2-positive or negative. Through bench to bedside translational research, the field has seen many advances, particularly in new agents aimed at overcoming endocrine resistance and promising targeted therapies, particularly in the HER2-positive and luminal-like (hormone sensitive) subtypes. Despite many improvements, progress in the more rare basal-like subgroup, also referred to as ‘triple negative’ breast cancer, has been slow. The lack of a reproducible ‘target’ has resulted in an ongoing reliance on chemotherapy alone. This review details progress in the three main sub-groups: ER positive, HER2-negative BC, HER2-positive BC, and basal-like (ER and HER2-negative) BC.
(click to enlarge)
ER-positive, HER2-negative ABC
Endocrine therapy (ET) remains as the standard first-line treatment in patients with ER-positive, HER2-negative ABC with the exception of those patients presenting with rapidly progressive disease and visceral compromise. In these cases, chemotherapy should be considered to achieve a quicker disease response.
The mechanism of action of endocrine therapy varies according to the agent employed. Strategies include reduction in oestrogen production (aromatase inhibitors), blocking signalling through the ER (fulvestrant), or antagonism of the ER itself (tamoxifen). Aromatase inhibitors (AI), tamoxifen and fulvestrant have all shown efficacy in post-menopausal women. The selection of one agent over another will often be guided by the form and duration of ET used in the adjuvant setting. For premenopausal women with intact ovarian function, temporary ovarian suppression by using gonadotropin-releasing hormone agonists (GnRH agonists), permanent ovarian ablation by oophorectomy or ovarian irradiation is often considered to allow the use of agents that have proven benefits in the postmenopausal setting.
The greatest challenge in the management of hormone-sensitive ABC is the development of endocrine resistance. This is categorised as primary or secondary resistance. Primary resistance is defined as relapse within two years of commencing adjuvant ET or progression within six months of first-line ET in advanced disease. In contrast, secondary resistance is relapse on ET after two years, relapse within 12 months of completing adjuvant therapy, or progression after six months of ET for ABC. Mechanisms of endocrine resistance have been identified but developing therapies to overcome these has been challenging. To date, drugs demonstrating promising results in this space include fulvestrant, palbociclib and everolimus.
Fulvestrant
Fulvestrant is an ER antagonist that blocks ER dimerisation and DNA binding, increases ER turnover and inhibits nuclear uptake of the receptor.2 It is postulated to overcome endocrine resistance as it blocks ER function before oestrogen can bind the receptor. Its progress as a therapeutic agent in ABC has been slow as an inferior dose regimen (250mg) was used in early studies. Based on data from the CONFIRM trial, the optimal dose is 500mg administered intramuscularly on day one, 14 and 29 and every 28 days thereafter.3 Data supporting the use of first-line fulvestrant in the FIRST trial was presented at the San Antonio Breast Cancer Symposium in 2014. In this phase 2 trial, 205 patients were randomly assigned to fulvestrant or anastrozole. Fulvestrant resulted in a 10- and six-month improvement in progression-free survival (PFS) and overall survival (OS) respectively.4 The confirmatory phase 3 FALCON study has completed accrual and results are awaited to determine its place in the management of ABC.
Palbociclib
Palbociclib is an oral inhibitor of cyclin-dependent kinase 4 and 6 (CDK 4/6) and has demonstrated anti-tumour activity in first and second-line therapy when combined with ET. The CDK 4/6 inhibitors bind to CDK 4 and 6 preventing phosphorylation of the Rb protein; this halts cell cycle progression and induces G1 cell cycle arrest. Cells with intact Rb protein are required for CDK4/6 inhibitors to be effective and thus, the luminal subtype acts as a proxy for predicting efficacy.5
PALOMA-1 was an open label phase 2 trial that randomised 165 post-menopausal women with hormone receptor (HR)-positive, HER2-negative ABC to first-line letrozole plus palbociclib or letrozole alone. Patients who received the combination had a 10-month improvement in PFS (20 v. 10 months). The benefit occurred early and was sustained. However, there was a higher incidence of neutropenia and fatigue. Approximately one-third and one-half of patients had received adjuvant ET or chemotherapy respectively.6 On the basis of this trial, the combination received FDA accelerated approval as first-line therapy in the US in February 2015. A confirmatory phase 3 PALOMA-2 trial has completed accrued and the analysis is awaited
Based on these results, postmenopausal women who progress 12 months from the end of adjuvant ET, or present with de novo ABC, should be considered for an AI or fulvestrant and we await the results of the phase 3 trial investigating an AI with palbociclib. Performance status and preferences of the patient should be considered in selecting first-line therapy.
Second-line therapy
Deciding optimal second- and third-line therapy is challenging due to a dearth of large clinical trials. Patients with good performance status who progress after six months of first-line ET should be considered for second-line ET. Options include a non-cross-resistant AI, tamoxifen, ET in combination with everolimus, an inhibitor of mammalian target of rapamycin (mTOR), or fulvestrant plus palbociclib.
Exemestane, a steroidal aromatase inhibitor, used in second-line after progression on a nonsteroidal AI was evaluated in a 2011 systematic review. The overall response rate (ORR) ranged from 2% to 26% with a clinical benefit rate ranging from 12% to 55%. An emerging mechanism of endocrine resistance is aberrant signalling through the phosphatidylinositol 3-kinase (PI3K)-Akt-mTOR pathway. Everolimus is a sirolimus derivative that inhibits mTOR. Its therapeutic benefit was investigated in the phase 3 BOLERO-2 study, where 724 patients who had progressed on anastrozole were assigned to exemestane or exemestane plus everolimus. Combination therapy resulted in a higher ORR (9.5 v. 0.4%), an improvement in PFS (seven v. three months) but no difference in OS and very significantly more grade 3 and 4 toxicity compared to exemestane alone.7 Drug-related toxicity, particularly stomatitis and pneumonitis, has been the rate limiting step for enthusiasm for this drug combination.
PALOMA-3 is a randomised double-blind placebo controlled phase 3 trial in 521 women with HR-positive, HER2-negative ABC evaluating the addition of palbociclib to fulvestrant v. fulvestrant alone. Pre- and peri-menopausal women were eligible and received goserelin. At the recent ASCO 2015 meeting, a 5.4 month improvement in PFS was observed with the addition of palbociclib to fulvestrant (9.2 v. 3.8 months). Overall, one-third of patients required a dose reduction, mostly for grade 3 neutropenia, but few discontinued treatment. The rate of febrile neutropenia was low. OS data is awaited.8 The introduction of CDK4/6 inhibitors represents an important advance in HR-positive ABC but how best to incorporate them into treatment paradigms is still being established. Many other similar agents such as ribociclib and abemeciclib are being evaluated.
Endocrine resistance
Other strategies to overcome endocrine resistance continue to be explored. Entinostat, a small molecule inhibitor of class 1 histone deacetylases (proteins required for the control of gene expression), exerts an anti-proliferative effect and promotes apoptosis in breast cancer cell lines. The ENCORE 301 randomised phase 2 trial assigned women who had progressed on AI therapy to exemestane or exemestane plus entinostat. A total of 62% of patients had prior chemotherapy. Patients receiving combination therapy demonstrated a significantly improved PFS (four v. two months) and a higher rate of fatigue, nausea, peripheral oedema and uncomplicated neutropenia compared to patients on exemestane alone.9 A phase 3 study is ongoing.
The phosphatidylinositol-3-kinase (PI3K)-Akt-mTOR signalling pathway plays a critical role in mediating cell growth, survival, and angiogenesis. Mutations in the PI3K pathway are commonly observed in HR-positive ABC. A number of agents targeting components of the pathway are being evaluated in clinical trials including several pan-PI3K inhibitors, eg. BKM120 (buparlisib) and GDC-0941 (pictilisib). Finally, androgen receptor (AR) expression is observed frequently in HR-positive ABC. Preclinical evidence has demonstrated synergism between ER and AR targeting.10 A randomised phase 2 trial of exemestane with or without enzalutamide is in progress in this group.
In women who progress following two lines of ET, subsequent treatment should be selected based on prior response, tumour burden and patient preference. Patients with slowly progressive, asymptomatic disease may continue and even benefit from further lines of ET but chemotherapy is the mainstay of treatment in endocrine refractory disease.
HER2-positive ABC
Approximately 20% of breast cancer expresses the human epidermal growth factor receptor 2 (HER2). In the past, overexpression of HER2 was a biomarker for a more aggressive subtype and poorer outcomes. However, advances in therapy for HER2-positive breast cancer have resulted in a dramatic improvement in the prognosis of patients affected by this disease. Recently, there has been a doubling of the number of anti-HER2 agents licensed for clinical use and several more remain under evaluation.
In 2001, Slamon et al reported a significant OS advantage (25.1 v. 20.3 months) when the humanised monoclonal antibody against HER2 (trastuzumab) was added to chemotherapy compared with chemotherapy alone.11 For over a decade, the combination of trastuzumab plus a taxane became standard first-line therapy in HER2-positive ABC with a PFS of approximately 12 months. In 2014, results from the CLEOPATRA study changed this paradigm. This phase 3 trial randomised 808 women to pertuzumab (a humanised monoclonal antibody targeting another epitope of the extracellular domain of HER2), trastuzumab and docetaxel compared with trastuzumab and docetaxel alone. The hypothesis was that blocking the heterodimerisation of HER2 receptor with other HER family members would result in additional therapeutic benefit. This strategy proved correct. The pertuzumab combination resulted in superior PFS (18.5 v. 12.4 months) and importantly, OS (56.5 v. 40.8 months). The majority of patients were trastuzumab-naïve or had at least a 12 month disease-free interval.12 The optimal duration of HER2 blockade is currently unknown but once best response is achieved, discontinuation of the cytotoxic agent and continuation of dual anti-HER2 therapy alone is reasonable. Important to note is that 5% to 10% of patients achieved a complete radiological response on this trial.
Trastuzumab emtansine (T-DM1) is commonly considered for second-line treatment. T-DM1 is an antibody drug conjugate composed of trastuzumab, a thioether linker and the microtubule inhibitor, mertansine (DM1). The cytotoxic DM1 is released within the target cells upon degradation of the human epidermal growth factor 2-T-DM1 complex in the lysosomes. This intracellular delivery spares non-target cells of toxicity seen with chemotherapy. In the EMILIA trial, 978 patients who had previously received trastuzumab and taxane were randomised to T-DM1 or lapatinib and capecitabine. At a median follow-up of 19 months, patients on T-DM1 had improved PFS (10 months v. six months) and improved OS (31 months v. 25 months) with less toxicity.13 Furthermore, in the heavily pre-treated patient population of the TH3RESA trial (greater than two lines of HER2-directed therapy), patients still appear to derive benefit from T-DM1. In this phase 3 trial, 602 patients were randomised to T-DM1 or physicians choice. Patients treated with TDM-1 had a significant PFS advantage (6.2 v. 3.3 months).14 There is limited data to guide treatment of patients who relapse on or shortly after adjuvant trastuzumab, but in EMILIA, the OS advantage for T-DM1 in 118 patients treated in this setting appeared similar to the effect seen overall.13 Hence, T-DM1 is the preferred choice for patients progressing after at least one line of trastuzumab-based therapy.
HER2 blockade
The duration of HER2 blockade in metastatic disease has been examined. The continuation of HER2 blockade while altering the chemotherapy backbone has demonstrated a PFS advantage.15 Importantly, this benefit has only been seen with trastuzumab to date and there is no data supporting the use of ongoing dual blockade with trastuzumab and pertuzumab or T-DM1 use beyond progression.
The role of ET in combination with HER2 blockade in patients with HER2-positive, ER-positive ABC has yielded disappointing results. While a PFS benefit has been identified in two large phase 3 trials, the results fell short of that reported with chemotherapy in combination with HER2 blockade.16,17 Nevertheless, there are a small number of patients where front-line ET and anti-HER2 therapy is reasonable, eg. in patients with indolent bone-only disease or those with poor performance status.
Despite significant advances, several questions remain. Can we individualise therapy based on a biomarker-led approach and avoid chemotherapy in some patients? As our systemic therapy improves, the occurrence of brain metastases remains a significant therapeutic challenge. Will the small molecule tyrosine kinase inhibitors such as lapatinib and neratinib prove beneficial in treating or preventing brain metastases? Finally, how do we optimise the value of these agents in an era of rising healthcare costs?
Basal-like or ‘triple negative’ (TNBC) subtype
Basal-like or triple negative breast cancer is estimated to account for 12% of breast cancers. Lacking ER, PR and HER2, TNBC is not amenable to targeted therapies against these, so chemotherapy remains the mainstay of treatment. In the face of advances in other subtypes, it has remained challenging to treat this disease particularly in the metastatic setting. There is significant clinical, pathological and molecular heterogeneity within this group and because it is mutationally diverse, there remain no clear targetable mutations.
A molecular classification suggesting six transcriptional subtypes has been proposed: Basal-like 1 and 2, immunomodulatory, mesenchymal, mesenchymal stem-like and luminal androgen receptor (LAR). Patients with basal-like subtypes often have BRCA mutations and show sensitivity to DNA damaging agents including platinum and PARP inhibitors, which have been the focus of recent studies.
The LAR dependent subtype is associated with better outcomes and is present in 10% to 30% of TNBC. They appear to be poorly responsive to traditional chemotherapy. Data presented at ASCO 2015 by Tung et al demonstrated that AR expression was associated with PD-L1 expression, older age, grade 1 or 2 tumours and rarely co-existed in BRCA mutation carriers.18 Androgen antagonists are being evaluated in this group which is also enriched for PIK3CA mutations and the combination of enzalutamide and a PIK3CA inhibitor is being assessed.
The current standard of care is sequential single agent chemotherapy. There are several options: anthracycline, taxane, capecitabine, vinorelbine, eribulin and platinum, with no defined optimal sequence. Combination chemotherapy is generally reserved for patients with visceral crisis or highly symptomatic disease. Choice of agent may be based on patient characteristics and preferences eg. alopecia, cardiac morbidity, oral therapy, diabetes, hepatic dysfunction etc. A predilection for the brain makes brain metastases a common encounter. There is some evidence that capecitabine crosses the blood brain barrier and may be appropriate in patients with brain metastases.19 Finally, there is no predetermined duration of therapy but a benefit in PFS may be seen with maintenance therapy, especially in young women.20
Going forward, clinical progress in this group is likely to be slow as we continue to sub-divide an already small patient group. Global collaboration in clinical trials is essential to further progress the management of this often aggressive disease sub-group.
Supportive care
The use of bisphosphonates and RANK ligand (RANKL) inhibitors have radically reduced the risk of skeletal-related events (SRE) in patients with breast cancer. Dosing schedules have been extensively investigated and while we would have recommended four-weekly bisphosphonate administration, results from the recently presented OPTIMIZE-2 trial are re-assuring. In this phase 3 trial, administration of zoledronic acid every 12 weeks resulted in a non-inferior skeletal event rate when compared to monthly administration.21 Reduced dosing will potentially lower the risk of toxicity and cost. The optimal duration of these drugs remains uncertain.
Denosumab is a monoclonal antibody that binds to RANKL, a protein involved in the formation, function and survival of osteoclasts. Increased osteoclast activity, stimulated by RANKL, is a mediator of bone pathology in bone metastases from solid tumours.22 A large phase 3 trial enrolled 2,046 patients with ABC. Patients were randomly assigned to subcutaneous denosumab (120mg) or intravenous zoledronic acid every four weeks. Denosumab resulted in a statistically significant delay in the time-to-first and subsequent SRE. No difference in OS was observed. Adverse reactions included osteonecrosis of the jaw and hypocalcemia. These occurred more frequently in patients treated with denosumab.23
Finally, the benefit of early palliative care has been demonstrated in other advanced malignancies, with improvements in quality of life and OS. As we continue to explore novel therapies and improve outcomes for our patients, it is important that they are offered early palliative input in order to optimise their quality of life. The All-Ireland Cooperative Oncology Research Group (ICORG) has completed a national ABC survey examining if the needs of patients with ABC in Ireland are being met. These results are awaited.
Real advances in the treatment of ABC have occurred and are continuing. Progress has been more marked in certain disease subtypes. While a tailored treatment approach has been achieved for the HER2-positive subtype, basal-like subtype continues to be treated with a ‘one size fits all’ approach. We have many challenges ahead. First, we must continue to identify targets that translate into a meaningful focus for new therapies and second, this must be achievable at an acceptable cost. Clearly a global collaborative effort on both parts is the only way forward.
References
Dawood S, Broglio K, Gonzalez-Angulo AM, et al. Trends in survival over the past two decades among white and black patients with newly diagnosed stage IV breast cancer. J Clin Oncol 2008; 26: 4891
DeFriend DJ, Howell A, Nicholson RI, et al. Investigation of a new pure antiestrogen (ICI 182780) in women with primary breast cancer. Cancer Res 1994; 54: 408
Di Leo A, Jerusalem G, Petruzelka L, et al. Results of the CONFIRM phase III trial comparing fulvestrant 250mg with fulvestrant 500mg in postmenopausal women with estrogen receptor-positive advanced breast cancer. J Clin Oncol 2010; 28(30): 4594–4600
Robertson JF, Llombart-Cussac A, Feltl D, et al. Fulvestrant 500 mg v. anastrozole as first-line treatment for advanced breast cancer: Overall survival from the phase II “first” study. 2014 San Antonio Breast Cancer Symposium; Abstract S6-04
Finn RS, Dering J, Conklin D, et al. PD 0332991, a selective cyclin D kinase 4/6 inhibitor, preferentially inhibits proliferation of luminal estrogen receptor-positive human breast cancer cell lines in vitro. Breast Cancer Res 2009; 11: R77
Finn RS, Crown JP, Lang I, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole v. letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol 2015; 16: 25
Piccart M, Hortobagyi GN, Campone M, et al. Everolimus plus exemestane for hormone-receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer: overall survival results from BOLERO-2. Ann Oncol 2014; 25: 2357
Turner NC, Ro J, André F, et al. Palbociclib in Hormone-Receptor-Positive Advanced Breast Cancer. N Engl J Med 2015; 373: 209
Yardley DA, Ismail-Khan R, Klein P. Results of ENCORE 301, a randomized, phase II, double-blind, placebo-controlled study of exemestane with or without entinostat in postmenopausal women with locally recurrent or metastatic estrogen receptor-positive (ER+) breast cancer progressing on a nonsteroidal aromatase inhibitor (AI). J Clin Oncol 2011; s27: 268
Cochrane DR, Bernales S, Jacobsen BM, et al. Role of the androgen receptor in breast cancer and preclinical analysis of enzalutamide. Breast Cancer Res 2014; 16: R7.
Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 2001; 344: 783
Swain SM, Baselga J, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med 2015; 372: 724
Verma S, Miles D, Gianni L, et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med 2012; 367: 1783
Krop IE, Kim SB, González-Martín A, et al. Trastuzumab emtansine v. treatment of physician’s choice for pretreated HER2-positive advanced breast cancer (TH3RESA): a randomised, open-label, phase 3 trial. Lancet Oncol 2014; 15: 689
von Minckwitz G, du Bois A, Schmidt M, et al. Trastuzumab beyond progression in human epidermal growth factor receptor 2-positive advanced breast cancer: a german breast group 26/breast international group 03-05 study. J Clin Oncol 2009; 27: 1999
Kaufman B, Mackey JR, Clemens MR, et al. Trastuzumab plus anastrozole v. anastrozole alone for the treatment of postmenopausal women with human epidermal growth factor receptor 2-positive, hormone receptor-positive metastatic breast cancer: results from the randomized phase III TAnDEM study. J Clin Oncol 2009; 27: 5529
Johnston S, Pippen J Jr, Pivot X, et al. Lapatinib combined with letrozole v. letrozole and placebo as first-line therapy for postmenopausal hormone receptor-positive metastatic breast cancer. J Clin Oncol 2009; 27: 5538
Tung NM, Garber JE, Torous V et al Prevalence and predictors of androgen receptor (AR) and programmed death-ligand 1 (PD-L1) expression in BRCA1-associated and sporadic triple negative breast cancer (TNBC). J Clin Oncol 33, 2015 (suppl; abstr 1005)
Kopf B, De Giorgi U, Zago S, et al. Innovative therapy for patients with brain metastases: oral treatments. J Chemother 2004; 16 Suppl 5: 94
Seidman AD. The search for an elusive uniform strategy for a heterogeneous disease: lesson learned? J Clin Oncol 2013; 31: 1707
Hortobagyi GN, Lipton A, Chew HK, et al. Efficacy and safety of continued zoledronic acid every 4 weeks v. every 12 weeks in women with bone metastases from breast cancer: Results of the OPTIMIZE-2 trial. J Clin Oncol 32:5s, 2014 (suppl; abstr LBA9500)
FDA Approval for Denosumab [Internet] 2013 July 2 [cited 2015 Sept 17]. Available from: http://www.cancer.gov/about-cancer/treatment/drugs/fda-denosumab
Stopeck AT, Lipton A, Body J-J, et al, on behalf of the 20050136 Breast Cancer SRE Study Investigators. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol 2010; 28: 5132-5139
 (click to enlarge)
(click to enlarge)