The common misconception of chickenpox as a relatively harmless childhood illness may be
changing in line with increased awareness of its potentially severe complications
Dr Karen McCarthy, Specialist Registrar in Paediatric Infectious Disease, Our Lady's Children's Hospital, Crumlin and Dr Patrick Gavin, Consultant in Paediatric Infectious Disease, Our Lady's Children's Hospital, Crumlin
Varicella zoster virus (VZV) is a pathogenic human herpes virus that is found worldwide. Primary infection causes chickenpox. Following primary infection, VZV establishes latency in sensory neurons of the peripheral dorsal root, cranial nerve, autonomic and enteric ganglia. Thereafter, reactivation, as a result of decreased cell-mediated immunity or other triggering factors, causes shingles (herpes zoster). In the pre-vaccine era, in temperate climates, chickenpox occurred with seasonal peaks from January to April and epidemics every two to five years.1 Most children in Ireland have had chickenpox by the age of 10. Approximately one in three individuals will develop shingles over their lifetime. Nevertheless, chickenpox and shingles, regarded by many as a rite of passage of childhood and an inevitability of ageing, are vaccine-preventable infections.
While chickenpox is generally considered a benign inconvenience of childhood, severe or complicated infection is associated with significant morbidity and mortality. Chickenpox is the most significant risk factor for invasive group A streptococcal (iGAS) disease, including necrotising fasciitis and toxic shock syndrome, and is a common cause of stroke in childhood. In Ireland, varicella infection is responsible for in excess of 220 admissions to public hospitals annually. This results in over 1,100 inpatient and 150 intensive care unit bed days/year.2
In contrast, countries where universal chickenpox vaccination is part of the childhood immunisation schedule have seen dramatic changes in their epidemiology. In the US, where chickenpox vaccination was first introduced in 1995, chickenpox incidence, complications and deaths in children have declined by over 95%. Moreover, morbidity and mortality in unvaccinated groups and those at risk of severe disease has reduced as a result of herd immunity.
Background
Chickenpox is highly contagious. One case potentially results in 10-12 further infections in susceptible individuals. Secondary attack rates among susceptible individuals within households are between 60-90%. Transmission is by inhalation of airborne droplets or direct contact with skin vesicles containing aerosolised infectious virus, and less frequently by inhalation of infectious respiratory secretions. The virus then incubates in the oropharynx for two weeks (range: 10 to 21 days). Thereafter, infected T lymphocytes enter the circulation and carry the virus to the skin where the characteristic rash develops.1
As viraemia precedes the development of rash, infected individuals can spread the virus from two days before appearance of the rash until all of the skin lesions have crusted five to seven days later3, following which it becomes latent in peripheral ganglia. Decades later, the virus may reactivate either spontaneously or after a number of triggering factors to cause herpes zoster (shingles). Less frequently, individuals with shingles may transmit VZV resulting in chickenpox in non-immune contacts. Infection occurs by direct or indirect contact with non-intact vesicles until all shingles lesions have crusted, typically by five days.
Clinical presentation
Chickenpox
Chickenpox is typically self-limiting, beginning with a prodrome of malaise and low-grade fever, followed by generalised vesicular rash (exanthem, see Picture 1), which is intensely pruritic. The fever typically lasts two to three days. The rash usually begins on the face and progresses to involve the trunk and extremities and frequently involves the mucous membranes (enanthem, see Picture 2).
(click to enlarge)
Lesions number from few to many hundreds, with an average of 300 to 500 lesions in varying stages of development (macules, papules, and vesicles) that subsequently burst, dry and crust over3 following which it becomes latent in peripheral ganglia. Decades later, the virus may reactivate either spontaneously or after a number of triggering factors to cause herpes zoster (shingles).
The rash may be very extensive and haemorrhagic in immunocompromised individuals. Chickenpox infection typically produces lifelong immunity; recurrence is very rare and occurs predominantly in immunocompromised individuals.
Complicated chickenpox
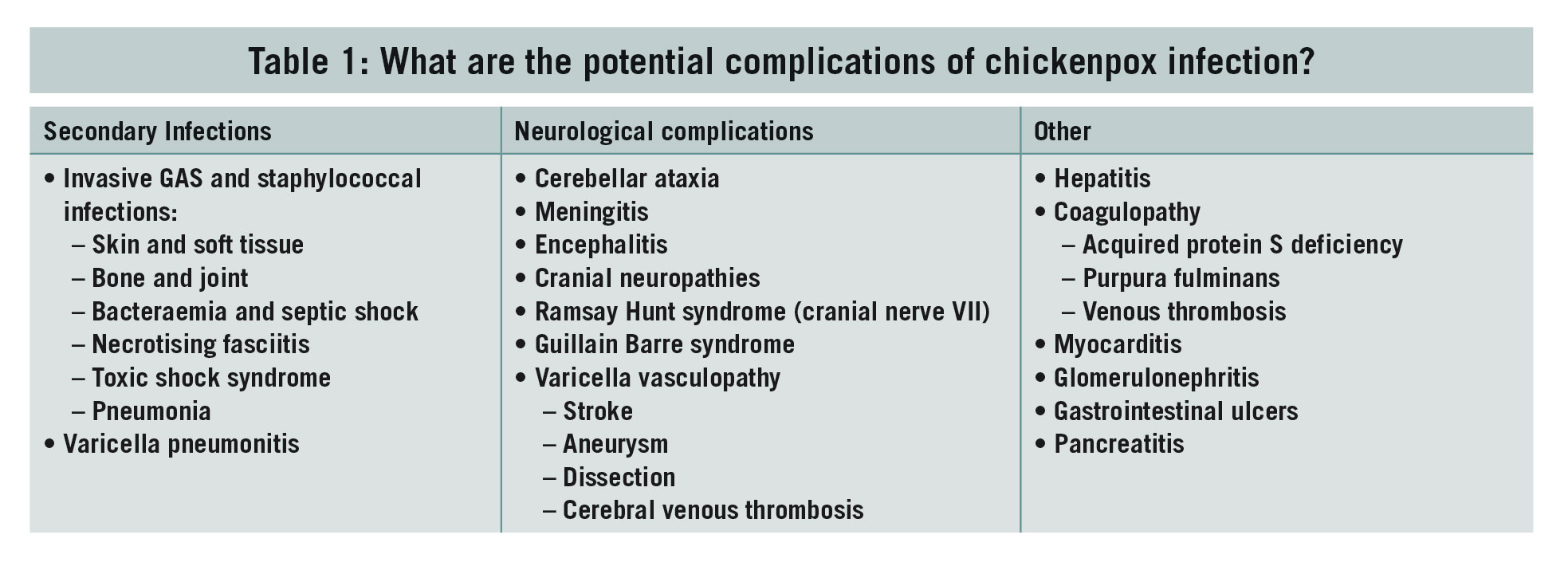
Unfortunately, for some individuals chickenpox is not a benign illness and complications may occur. In Ireland, VZV infection results in an average of five hospitalisations/100,000 population/year, with 30% of patients experiencing significant secondary complications.2 Complications are divided into secondary infectious, neurological and other (see Table 1).
(click to enlarge)
Secondary iGAS or staphylococcal disease is potentially life or limb-threatening. Chickenpox is the most common risk factor for paediatric iGAS disease, including necrotising fasciitis and toxic shock-like syndrome (see Picture 3). Hospitalisations due to iGAS disease have been increasing in Ireland over the past decade.2 In a recent series of iGAS cases presenting to the Temple Street Hospital, 70% had active chickenpox.
Bacterial super-infection (see Picture 4) complicating chickenpox should be suspected in any child with fever that persists or recurs beyond four to five days of illness, where severity of pain is disproportionate, or with redness and swelling around skin lesions.
(click to enlarge)
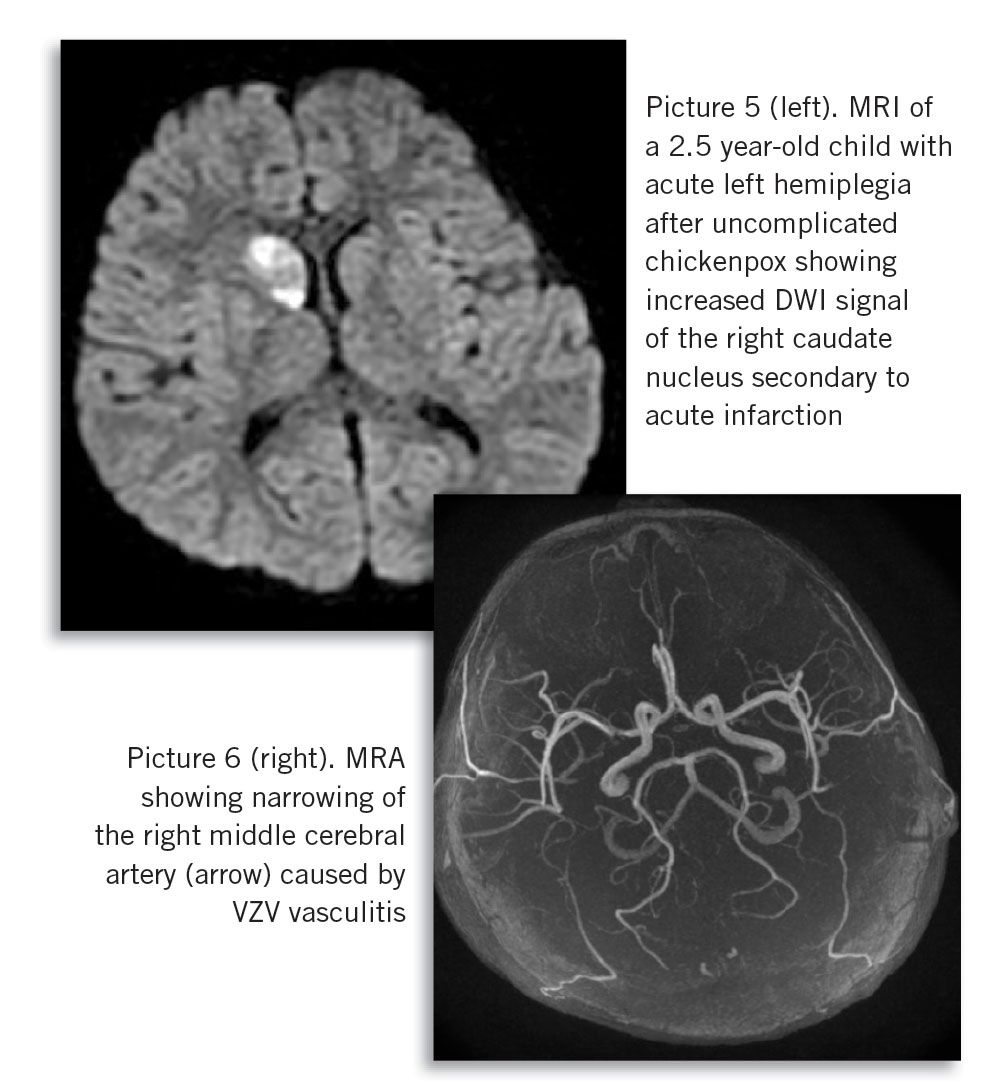
In contrast to bacterial super-infection, neurological complications (see Picture 5 and 6) of chickenpox caused by virus reactivation or post-inflammatory, typically present after a delay, at a time distant from chickenpox infection, making the diagnosis more challenging. Risk of chickenpox complications is increased in children less than one year or over 15 years old, in pregnant women and in the immunocompromised. However, the majority of complicated chickenpox cases occur in previously healthy children.
(click to enlarge)
Shingles
Reactivation of VZV manifests as shingles or herpes zoster. Approximately one in three individuals will develop shingles over their lifetime, with two-thirds of cases occurring after 50 years of age. Reactivation occurs due to age-related immunosenescence or is triggered by other infections or immunosuppressing conditions or medication.
Shingles presents as acute pain or itching in the sensory distribution of the affected dorsal root ganglia followed by a vesicular rash in that area. Lesions most commonly occur unilaterally along a thoracic dermatome. Less commonly, shingles reactivation is disseminated affecting three or more dermatomes. Rarely, reactivation (with dermatomal pain) occurs without rash, ‘zoster sine herpete’.
Associated symptoms include headache, photophobia and malaise. Shingles typically lasts for five days; lesions heal over one month, but may leave residual pigmentation or scarring. Post-herpetic neuralgia, defined as radicular pain in the area of rash that persists three months after an episode, occurs in approximately 15% of cases (more frequently with increasing age) and may last for months to years.1
Varicella infection in pregnancy
Varicella infection in pregnancy requires special consideration. Firstly, chickenpox infection in the second and third trimester of pregnancy may cause severe and complicated maternal infection, particularly varicella pneumonia. Furthermore, VZV can cross the placenta and is potentially teratogenic. Infection prior to 20 weeks gestation may result in congenital varicella syndrome, which carries high foetal mortality or the potential for multiple anomalies that include: skin scarring; cortical atrophy and microcephaly; micropthalmia, chorioretinitis and cataracts; limb hypoplasia; and intrauterine growth retardation.4
Thankfully, congenital VZV infection is very rare with an incidence of 1-2% in the event of maternal chickenpox up to 20 weeks gestation, and only rare reports associated with chickenpox later in pregnancy. Congenital varicella syndrome has also been reported rarely in association with maternal shingles.5 In addition, maternal chickenpox infection from one week before to one week after delivery carries the risk of severe neonatal chickenpox (highest risk five days before to two days after).
Diagnosis
Chickenpox and shingles are clinical diagnoses. However, if there is diagnostic uncertainty, atypical presentation or breakthrough infection post-vaccination, vesicular fluid may be tested for VZV by PCR in the National Virus Reference Laboratory, University College Dublin. Cerebrospinal fluid may also be tested by PCR in cases of suspected varicella encephalitis or meningitis.
Management
Treatment of uncomplicated chickenpox in healthy children is limited to symptomatic relief, and antiviral medications are not recommended. Paracetamol is the antipyretic of choice given the association between aspirin and Reye’s syndrome and the epidemiological (although not causal) association between ibuprofen and increased risk of iGAS disease.6,7 High-dose intravenous acyclovir reduces visceral dissemination of the virus. Antiviral medications may be considered in severe chickenpox or in individuals at greater risk of developing complications. Neonates born to mothers who develop chickenpox in the week before or after delivery are usually hospitalised for observation and pre-emptive IV antiviral treatment.8 If oral therapy is being considered for individuals at increased risk of moderate to severe infection, valacyclovir has improved bioavailability and the advantage of less frequent daily dosing.8 Shingles should be treated promptly with oral antiviral agents, or intravenously if severe or disseminated.
Vaccination
Chickenpox vaccine has been around for a long time. The first successful live attenuated vaccine was developed by Takahashi in Japan in 1974.9 The WHO recommends that countries where varicella is an important public health burden should consider introducing chickenpox vaccination into routine childhood immunisation programmes.10
The US introduced universal chickenpox vaccination for healthy children from 12 months of age in 1995. However, most European countries have been slow to do so. At present, universal varicella vaccination is recommended in the US, Canada and Australia, nationally in six European countries and regionally in two.11 While chickenpox vaccine is licensed in Ireland since 2003, it is not yet recommended as part of the primary immunisation schedule, but parents may seek vaccination privately.8
Varicella zoster vaccine
Varicella vaccine (Varivax) is a live attenuated viral vaccine available as a lypophilised preparation for reconstitution with a diluent.12
A dose of 0.5ml is given intramuscularly (or subcutaneously if intramuscular injections are contraindicated) in the anterolateral thigh (infants) or deltoid (adults). Healthy children from 12 months of age should receive two doses of chickenpox vaccine at least one month apart. Infants from nine months of age may receive chickenpox vaccine in the setting of an outbreak, with the follow-up dose deferred for three months after the initial dose. Vaccination is highly effective with protective antibody levels in 85-95% of vaccinated children after one dose and 99% after two doses.13,14 Breakthrough chickenpox may occur rarely in vaccinated individuals but is usually milder with fewer lesions, fewer complications and reduced risk of transmission.
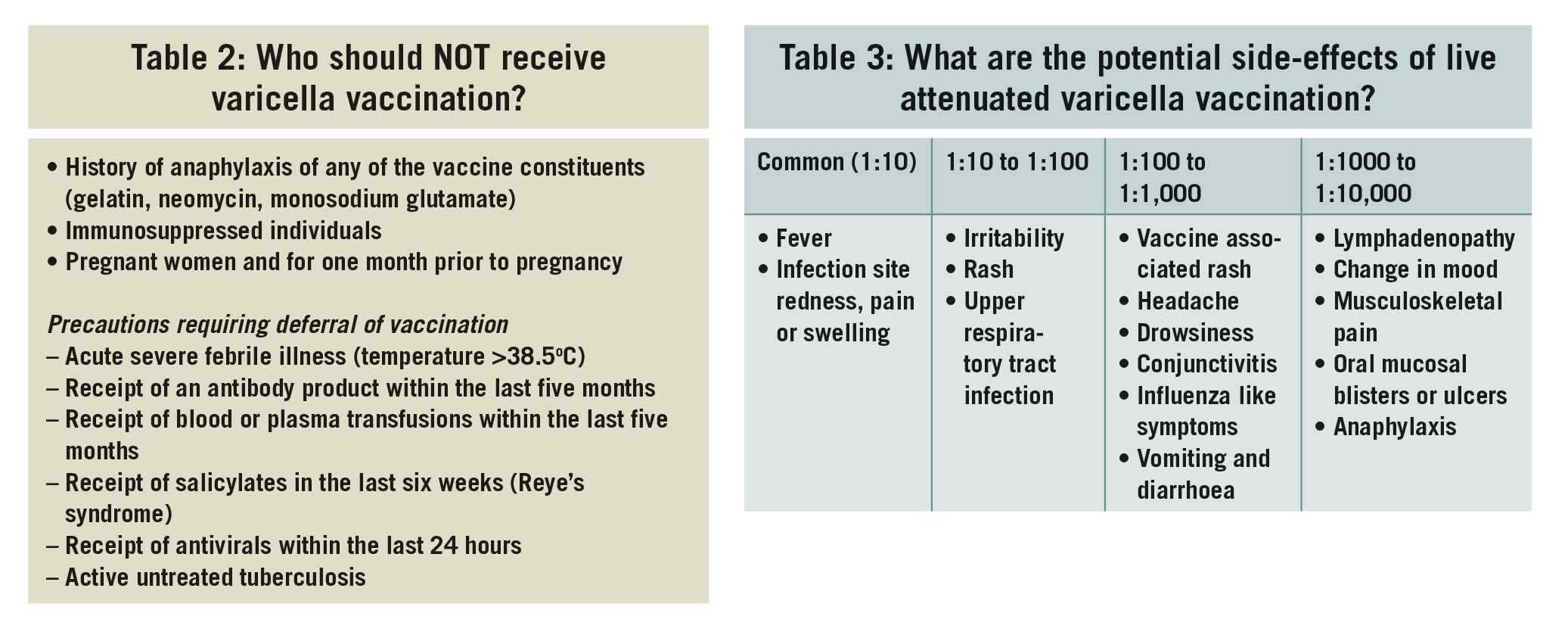
Contraindications to chickenpox vaccine are relatively few (see Table 2).8 Importantly, treatment with low-dose oral (< 2mg/kg/day), topical, replacement or inhaled steroids is not a contraindication to receipt of chickenpox vaccine. While pregnant women should not receive chickenpox vaccine, non-immune pregnant women can safely receive vaccine after delivery.
Vaccine virus is not transmissible in breast milk and breastfeeding is not a contraindication to receipt of chickenpox vaccine for non-immune mothers. Chickenpox vaccine is not contraindicated in household contacts of pregnant women or in immunocompromised individuals who cannot receive vaccine themselves.
In point of fact, vaccination of household contacts of at-risk individuals represents an opportunity to protect their non-immune household and pregnant contacts. While chickenpox infection caused by reactivation of vaccine virus is described occasionally (c. 2%), the resulting rash rarely vesiculates and transmission of vaccine virus to non-immune contacts is extraordinarily rare.
Chickenpox vaccine is safe and generally well tolerated. Common side effects include fever, pain, redness and swelling at the injection site (Table 3). Serious adverse reactions occur almost exclusively in individuals with unrecognised immunocompromise. Chickenpox vaccine can be safely administered at the same time as other vaccines, although if not given simultaneously, it should be given at least four weeks before or after other live vaccines such as MMR.
(click to enlarge)
Herpes zoster (shingles) vaccine
Herpes zoster vaccine (Zostavax) is a live attenuated viral vaccine licensed in those over 50 for prevention of zoster and zoster-related post-herpetic neuralgia.15 It is administered at a single dose of 0.65ml subcutaneously in the deltoid region. Each dose contains c. 14 times the amount of vaccine strain virus found in chickenpox vaccine. Vaccination reduces the incidence of shingles by about 50%, duration and severity of symptoms if disease occurs and incidence of post-herpetic neuralgia by about two-thirds16 (67% in PHN and 73% in severe cases of zoster).17
Herpes zoster vaccine can be administered to individuals with a previous history of shingles to boost immunity and may be given at the same time as seasonal influenza vaccine. Co-administration with PPV23 is also possible, according to the latest SmPC. Contraindications to receipt of the vaccine are similar to those for chickenpox vaccine.
Post-exposure prophylaxis
Chickenpox’s relatively long incubation period provides an opportunity for post-exposure prophylaxis with chickenpox vaccine, varicella zoster immunoglobulin (VZIG) or antiviral treatment to abort, modify or reduce the severity of subsequent infection, but timing is critical. Chickenpox vaccine administered to non-immune children over 12 months of age or adults within three days (and possibly up to five days) of chickenpox or shingles exposure, may prevent or reduce severity of infection. In the absence of contraindication to vaccination, chickenpox vaccine is the prophylactic strategy of choice as it induces protection against subsequent exposure, whereas passive immunity provided by VZIG wanes (usually after one month).
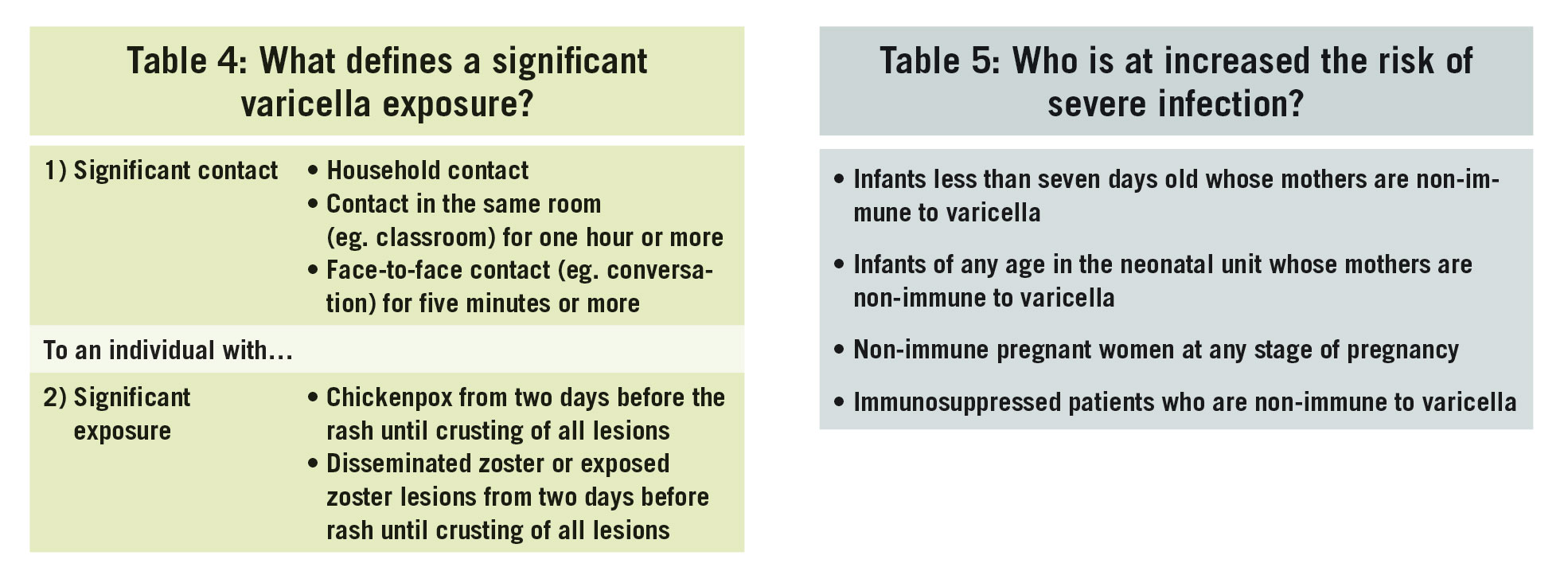
Where chickenpox vaccine is contraindicated, VZIG may be given to non-immune children from 12 months of age and older who have a significant chickenpox or shingles exposure (see Table 4) and an underlying condition that increases the risk of severe infection (see Table 5). VZIG should be given as soon after exposure as possible and preferably within four days for maximal effectiveness. Patients receiving monthly immunoglobulin replacement therapy for antibody deficiency do not require additional prophylaxis.
(click to enlarge)
VZIG is available as intravenous and intramuscular preparations. Intramuscular VZIG (VZIG BPL) is available as a 250mg vial (100iu VZab/ml). Dosing is age-dependent and is generally not suitable for children where high-volume intramuscular injections pose a problem. Intravenous VZIG (Varitect CP) is available in 5ml or 20ml vials and is administered at a dose of 25IU/kg body weight IV.8 Potential side-effects include nausea, chills, fever, headache, vomiting and allergic reaction. The efficacy of live attenuated varicella vaccination is impaired following administration of immunoglobulin and should be deferred for five months.
Beyond these time periods, pre-emptive oral acyclovir or valacyclovir administered for seven days from day seven to 10 after exposure may reduce the severity of subsequent illness. Post-exposure prophylaxis is not indicated in otherwise healthy term infants older than seven days. Term infants born to immune mothers (who have a history of chickenpox or VZV vaccination) are generally protected by maternal antibody for the first year of life and do not require prophylaxis following exposure to chickenpox or shingles.
In cases where doubt regarding maternal immunity exists, rapid maternal serologic testing for varicella antibody is available (through the National Virus Reference Laboratory, UCD). Premature infants (< 28 weeks) born to immune mothers may lack protective maternal antibodies and should have varicella serology performed in the event of a significant exposure. Excellent guidelines on post exposure prophylaxis, particularly for young infants, are available at: www.hse.ie/eng/health/immunisation/hcpinfo/ guidelines/ (Chapter 23, Varicella Guidelines).
Why is the chickenpox vaccine not incorporated into primary immunisation?
In Ireland, only hospitalised laboratory-confirmed cases of chickenpox are notifiable to the Health Protection Surveillance Centre. However, because most VZV infection is diagnosed clinically without laboratory confirmation and is therefore not notifiable, rates of hospitalisation and severe infection are likely a significant underestimate. Nevertheless, existing hospital inpatient enquiry data demonstrate that VZV infection places a consistent and predictable annual burden on the Irish healthcare system.2
(click to enlarge)
The WHO advises universal varicella vaccination for countries where varicella remains a public health problem, providing resources are sufficient to ensure and maintain high vaccination coverage (> 80%).18 Chickenpox vaccine is part of universal childhood immunisation schedules in the US, Canada, Australia and many of our European neighbours. A safe, highly effective, tried and tested vaccine is available and licensed in Ireland for use in healthy children over 12 months of age.
Why then, is chickenpox vaccine not part of the routine childhood immunisation schedule in Ireland? The argument against universal childhood varicella immunisation centres around concerns about a potential shift of incidence of chickenpox to older age-groups (who tend to have more complicated disease), increased risk of shingles in the elderly, and cost-effectiveness of a national two-dose vaccination programme.19 Data to support these concerns, particularly in relation to increasing the age-profile for chickenpox and the incidence of shingles, are controversial.
Studies of vaccine impact in countries following introduction of universal childhood chickenpox vaccination do not support the theoretical shift in chickenpox incidence to non-immune older age groups. In fact, post-vaccine surveillance demonstrates decreased overall incidence of chickenpox, including among older age-groups, and a herd-immunity effect with indirect protection among susceptible groups who cannot themselves receive chickenpox vaccine (children under one year of age, non-immune pregnant women and the immunocompromised).19,20
Similar concerns that introduction of universal childhood chickenpox vaccination would lead to increased incidence of shingles and its complications in the elderly (by reducing natural boosting of immunity from exposure to children with chickenpox) have not been borne out.21 In fact, the incidence of shingles has been increasing at the same rate in countries with and without chickenpox vaccination programmes. Local data from the ICGP sentinel network demonstrates a significant increase in average annual incidence of shingles in Ireland from 2005 to 2016 (p < 0.04) in the absence of routine chickenpox vaccination.22
And finally, many of the modelling studies predicting increased incidence of shingles in the elderly pre-date availability of zoster vaccine. So it appears that the continued absence of chickenpox vaccine from the childhood immunisation schedule in Ireland is primarily related to issues around cost.
Conclusion
The public perception of chickenpox is of a relatively benign, inconvenient childhood illness. In many communities, the concept of exposing young children to chickenpox at ‘pox-parties’, in an effort to get infection out of the way early, still exists. However, with increasing awareness of potentially severe complications, increased numbers of immunosuppressed and transplant patients at risk of severe disease, and increasing recognition of the socio-economic consequences of school and parental work absenteeism during illness, this common misconception may be changing.
A safe, highly effective vaccine against chickenpox has been available for over 40 years. In the US, introduction of universal childhood chickenpox vaccination has significantly reduced infection, hospitalisations and mortality caused by chickenpox and its complications in vaccine recipients and in their non-vaccinated contacts.
In addition, if given within three days of exposure to chickenpox, the vaccine has the potential to prevent or reduce severity of infection in non-immune recipients and protect against future exposure. Furthermore, as life expectancy and the incidence of shingles increase, zoster vaccine has the potential to significantly enhance quality of life among the elderly.
References
Gershon AA, Breuer J, Cohen JI, et al. Varicella zoster virus infection. 2017; 1-41
McCarthy K, O Maoldomhnigh C, Butler KM, Gavin PJ. Trends in Hospital Admissions in Ireland due to Primary Varicella Infection: 2005-2016. Press. 2019
Kennedy PGE, Gershon AA. Clinical Features of Varicella-Zoster Virus Infection. Viruses. 2018; 10(11): 1-11
Sauerbrei A, Wutzler P. The congenital varicella syndrome. J Perinatol. 2000; 20(8 Pt 1): 548-54
Ahn KH, Park YJ, Hong SC, et al. Congenital varicella syndrome: A systematic review. J Obstet Gynaecol (Lahore). 2016; 36(5): 563-6
Maheady DC. Reye’s Syndrome: Review and Update. 1989; 246-50
Lesko SM, Brien KLO, Schwartz B, Vezina R, Mitchell AA. Invasive Group A Streptococcal Infection and Nonsteroidal Antiinflammatory Drug Use Among Children With Primary Varicella. 2001; (5)
Health Service Executive National Immunisation Advisory Committee. Immunisation Guidelines of Ireland Chapter 23 Varicella- Zoster. 2015.
Takahashi M. Current status and prospects of live varicella vaccine. 1992; 10(14): 1007-14
World Health Organisation. Varicella and herpes zoster vaccines: WHO position paper. [Internet]. Geneva, Switzerland; 2014. Available from: http://www.who.int/wer/2014/wer8925.pdf?ua=1
European Centre for Disease Prevention and Control. ECDC Guidance - Varicella vaccination in the European Union. 2015. 1-58 p
Health Products Regulation Authority Ireland. VARIVAX powder and solvent for suspension for injection. Varicella Vaccine (live). Information for the user. 2018; Available from: http://www.hpra.ie/docs/default-source/vaccine-pils/varivax.pdf?sfvrsn=18
Merck. HIGHLIGHTS OF PRESCRIBING INFORMATION for VARIVAX®. [Internet]. Vol. 2. 2017. Available from: http://www.merck.com/product/usa/pi_circulars/v/varivax/varivax_pi.pdf
Marin M, Marti M, Kambhampati A, Jeram SM, Seward JF. Global Varicella Vaccine Effectiveness: A Meta-analysis. Pediatrics [Internet]. 2016 Feb 16; Available from: http://pediatrics.aappublications.org/content/early/2016/02/14/peds.2015-3741.abstract
Health Products Regulation Authority Ireland. ZOSTAVAX. Posder and solvent for suspension for injection in a pre-filled syringe. Information for the user. 2017; 91: 399-404
Homma S, Thompson J LP, Pullicino PM, et al. A Vaccine to Prevent Herpes Zoster and Postherpetic Neuralgia in Older Adults. NEnglJMed2. 2012; 366(20): 1859-69
Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352(22):2271-8
World Health Organisation. Varicella and herpes zoster vaccines: WHO position paper. Wkly Epidemiol Rec Relev épidémiologique Hebd [Internet]. 2018; 93(25): 73-96 Available from: http://www.who.int/wer
Varela FH, Pinto LA, Comerlato M. Global impact of varicella vaccination programs. Hum Vaccin Immunother [Internet]. 2018;0(0):1–13. Available from: https://doi.org/10.1080/21645515.2018.1546525
Spoulou V, Alain S, Gabutti G, Giaquinto C, Liese J, Martinon-Torres F. Implementing Universal Varicella Vaccination in Europe. Paediatr Infect Dis J. 2019; 38(2): 181-8
Edmunds WJ, Brisson M. The Effect of Vaccination on the Epidemiology of Varicella Zoster Virus. 2002; 44
McCarthy K, Gavin PJ. Clinically reported cases of Chickenpox & Shingles from the Sentinel GP Network: 2005-2016. Unpublished
 (click to enlarge)
(click to enlarge)