Productivity losses associated with head and neck cancer are a significant component of the burden of illness
Ms Alison Pearce, Postdoctoral Research Fellow, National Cancer Registry Ireland, Cork, Ms Aileen Timmons, Postdoctoral Research Fellow, National Cancer Registry of Ireland, Cork, Dr Paul Walsh, Postdoctoral Research Fellow, National Cancer Registry of Ireland, Cork, Prof Linda Sharp, Professor of Cancer Epidemiology, National Cancer Registry of Ireland, Cork, Mr Paul Hanley, Lecturer in Economics, National College of Ireland, Dublin, Prof Ciaran O'Neill, Professor of Health Economics, National University of Ireland, Galway, Ms Audrey Thomas, Postdoctoral Research Fellow, National University of Ireland, Galway, Ms Eleanor O'Sulllivan, Senior Lecturer in Dental Surgery, Cork University Dental School and Hospital, Cork, Ms Rachel Gooberman-Hill, Reader in Applied Health Research, University of Bristol, Bristol, UK and Prof Pamela Gallagher, Professor of Health Psychology, Dublin City University, Dublin
Head and neck cancer, which encompasses cancers of the mouth, salivary glands, pharynx, nasal cavity/middle ear/sinuses, and larynx, is diagnosed in over 570 individuals in Ireland annually.1 While traditionally a cancer of older men, the emergence of human papilloma virus (HPV)-related cancers of the head and neck have markedly changed incidence patterns.2,3 HPV-related head and neck cancer occurs primarily among younger (40-59 years) non-smokers from higher socio-economic groups,3 resulting in head and neck cancer becoming increasingly common in those of working age. Similar to other cancers, most people diagnosed with head and neck cancer who are working at the time of diagnosis are likely to take some time out of the workforce for treatment (surgery, radiotherapy or chemotherapy), recuperation and rehabilitation.4,5
Measuring productivity losses
In addition to impacting on the individual’s identity6 and quality of life,7 time away from the workplace as a result of cancer has implications both for the employer and for society as a whole in the form of productivity losses. Estimates of productivity losses can contribute to decision making from a cost of illness perspective, and to economic evaluations of new drugs, devices and services within a healthcare system.
The traditional approach to estimating productivity losses in health economics has been the human capital approach (HCA), which sees individuals as potentially producing a stream of output over a working life.8,9 HCA measures lost productivity as the time the working life is shortened by due to illness, valued at the market wage.
An alternative to the HCA is the friction cost approach (FCA), which takes into account that absent workers are usually replaced within the workplace.10 Lost productivity is limited to the time taken to replace the worker (the so called ‘friction period’), again valued at the market wage. The choice of method for calculating productivity losses remains under debate.11
A small number of previous studies report productivity losses associated with head and neck cancer.3,12,13,14 They suggest losses due to premature mortality are higher for head and neck cancer than other types of cancer12 and that socio-demographic and clinical factors such as age, gender and cancer site may contribute to lost productivity.13 However, these studies only included losses due to a single aspect of productivity, such as absenteeism14 or premature mortality,12,13 and only used the HCA. This analysis aimed to estimate the cost of lost productivity due to different types of absenteeism and premature mortality associated with head and neck cancer using both the HCA and FCA.
Methods
To estimate productivity costs using the HCA and FCA, survey data of workforce participation prior to and following head and neck cancer diagnosis was combined with population level survival data and national economic data. Four types of productivity loss were calculated:
Temporary time off work (TTO): individuals who take time off work after diagnosis, but then return to work
Permanent time off work (PTO): individuals who cease working as a result of their diagnosis
Reduced hours at work (RHW): individuals who continue working after their diagnosis (with or without a period of TTO) but work fewer hours than before diagnosis
Premature mortality (PM): projected ‘excess’ years of life lost (to age 65) for every individual – excluding background mortality losses.
For the survey, a population-based sample of head and neck cancer (ICD-10 codes C00-C14 or C32) survivors diagnosed during 1994-2008 was selected from the National Cancer Registry Ireland (NCRI). Ethical approval was provided by the research ethics committee for each of the 14 participating public and private hospitals around Ireland. A total of 991 survivors were sent the survey between August and October 2012. In addition to demographic and clinical information, questions were included on employment status at diagnosis, occupation at diagnosis, weekly hours worked, and time taken off work following diagnosis.
For the FCA, the friction period was assigned based on average Irish vacancy rates by occupation type.15 Professional occupations were assumed to have a friction period of 13.3 weeks, service occupations had a friction period of 9.9 weeks, and manual occupations had a friction period of 10.1 weeks.15
NCRI population-level survival data (available on request) for all head and neck cancer types and stages combined and Irish life table data16 were used to estimate premature mortality.17,18
Results
A total of 251 eligible survey respondents who were both of working age and employed or self-employed at the time of diagnosis were included in the analysis.
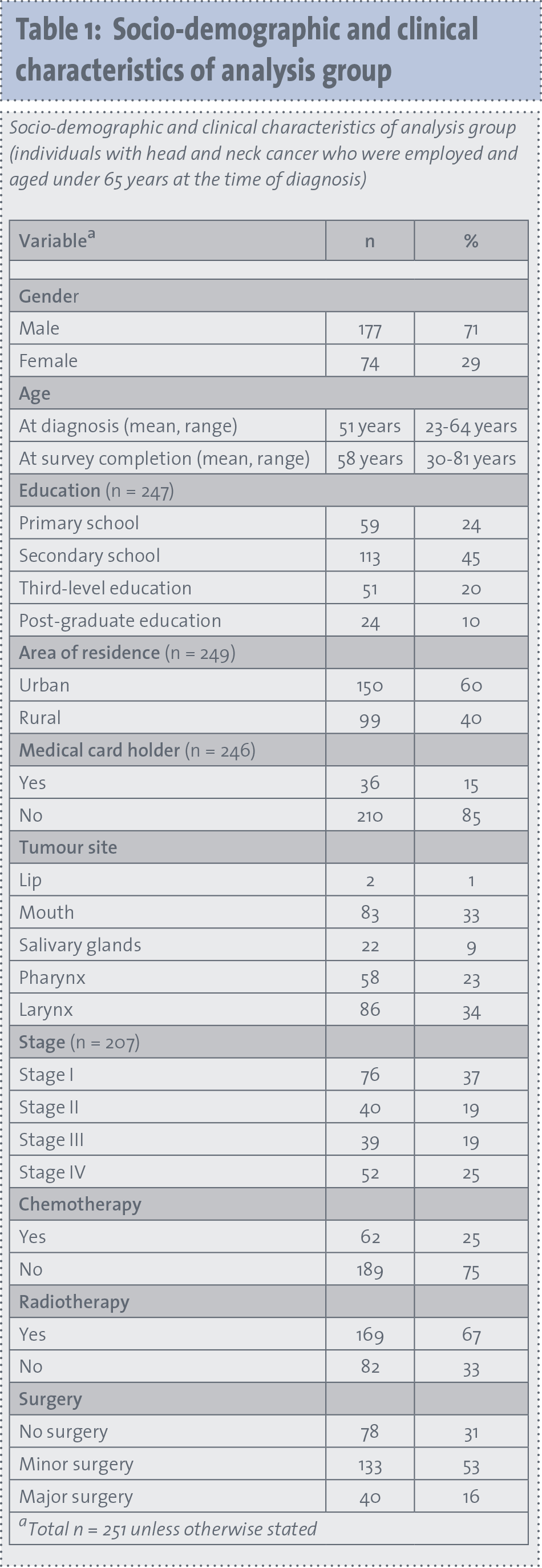
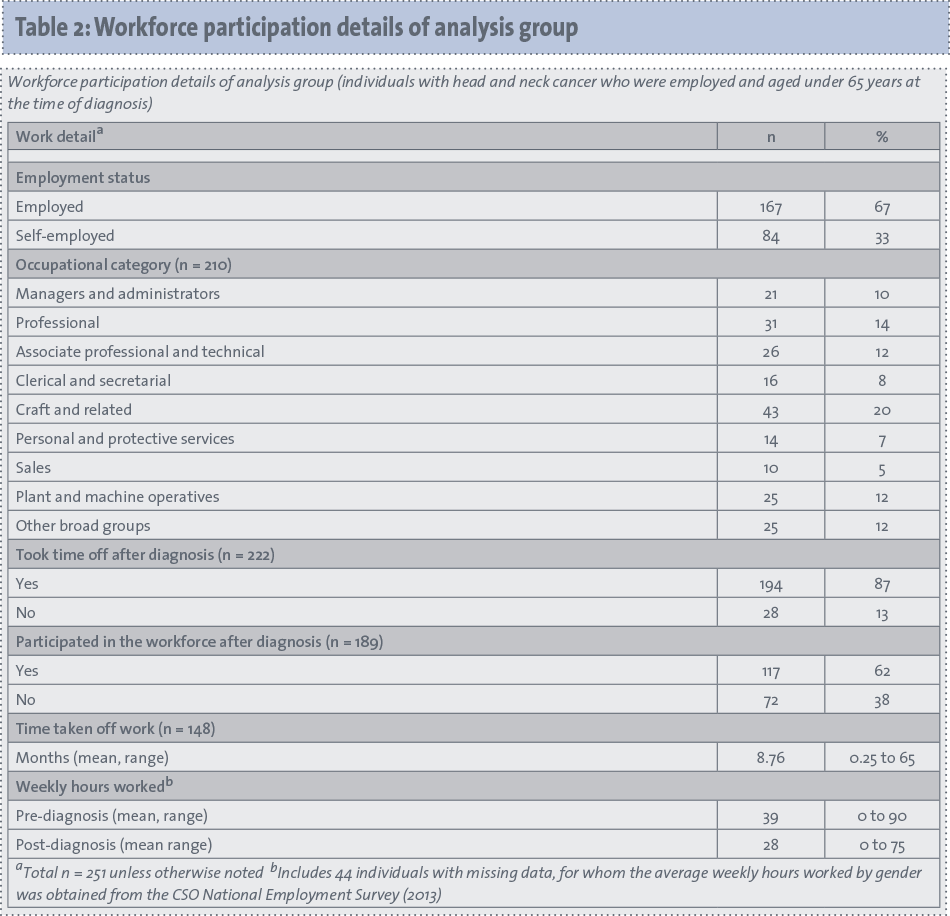
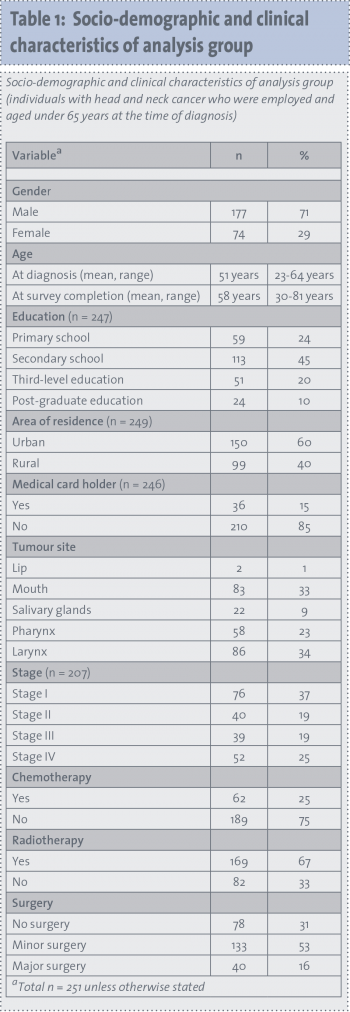
Socio-demographics, clinical and work details of analysis group
Table 1 presents the socio-demographic and clinical characteristics of the analysis sample and Table 2 their working arrangements. The mean age at diagnosis was 51 years and 71% of subjects were male. Seventy-seven percent of the sample reported taking time off work, with 30% not returning to the workforce by the time of the survey. The average pre-diagnosis working hours were 39 per week, and one-third of participants were self-employed.
(click to enlarge)
(click to enlarge)
Productivity losses
Table 3 shows the average total productivity losses calculated using the HCA and FCA. Average total productivity losses for head and neck cancer were estimated to be €253,800 per person working at the time of diagnosis with HCA and €6,800 per person working at the time of diagnosis with FCA. The FCA estimate is approximately 3% of the HCA estimate. The main driver of cost using the HCA was premature mortality (which accounted for 38% of the total cost), while using the FCA it was temporary time off (73% of the total cost).
(click to enlarge)
Productivity losses by socio-demographic and clinical factors
Regardless of approach, productivity losses were higher for males, those with higher education and those with professional occupations, driven by the higher wages in these groups. Using the HCA, younger individuals had much higher productivity losses than older individuals due to the longer time period of lost productivity. For clinical subgroups, both approaches found that those with pharyngeal cancer, more advanced disease and who received chemotherapy had higher productivity losses.
Sensitivity analysis
While the sensitivity analysis resulted in a range of HCA estimates from €197,952 to €519,332, and a range of FCA estimates of €5,843 to €8,119, it did not impact on the distribution of productivity cost components for either approach.
Discussion
This is the first study estimating the lost productivity costs associated with head and neck cancer using both the HCA (€253,800 per person working at the time of diagnosis) and FCA (€6,800 per person working at the time of diagnosis). It is also the first study to estimate the productivity losses associated with different aspects of workforce absenteeism (TTO, PTO, RHW), as well as premature mortality (PM) for head and neck cancer.
Comparison of results to previous work
Comparisons to previous studies of productivity losses in head and neck cancer are difficult, due to the differing methodologies used.
The FCA estimates of total head and neck cancer costs in this study are similar to, although somewhat lower than, estimates for other cancer sites (eg. €8,103 in breast cancer, €8,205 in prostate cancer17), primarily driven by the limited period during which costs are accrued. However, the magnitude of the HCA estimates for head and neck cancer (€253,800) are higher than those for breast (€193,400),17 prostate (€109,100)17 and colorectal (€205,800)18 cancers in the same setting. In particular, permanent time off costs were at least twice as high in head and neck cancer (€68,600) as in the other cancers (which ranged from €24,400 in colorectal cancer18 to €34,700 in prostate cancer17), driven by the substantially higher proportion of individuals who depart the workforce permanently following head and neck cancer (30% compared to 13% in breast cancer and 12% in prostate cancer).17 These higher numbers may be due to the increased morbidity associated with head and neck cancer and its treatments compared to other cancers.19
Using the human capital and friction cost approaches in economic evaluation
While productivity loss estimates have, for a long time, contributed to cost of illness estimates, they are increasingly being included in economic evaluations. One of the primary purposes of economic evaluations is to determine the reimbursement of new drugs and devices within a health care system.
The HCA takes a societal, and therefore more comprehensive, approach17,20 by measuring ‘potential’ losses to society. This results in estimates of the maximum of possible production lost.17 It is thus appropriate when conducting an economic evaluation from a societal perspective,11 and the well-established methods with relatively accessible data means it is comparatively easy to apply.
In contrast, the FCA is said to more accurately estimate the ‘actual’ or lower bound of lost production,17 by allowing for co-workers to compensate for some lost production, and unemployed individuals to replace lost workers.17 This approach is more consistent with an employer’s perspective, which is particularly relevant in healthcare systems where employers pay for at least part of employee health insurance.20
Drivers of differences between approaches
As seen in other studies,17,21 this analysis found the key driver of productivity losses with HCA was age, while the FCA was driven by wage differences. The HCA results in particularly high values of lost production for younger individuals who cease working, whereas age has less of an impact of FCA estimates. The equity implications of using wages to value production have been well documented,22 with concern that highly paid individuals will have their health gains valued more highly.
Similar issues apply with the FCA, where individuals with lower salaries tend to be easier to replace, and thus have shorter friction periods and correspondingly lower productivity losses. This highlights the ethical concerns around subgroup analysis in productivity analyses.
Diseases with longer-term impacts, such as cancer, are likely to have greater differences between the HCA and FCA than short-term illnesses such as influenza. The results of this study highlight the importance of health economists and policy makers being aware of the assumptions underpinning estimates of lost productivity.
Conclusion
Productivity losses associated with head and neck cancer are a significant component of the burden of illness. Individuals with pharyngeal cancer, more advanced disease and who received chemotherapy had greater productivity losses. Using the HCA and FCA approach to estimate productivity costs provides decision makers with information concerning the differences in costs derived according to each approach and the key drivers of costs, which change according to the method applied.
A pragmatic approach for future research may be to use both HCA and FCA to estimate productivity losses associated with cancer.
References
National Cancer Registry Ireland, Cancers of the head and neck. Cancer Trends No. 10. National Cancer Registry Ireland: Cork, 2011.
Adelstein DJ et al. Head and neck squamous cell cancer and the human papillomavirus: summary of a National Cancer Institute State of the Science Meeting, November 9-10, 2008, Washington, DC. Head and Neck 2009; 31(11): 1393-1422.
Coughlan D, Frick KD. Economic impact of human papillomavirus-associated head and neck cancers in the United States. Otolaryngology Clin North Am 2012; 45: 899-917.
Verdonck-de Leeuw IM et al. Employment and return to work in head and neck cancer survivors. Oral Oncology 2010; 46: 56-60.
Pearce A et al. Long-term workforce participation patterns following head and neck cancer. J Cancer Survivorship 2014: 1-10.
Syse A, Tretli S, Kravdal O. Cancer’s impact on employment and earnings – a population-based study from Norway. J Cancer Survivorship 2008; 2: 149-158.
Ramirez MJF et al. Psychosocial adjustment in patients surgically treated for laryngeal cancer. Otolaryngol Head Neck Surg 2003; 129: 92-7.
Weisbrod B. Economics of Public Health. Philadelphia: University of Pannsylvania Press, 1961.
Cooper BS, Rice DP. The economic cost of illness revisited. Social Security Bull 1976; 39: 21-36.
Koopmanschap MA et al. The friction cost method for measuring indirect costs of disease. J Health Econ 1995; 14: 171-189.
Knies S et al. The transferability of valuing lost productivity across jurisdictions. Differences between national pharmacoeconomic guidelines. Value in health. J Int Soc for Pharmacoeconomics Outcomes Res 2010; 13(5): 519-527.
Ekwueme DU et al. Years of potential life lost and productivity costs because of cancer mortality and for specific cancer sites where Human Papillomavirus may be a risk factor for carcinogenesis – United States, 20013. Cancer 2008; 113(10 suppl): 2936-45.
Bradley CJ et al. Productivity costs of cancer mortality in the United States: 2000-2020. J Nat Cancer Inst 2008: 1763+.
Borget I, Abramowitz L, Mathevet P. Economic burden of HPV-related cancers in France. Vaccine 2011; 29(32): 5245-5249.
Hanly P, Koopmanschap MA, Sharp L. The friction cost approach in a changing macroeconomic environment: The case of colorectal cancer productivity costs. TBC, Draft.
Central Statistics Office, Irish Life Tables No. 15, 2005-2007. Central Statistics Office: Dublin, 2009.
Hanly P et al. Breast and prostate cancer productivity costs: a comparison of the human capital approach and the friction cost approach. Value Health 2012; 15(3): 429-36.
Hanly P et al. Work-related productivity losses in an era of ageing populations: the case of colorectal cancer. J Occup Environ Med 2013; 55(2): 128-34.
Penner JL. Psychosocial care of patients with head and neck cancer. Sem Oncol Nursing 2009; 25(3): 231-241.
Lensberg BR et al. Challenges in measuring and valuing productivity costs, and their relevance in mood disorders. ClinicoEconom Outcomes Res 2013; 5: 565-573.
Tranmer JE et al. Valuing patient and caregiver time: A review of the literature. PharmacoEconomics 2005; 23(5): 449-459.
Williams A. Cost-effectiveness analysis: is it ethical? J Med Ethics 1992; 18: 7-11.
 (click to enlarge)
(click to enlarge)