An examination on whether an educational intervention is effective in reducing pre-hospital delay times for acute coronary syndrome patients
Ms Mary Mooney, Lecturer, School of Nursing and Midwifery, Trinity College Dublin, Ms Gabrielle McKee, Lecturer, School of Nursing and Midwifery, Trinity College, Dublin and Ms Frances O'Brien, Lecturer, School of Nursing and Midwifery, Trinity College, Dublin
Acute coronary syndrome (ACS) includes unstable angina and the two categories of myocardial infarction (MI); ST elevated and non-ST elevated MI.1 These conditions are associated with reduced coronary perfusion, thereby indicating the importance of early diagnosis and risk stratification to guide management and improve short and long-term outcomes.2,3,4
While time is of less importance for those with unstable angina and non-ST elevated MI (NSTEMI) than those with ST-segment elevation MI (STEMI), coronary ischaemic time should be kept to a minimum in all cases.5,6 In the presence of ACS, patient delay contributes most significantly to delayed admission to the emergency department (ED).7,8
In light of this, using a randomised controlled trial, this study tested whether an individualised educational intervention would be effective in reducing patient pre-hospital delay time among patients who were re-admitted to an ED with ACS symptoms. Pre-hospital delay time refers to the time from ACS symptom onset until arrival at the ED.9,10
Patients were recruited to the study from the coronary care units and cardiology wards of five large tertiary hospitals in Dublin. The study was ethically approved by each hospital’s ethics committee. The gatekeepers for the study were the clinical nurse managers and staff nurses in the clinical areas. They screened the patients for eligibility and gave their names to the research nurse who met the patients and informed them about the study before seeking informed consent. Enrolment to the study was generally within two to four days of hospital admission.
Patients were randomly assigned to the control or intervention groups. This was determined by their study numbers, which were generated using a computerised system. Using the ACS response index,11 baseline data were collected. Those assigned to the intervention group received a 30-40 minute educational intervention that focused on reducing patient pre-hospital delay time.
Unlike previous research studies, all patients recruited to this study were admitted via an ED with an ACS diagnosis. Pre-hospital delay time was measured on admission (baseline), and again for all patients on their first subsequent readmission with ACS symptoms, within two years of recruitment to the study.
The control and intervention groups received usual in-hospital care from their healthcare provider. It is worth noting that usual care did not appear to be standardised within or between the research sites. Pre-discharge patient education broadly comprised information about medications, modifiable risk factors and advice about lifestyle adjustments. None of the sites delivered extensive information that focused on pre-hospital delay or the factors that influence it.
The intervention content
The aim of the intervention was to reduce patient pre-hospital delay time. Most of the emphasis was on patient-decision delay, which accounts for up to 75% of pre-hospital delay time.12
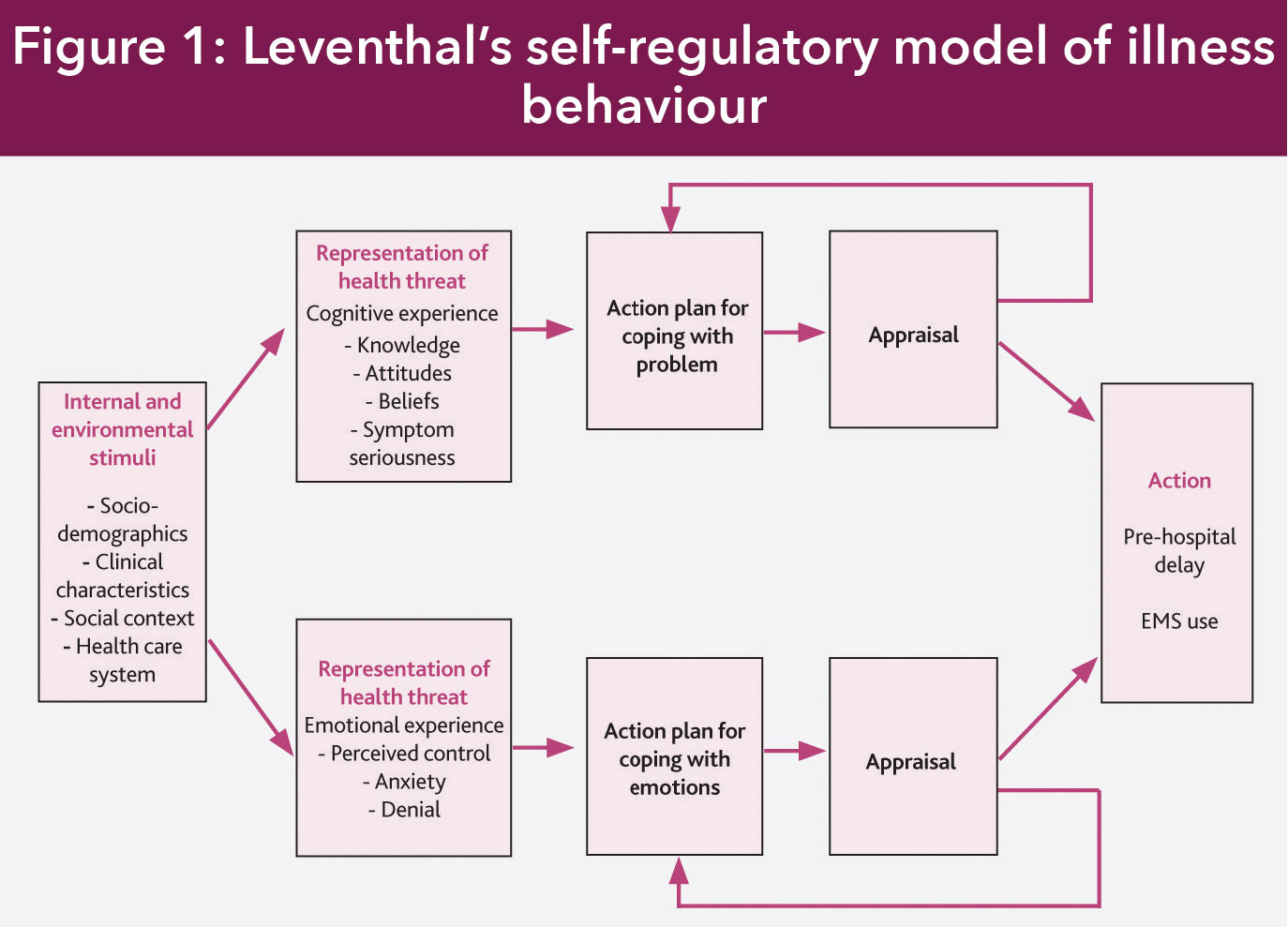
The session was prefaced with a reminder about the purpose and aim of the study. The educational intervention was underpinned by Leventhal’s self-regulatory model of illness behaviour (see Figure 1).13,14
(click to enlarge)
This model advocates that the onset of symptoms triggers an individual to make behaviour adaptations. These adaptations occur in three stages that are processed cognitively (problem-solving) and emotionally and are influenced by internal and environmental stimuli. Internal stimuli include sociodemographic factors, such as age, while environmental stimuli include messages from family or friends.
The intervention addressed informational, emotional and social factors as these are the variables that are known to influence pre-hospital delay time. These three factors mirror Leventhal’s cognitive, emotional and environmental components of the self-regulatory model of illness behaviour.
Information or cognitive stage
Using the intervention manual that was devised for the study, the education began with a simplified explanation about atherosclerosis and the mechanism by which a heart attack occurs.
The concept of the golden hour was then explained to patients. The golden hour refers to one hour of golden opportunity to receive optimum care that could save a life or prevent worsening disability when a heart attack occurs.
The benefits of prompt hospitalisation in the presence of heart attack symptoms were outlined. This included reference to the importance of early reperfusion to restore blood flow to the myocardium and the other therapeutic options that are available for the treatment of a heart attack. Patients were also informed that many people miss out on the best possible outcomes because they delay too long before seeking care.
The next informational message was centred on symptoms. The range and variability of symptoms were discussed. Typical ACS symptoms such as chest pain, tightness and discomfort were highlighted together with left arm discomfort, indigestion and breathlessness. Less typical symptoms were also emphasised and these include gum, neck and jaw discomfort, intrascapular discomfort and nausea. Patients were informed that symptom onset could be sudden or gradual and that they could be continuous or intermittent.
They were made aware that the ‘Hollywood heart attack’ was only one of a range of manifestations of a heart attack or ACS symptoms. It was made clear that ACS symptoms are not individualised and that symptoms that are experienced on one occasion may differ on a subsequent occasion.
They were informed about the potential for symptom variation among different groups, such as older people and those with diabetes. However, this aspect of the informational message was tailored to each patient and their circumstances.
Patients were then reminded that their current ACS diagnosis rendered them more susceptible to a future ACS event than those without a history of ACS. They were instructed that the appropriate behaviour to take in the event of symptom occurrence was to stop and rest in the presence of symptoms, and if nitrates were prescribed, to use them. They should also inform another person about the symptoms and if they persisted beyond 15 minutes, they were asked to call 999 or 112 for an ambulance without summoning the advice of a GP.
Emotional issues
In addressing emotional issues, advice was given about the role of emotions when ACS symptoms are present. It was acknowledged that emotional responses could interfere with symptom identification, acknowledgement and coping.
The potential for emotions such as fear, denial, anxiety and embarrassment to interfere with treatment-seeking behaviour was discussed.
Patients were advised that people often fear the consequences of acknowledging their symptoms. Consequently, they may deny the seriousness of symptoms or engage in symptom misattribution, which can delay the time in seeking treatment.
The reasons for delay were discussed objectively. The objective discussion avoided blame-focused messages or implications of wrong-doing by the patient. Much of this discussion took place in the first person plural. One example of this was with respect to the role of anxiety in patient pre-hospital delay. The words used to explain this were as follows: ‘anxiety can cause us to think less clearly and make excuses about what is happening…’ and ‘fear causes many people to delay seeking care’. These words indicate that delay-related responses were not isolated to the patient, but could be applied generally to individuals with ACS symptoms.
Scenarios and role play were used to re-enact a recurrence of an ACS event. This was to increase the likelihood of appropriate future reactions, to challenge emotional responses to symptoms and to reinforce the intervention message. Patients were encouraged to treat unresolved ACS symptoms as an emergency. This was important, as behaviour in threatened-health is dependent on how the individual views that threat.13
Previous ED admission experiences were discussed, as negative experiences could impact on the person’s willingness to return to the ED in future. Unpleasant past experiences were acknowledged, but these were reconciled with the intervention message that the beneficial rewards of seeking treatment promptly would outweigh everything else.
Positive messages were disseminated, such as early attendance at the ED would enhance preservation of heart muscle and increase the chance of survival. This was considered important, as positive messages are considered potentially more effective.15
While addressing emotional stimuli, the patient was asked to consider what they would do if they thought they were having a heart attack. A range of reactions were suggested, including adopting the stance that the symptoms were not heart related or not serious.
Further suggestions included emotional issues, such as concern about troubling others and embarrassment about seeking help for something that may transpire to be clinically insignificant. It was anticipated that normal reactions would be identified so that these could be acknowledged, addressed and set aside with a view to addressing self-care needs.
In the final ten minutes of the intervention, and to further address the role of emotional responses to a health threat, patients were given pre-prepared scenarios to consider. The scenarios that were most reflective of the patient’s cardiac event experience were chosen from the range of scenarios available. Based on these, and using role play, patients were asked to anticipate some or preferably all of the emotions they might experience in the presence of ACS symptoms.
It was considered that the rehearsal of responses using role play would improve patients’ levels of perceived control on a subsequent occasion. It has been suggested that anxiety levels reduce if a person is confident in their ability to act appropriately.16 Furthermore, even when experiencing emotional reactions to symptoms, the use of guidance on the appropriate actions to take increases the likelihood of appropriate responses to a future health threat.17
Social and environmental stimuli
As part of the intervention, patients were informed that family and friends can delay them seeking care, as they may wish to deny the possibility of symptoms. The importance of avoiding consultation with a GP was discussed in the context of social stimuli. The misunderstanding by individuals that it is correct to summon the advice of a GP in the presence of ACS was clarified.
Patients then completed an action plan, which they were given to take home as a reminder of what to do if symptoms arose. This action plan included the name and phone number of the person they would call if symptoms occurred and the emergency numbers to call in the face of unresolved symptoms. A pre-printed wallet card with a summary of what to do in the presence of ACS symptoms was also given. The intervention was reinforced by telephone one month after the intervention was delivered and six months later, by post. Motivational interviewing techniques were used to promote the uptake of the intervention and to help patients reconcile elements of the intervention that they found challenging.
At the end of the education session, the information was summarised together with the correct course of action to be taken in the event of symptom recurrence. This included the following message:
In the event of symptoms you should:
• Stop and rest
• If nitrates are prescribed, take these as directed
• Inform somebody about what is happening
• If symptoms persist for more than 15 minutes then call directly for an ambulance.
The research nurses used pre-printed flip charts and prescriptive scripts as educational aids. The educational intervention was individualised to the patient’s specific needs and illness experiences and sought to address the range of potential cognitive, social and emotional effects that the person with ACS symptoms may have experienced.
The effect of intervention
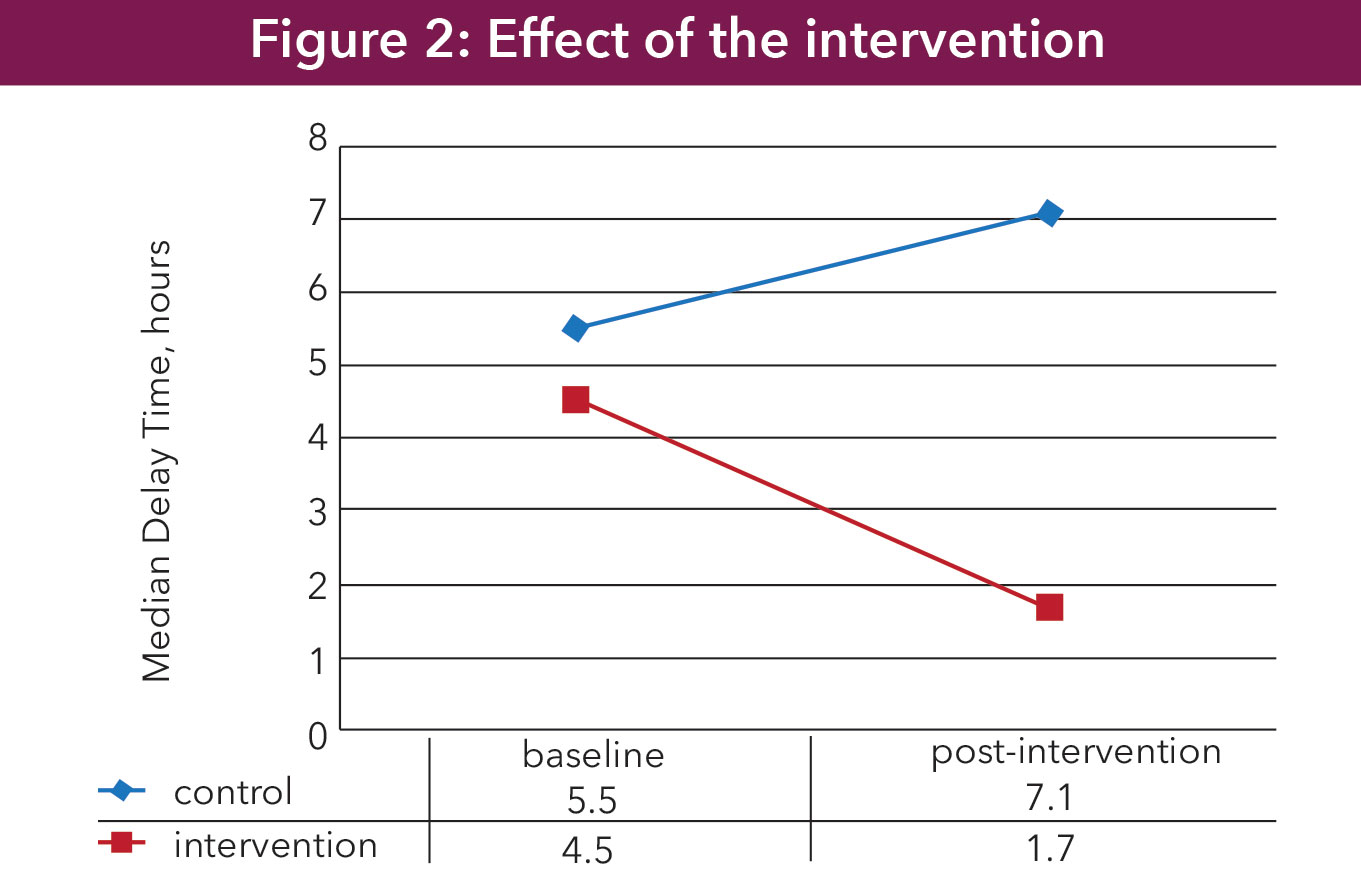
The intervention was effective in reducing pre-hospital delay time among the intervention group. Among this group, the median pre-hospital delay time was reduced from 4.5 hours (at baseline) to 1.7 hours [25th percentile 1.1, 75th percentile 2.9] (see Figure 2).
(click to enlarge)
The post-intervention median pre-hospital delay time for the control group increased from 5.5 hours (at baseline) to 7.1 hours [25th percentile 2.7, 75th percentile 16.7]. These post-intervention readmission pre-hospital delay times represent an increase of 1.6 hours in the control group and a reduction of 2.8 hours in the intervention group, with a difference of 5.4 hours between the groups. The intervention was therefore very effective in reducing pre-hospital delay time.
From a European perspective, this was the first RCT to target a reduction in patient pre-hospital delay time. Furthermore, it was the first RCT in the world to be effective in this regard. Therefore, this study represents a major contribution to the body of existing knowledge about pre-hospital delay time. It could also pave the way for changes to nursing practice with respect to the content and delivery of usual pre-discharge education for patients with ACS.
This article was previously published in the Journal of Emergency Medicine
Acknowledgement
This study was funded by the Health Research Board of Ireland
References
Anderson JL, Adams CD, Antman EM et al. ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction). Developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007; 50(7): 1-157
Fox K, Dabbous O, Goldberg RJ et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). Br Med J. 2006; 333: 1091-1106
Granger C, Goldberg RJ, Dabbous O et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003; 163: 2345-2353
Karras C, Donlan S, Aitchison R, Aitchison P, Wang E, Kharasch M. Acute coronary syndromes. Disease a Month. 2013; 59: 202-209
Hamm CW, Bassand JP, Agewall S et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2011; 32(23): 2999-3054
Bassand JP, Hamm CW, Ardissino D et al. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: The Task Force for the Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of the European Society of Cardiology. Eur Heart J. 2007; 28(13): 1598-1660
Tubaro M, Danchin N, Goldstein P et al. Pre-hospital treatment of STEMI patients. A scientific statement of the Working Group Acute Cardiac Care of the European Society of Cardiology: Acute Coronary Syndromes. Acute Card Care. 2011; 13(2): 56-67
Garofalo D, Grey C, Lee M, Exeter D, Kerr AJ. Pre-hospital delay in acute coronary syndromes: PREDICT CVD-18. N Z Med J. 2012; 125: 12-22
Dracup K, McKinley S, Riegel B et al. A nursing intervention to reduce pre-hospital delay in acute coronary syndrome: a randomised clinical trial. The Journal of Cardiovascular Nursing. 2006; 21(3): 186-193
McKee G, Mooney M, O’ Donnell S et al. Multivariate analysis of predictors of pre-hospital delay in acute coronary syndrome. Int J Cardiol. 2013
Riegel B, McKinley S, Moser DK et al. Psychometric evaluation of the Acute Coronary Syndrome (ACS) response index. Res Nurs Health. 2007; 30(6): 584-594
Rasmussen CH, Munck AM, Kragstrup JK, Haghfelt TH. Patient delay from onset of chest pain suggesting acute coronary syndrome to hospital admission. Scand Cardiovasc J. 2003; 37(4): 183-186
Leventhal H, Cameron L. Behavioral theories and the problem of compliance. Patient Educ Couns. 1987; 10: 117-138
Leventhal H, Safer M, Panagis D. The impact of communications on the self-regulation of health beliefs, decisions and behaviour. Health Educ Q. 1983; 10(1): 3-29
Dracup K, McKinley SM, Moser DK. Australian patients’ delay in response to heart attack symptoms. Med J Aust. 1997; 166(5): 233-236
Moser DK, Riegel B, McKinley S et al. Impact of anxiety and perceived control on in-hospital complications after acute myocardial infarction. Psychosom Med. 2007; 69(1): 10-16
Leventhal H, Breland JY, Mora PA, Leventhal EA. Lay representations of illness and treatment: a framework for action. Handbook of Behavioral Medicine: Springer; 2010; 137-54.
 (click to enlarge)
(click to enlarge)