Pharmacological management of cancer pain in adults – new national guidelines
Exacting standards have been applied to the preparation of new national guidelines for the pharmacological management of cancer pain in adults
Dr Sarah McLean, Specialist Registrar in Palliative Medicine, Royal College of Physicians Ireland, Dublin, Dr Lucy Balding, Consultant in Palliative Medicine, Our Lady’s Hospice and Care Services, Harold’s Cross, Dublin, Dr Michael Lucey, Consultant in Palliative Medicine, Milford Hospice, Limerick, Ms Fiona McGrehan, Clinical Pharmacist, Our Lady’s Hospice and Care Services, Harold’s Cross, Dublin, Ms Cliona Hayden, Clinical Pharmacist, Our Lady’s Hospice and Care Services, Harold’s Cross, Dublin and Dr Karen Ryan, Consultant in Palliative Medicine, Mater Misericordiae University Hospital, Dublin
Estimates indicate that 50-90% of patients with cancer experience pain at some stage.1 There is a clear imperative to make best use of the available evidence, however limited, and to inform, aid, and support healthcare professionals challenged with managing patients experiencing cancer-related pain.
The National Palliative Care Programme set out to produce clinical guidelines for the management of a number of conditions in patients with life-limiting conditions, including depression, and constipation.
Here, we describe the methodology utilised, and challenges experienced, during the process of developing national clinical guidelines for the pharmacological management of cancer pain in adults, and outline some of the key clinical recommendations.
Methods
The potential benefits of guidelines are only as good as the quality of the guidelines themselves. Appropriate methodologies in the guideline development process are important for the successful implementation of the resulting recommendations.2,3 As a framework for the development of the national cancer pain guidelines, the principles of the ADAPTE tool were followed.
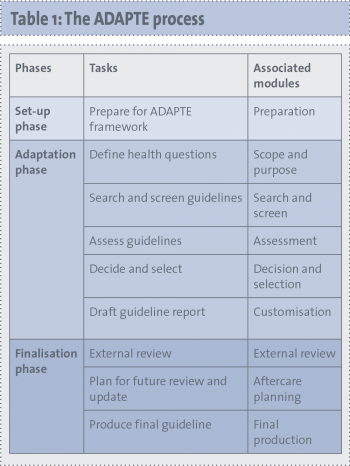
ADAPTE is an international collaboration that aims to promote the development of clinical practice guidelines through the adaptation of existing guidelines produced in one cultural and organisational setting, for application in another context.4 The ADAPTE process is outlined in Table 1.
(click to enlarge)
A formal literature search to identify existing guidelines was undertaken in order to identify those published between 2008 and November 2011 (the time of document preparation). This search detected a number of existing guidelines of widely varying relevance and quality.
Each guideline was assessed using the AGREE (Appraisal of Guidelines Research and Evaluation) II instrument, which is a 23-item guideline appraisal tool that assesses the methodological rigour and transparency with which a guideline is developed. Individual domain and overall scores for each guideline were calculated and tabulated, allowing easy comparison of guidelines.
The rigour score is defined by ADAPTE as ‘a level above which a guideline is deemed acceptable’, ie. the guideline itself may be referenced, rather than a primary evidence source.
Four guidelines met the rigour level for this guideline of 30%: SIGN (Scottish Intercollegiate Guidelines Network) 106,5 which was chosen as the basis for the national cancer pain guidelines; the National Comprehensive Cancer Network (NCCN) Guidelines 2010,6 the Oncology Nursing Society Guidelines 2009,7 and the Palliative Adult Network Guidelines (PANG).8 Recommendations contained within these four guidelines were collated into a recommendation matrix.
In order to address topics, which were either not covered in the SIGN guidelines or were a result of new evidence since publication of SIGN in 2008, 19 health questions were formulated. A systematic review of the evidence was performed, using the PICOT (Population, Intervention, Comparison, Outcome, Timeline) format, to address each individual question. In addition, the evidence from a further 19 questions recently addressed by the EPCRC in comprehensive systematic reviews was assimilated.
Evidence from SIGN, health questions, and the recommendation matrix was collated.
The guidelines were completed in May 2013. From the evidence available, 42 graded recommendations were formulated. Under the auspices of the Clinical Strategy and Programmes Directorate, a national consultation process followed and the feedback provided was considered and incorporated into the guidelines, where appropriate. The guidelines have now been submitted for approval and publication by the HSE. The guidelines will be disseminated nationally through publication on the HSE website, and presentation at conferences, and at regional level by distribution to clinicians. The implementation of the guideline will be facilitated by the educational departments and clinical managers of palliative care services nationally. The guideline document includes a list of topics for clinical audit. Review of the guidelines is scheduled in three years.
Clinical concepts and recommendations
The target users of the guidelines are healthcare professionals involved in cancer pain management, including specialist palliative care professionals, physicians, GPs, and pharmacists. The guidelines are not intended to deal with non-cancer-related acute or chronic pain, or the paediatric population. Pharmaco-economic analysis is outside the scope of the guideline.
A list of the guideline contents, and key-graded clinical recommendations, are contained in Table 2. The evidence and key findings pertaining to individual recommendations are contained within the full text of the draft guidelines.9
(click to enlarge)
(click to enlarge)
Of note, at time of publication of this article, the guidelines remain under review. The recommendations outlined in Table 2 consist only of sample, draft recommendations. It is anticipated that the final guidelines will be published in late 2013.
Conclusion
The national guidelines for the pharmacological management of cancer pain in adults are the first to be developed specifically for the Irish clinical context. The document contains 42 graded recommendations based on best available current evidence. Features unique to these new guidelines, when compared with international cancer pain guidelines, include a section on the management of cancer pain in patients with a history of substance addiction; and a section on the management of pain in patients with hepatic impairment.
Clinical guidelines should allow the implementation of research findings; ensure that clinical decisions are based on evidence rather than opinion; eliminate unexplained variation in practice; and allow optimisation of clinical outcomes and the patient experience. It is well recognised internationally that the development, dissemination, implementation, and regular review of high-quality clinical guidelines require substantial resources. In particular, regular audit is required in order to ensure the implementation of standards set out in clinical guidelines.
International experience has led to a reformulation of adaptation methodology in order to avoid duplication of effort, and an emphasis on improved resource sharing. The template utilised in the development of these national guidelines for the pharmacological management of adult cancer pain is now being used nationally by the Clinical Care Programme for the development of national clinical practice guidelines for the management of all types of cancer, and within palliative care for common symptoms.
It is hoped that these guidelines will not only improve the management of patients with cancer-related pain, but also guide the development of other clinical guidelines in order to improve outcomes and the experience of patients with other conditions.
References
Abernethy AP, Samsa GP, Matchar DB. A clinical decision and economic analysis model of cancer pain management. Am J Manag Care 2003; 9(10): 651-664
AGREE Collaboration. Development and validation of an international appraisal instrument for assessing the quality of clinical practice guidelines: the AGREE project. Qual Saf Health Care 2003; 12(1): 18-23
Shaneyfelt TM, Mayo-Smith MF, Rothwangl J. Are guidelines following guidelines? The methodological quality of clinical practice guidelines in the peer-reviewed medical literature. JAMA 1999; 281(20): 1900-1905
Fervers B, Burgers JS, Haugh MC et al. Adaptation of clinical guidelines: literature review and proposition for a framework and procedure. Int J Qual Health Care 2006; 18(3): 167-176
Scottish Intercollegiate Guidelines Network. SIGN. Control of pain in adults with cancer. A national clinical guideline (106). NHS. Edinburgh, 2008
NCCN. In: NCCN, editor
Aiello-Laws L, Reynolds J, Deizer N et al. Putting evidence into practice: what are the pharmacologic interventions for nociceptive and neuropathic cancer pain in adults? Clin J Oncol Nursing 2009; 13(6): 649-655
Watson M, Lucas C, Hoy A, Back I, Armstrong P, eds. (2011) Palliative Adult Network Guidelines (PANG). 3rd ed: (Nine cancer Networks across the UK)
 (click to enlarge)
(click to enlarge)

