CANCER
Rehabilitation needs in brain tumour patients
Research evidence to support implementation
April 1, 2024
-
More than 300,000 brain and central nervous system tumours were diagnosed worldwide in 2020.1 In Ireland, around 480 people are diagnosed with primary brain tumours every year.2 Brain tumours are a heterogeneous group of conditions, varying in location, histopathology and molecular features.3 Astrocytic tumours, primarily high-grade glioblastomas, form the majority of malignant brain cancers.2
Brain tumours can shorten life span and cause neurological impairment, resulting in functional limitations. There may be significant symptom burden associated with brain tumours which can frequently present in clusters and increase in severity as the disease progresses.4 Symptoms may include physical, cognitive and neuropsychological sequelae, and fatigue.5,6 Such symptoms can have profound effects on the lives of those living with and beyond brain tumours, and their families.7,8,9,10
Therapies, such as physiotherapy and occupational therapy, are often used in rehabilitation settings to help maximise functioning and regain independence. However, due to variations in disease course and fluctuations in neurological presentation, people with brain tumours often experience unmet needs and report difficulties in accessing rehabilitation services.11 Specific issues related to the rehabilitation needs of people with neurological conditions in Ireland include long waiting lists, limited access to specialist rehabilitation services and a shortage of community-based specialist rehabilitation and support services.12
Despite the complexity of presentation and disease course, research has shown that the functional limitations imposed by brain tumours are amenable to rehabilitation just like other neurological conditions.13 Therefore, it is important to understand rehabilitation needs for those with brain tumours with a view to improving their experiences and outcomes.
Background to the research
The biological characteristics of brain tumours mean they can be challenging to treat and often resistant to conventional and novel treatments.14 These challenges are exacerbated by the relatively low incidence of brain tumours in most populations, and limited engagement from the pharmaceutical sector and research community on innovation approaches to management. Poor prognosis, changes in daily functioning after treatments and loss of independence can affect those with brain tumours and significantly impact cancer survivorship, particularly health-related quality-of-life (HRQoL).15
Rehabilitation
The goal of rehabilitation is to help maximise an individual’s functional independence and quality of life post-intervention. Rehabilitation care for those with brain tumours requires multidisciplinary teams to address the range of symptoms and treatment side-effects. Multidisciplinary rehabilitation generally involves many healthcare professionals (HCPs) – rehabilitation medicine physicians, physiotherapists, occupational therapists, psychologists, social workers, nurses, speech and language therapists, dietitians and palliative care specialists.
Rehabilitative measures have proven beneficial for cancer patients across inpatient and outpatient rehabilitation settings. Several studies have highlighted the benefits of rehabilitation for those with brain tumour.13,16,17,18 Significant disability, caused by the brain tumour, was found to be responsive to multidisciplinary rehabilitation and rehabilitation has been shown to improve motor/cognitive functional prognosis and quality of life.13,18 However, brain tumours present specific rehabilitation challenges – treatment of the primary neuromuscular pathology as well as complex symptom presentation.19
Research in those with gliomas assessed the effectiveness of physical and occupational rehabilitation, involving cardiovascular training, resistance training and individually designed interventions. It demonstrated significant improvements in aerobic power and lower and upper limb strength.9 Despite these findings, research evidence supporting brain tumour rehabilitation generally focuses on patients with glioma and is not well established or implemented.18,20 The reasons for this are unclear but may relate to uncertainty about tumour prognosis, the implications for rehabilitation on the timing and side-effects of treatments such as radiotherapy and chemotherapy, and the resourcing of specialist rehabilitation services.
The European Association for Neuro-Oncology and the National Institute of Clinical Excellence (NICE) has several recommendations regarding care of those with brain tumours. These include engagement with rehabilitation during treatment and follow-up; providing information to people with brain tumours, their families, carers on rehabilitation options (community based, outpatient/inpatient); information on accessing rehabilitation assessments; allocated central points of contact; including carers in medical consultations.21,22
Despite this advice, clinical practice guidelines related to rehabilitation are unclear and currently best practice is not defined.9 It has been acknowledged nationally that developments in community neuro-rehabilitation have not kept pace with developments in the acute care setting and there is a widening gap between demand and capacity for specialist rehabilitation services in Ireland.12
A national steering group was established in 2017 to develop and implement a National Implementation Framework for neuro-rehabilitation services in Ireland. A key part of this framework focuses on the development of a range of services – acute rehabilitation, complex specialist rehabilitation services (in the NRH), post-acute inpatient specialist rehabilitation services and community specialist neuro-rehabilitation services.12
Acute neuro-rehabilitation is provided within the acute hospital setting as early as possible by a consultant-led interdisciplinary team. Complex specialist rehabilitation (such as the National Rehabilitation Hospital [NRH]) services provide a higher level of specialist expertise, facilities, and programme intensity to highly complex rehabilitation needs. Post-acute inpatient specialist rehabilitation is delivered in an inpatient and/or ambulatory setting by a specialist interdisciplinary team led by a rehabilitation medicine consultant.
Community-based specialist rehabilitation teams should provide multidisciplinary rehabilitation; preferably with case managers; to those with stable complex needs. A range of specialist community-based services to meet ongoing and longer-term neuro-rehabilitation needs is also required. In addition, many voluntary organisations complement specialist rehabilitation services with a range of supports to integrate people with neurological disability in the community.12
Multidisciplinary healthcare teams that deliver tailored care in both inpatient and outpatient settings are central to the rehabilitation of those with brain tumours. However, studies of multidisciplinary rehabilitation have had mixed findings – low level evidence for higher intensity inpatient rehabilitation compared to standard outpatient care18; functional and cognitive improvements at the end of intervention.20,23,24
While outpatient therapy has been less studied there was evidence of functional gains among people with brain tumours in an interdisciplinary outpatient rehabilitation programme.25 A better understanding of the effectiveness of multidisciplinary rehabilitation at different stages of the treatment/recovery trajectory is needed. This should include information on the optimal structure, function, timing, setting and content of beneficial rehabilitation interventions.
The construct of ‘rehabilitation potential’ is a commonly cited consideration in determining suitability for rehabilitation services. Rehabilitation potential is the clinical prediction of a patient’s anticipated improvement with rehabilitation interventions.26 It exists on a continuum, can change over time, and is based on patient characteristics and the local healthcare environment.26 A perceived ‘lack of rehabilitation potential’ can be used to exclude patients from rehabilitation services.27
However, a considerable amount of information other than functional outcomes is needed to evaluate potential benefits. There is little evidence to support who will benefit most from rehabilitation in terms of improvements in function and HRQoL. The World Health Organization (WHO) recommends a broader consideration of rehabilitation, defined as “a set of interventions designed to optimise functioning and reduce disability in individuals with health conditions in interaction with their environment”.28 The use of rehabilitation potential as a judgment to limit access to rehabilitation, is considered invalid.27
In the Irish context, those with brain tumours are not excluded from accessing neuro-rehabilitation. However, as the numbers of brain tumours is relatively small in relation to all cancers, individuals may not be prioritised in existing models of care and services with limited resources.
Brain-Restore project
The Brain-Restore project is funded by Health Research Charities Ireland, the Health Research Board and Breakthrough Cancer. Our aim is to increase understanding of the rehabilitation needs of patients with brain tumours in Ireland towards improved care. Those with brain tumours generally experience a continuum of rehabilitation care and the project is designed to reflect this trajectory. It also includes an action-research approach to gather information from key stakeholders and involves four interlinked studies:
• Study 1. A scoping review to determine the scope of current evidence on rehabilitation needs. The study objectives are to:
– Determine the extent and scope of current evidence on rehabilitation needs in people with brain tumours
– Chart the landscape of the types and range of interventions (physical and cognitive) for people with brain tumours, and
– Identify gaps in the literature for future research.
• Study 2. A survey with HCPs involved in the care and rehabilitation of people with brain tumours. The study objective is to conduct a cross-sectional survey with HCPs on rehabilitation needs and assessment of current rehabilitation services.
• Study 3. An epidemiological study - using existing databases – to characterise brain tumours in Ireland. The study objectives are to:
– Epidemiologically profile brain tumour survivors in Ireland and
– Increase understanding of the severity and complexity of symptom burden.
• Study 4. A longitudinal mixed methods study with embedded action research composed of:
– A prospective cohort study to measure the evolution of rehabilitation needs with quantitative patient-reported outcome measures over one-year period and
– An embedded qualitative study to capture the experiences of those with brain tumour and their carers.
The study objectives are to:
– Measure physical, cognitive and social impacts of a brain tumour on patients and family over the first year of diagnosis
– Explore patient and family lived experience of rehabilitation need/services
– Use an action research approach to identify potential changes to current practice to improve patient outcomes; and
– Integrate study findings with the other studies and disseminate to key stakeholders, including brain tumour survivors, their families, HCPs and policy makers.
Action Research – a strategy for implementing change
Action research studies in a range of healthcare contexts have become increasingly common in the past 20 years. The primary goal for action research is to address issues by bringing about change in particular situations, local systems and real-world environments.29 Change is achieved by taking action in a particular system; in response to specific forces. As a result knowledge is created about that action which can be used by other healthcare organisations.30
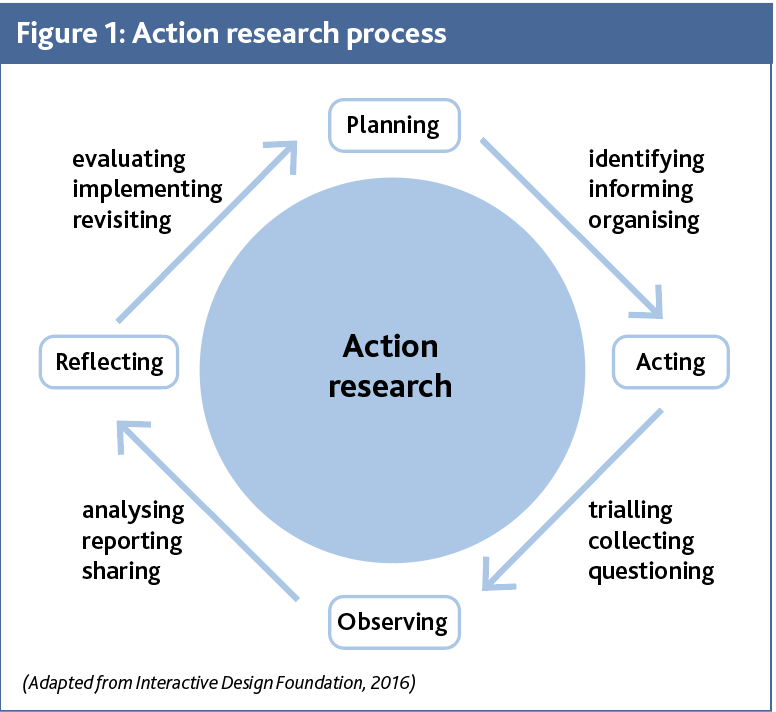
Participation is a central strategy of this process as well as a focus on generating solutions to practical problems.30 Action research is considered a useful and versatile process; linking theory and practice, thinking and doing; to achieve practical objectives.30 The approach is problem focused, context specific, emphasises participation, collaboration, reflection and involves change interventions modelled for improvement.31 In contrast to traditional approaches, the process is based on cycles of research, action, reflection and evaluation (see Figure 1 overleaf).30
 (click to enlarge)
(click to enlarge)