Atrial fibrillation (AF) is the most common cardiac arrhythmia, affecting at least 3% of Irish adults over 60 and 6% over 70.1 The worldwide prevalence has been rising and is currently approximately 600 in men and 375 in women per 100,000 population.2 Atrial fibrillation is associated with almost one in three strokes in Ireland and is associated with more disabling neurological deficits due to, in the main, clot burden and a relatively poor recanalisation rate of only 40% with intravenous thrombolysis in such cases of large vessel occlusion (LVO).
While prognosis after an AF-associated stroke has improved with the advent of endovascular treatment of stroke with mechanical thrombectomy, nevertheless, many such strokes are not amenable to this treatment. The treatment is expensive and carries some risk, and the majority of cases treated will still need periods of rehabilitation in hospital post-procedure.
Atrial fibrillation is an age-related condition and in addition to the manifest risk of stroke the evidence for its role in cardiac failure with preserved left ventricular dysfunction, fatigue, poor quality of life and dementia is growing.
Europe has an ageing demography and a challenging increased prevalence of cases of AF is on the immediate horizon. The Stroke Alliance for Europe, in its report Burden of Stroke in Europe has signalled a possible 58% increase in the absolute numbers of stroke in Ireland over the next decade or so and much of this can be accounted for by increasing numbers of AF-related stroke as our population ages.3 Reducing the incidence of AF and ensuring effective stroke prevention in cases of AF remains a key goal for all cardiovascular and stroke programmes.
For all the recent advances we are still in a relative infancy in our understanding of the pathophysiology of AF, its association with risk of stroke and other illnesses. While much progress has been made in the past 10 years, in particular with collaborative interdisciplinary working and research between cardiologists, stroke physicians, primary care providers and industry, nevertheless there are many unanswered questions and dilemmas in AF and more collaborative work is needed.
SPAFI – an interdisciplinary initiative
In Ireland we have recently launched an interdisciplinary initiative, Stroke Prevention and Atrial Fibrillation Ireland (SPAFI) to try and comprehensively address the challenge of AF and to try and answer some of our ‘known unknowns’ and discover our ‘unknown unknowns’ about the condition.
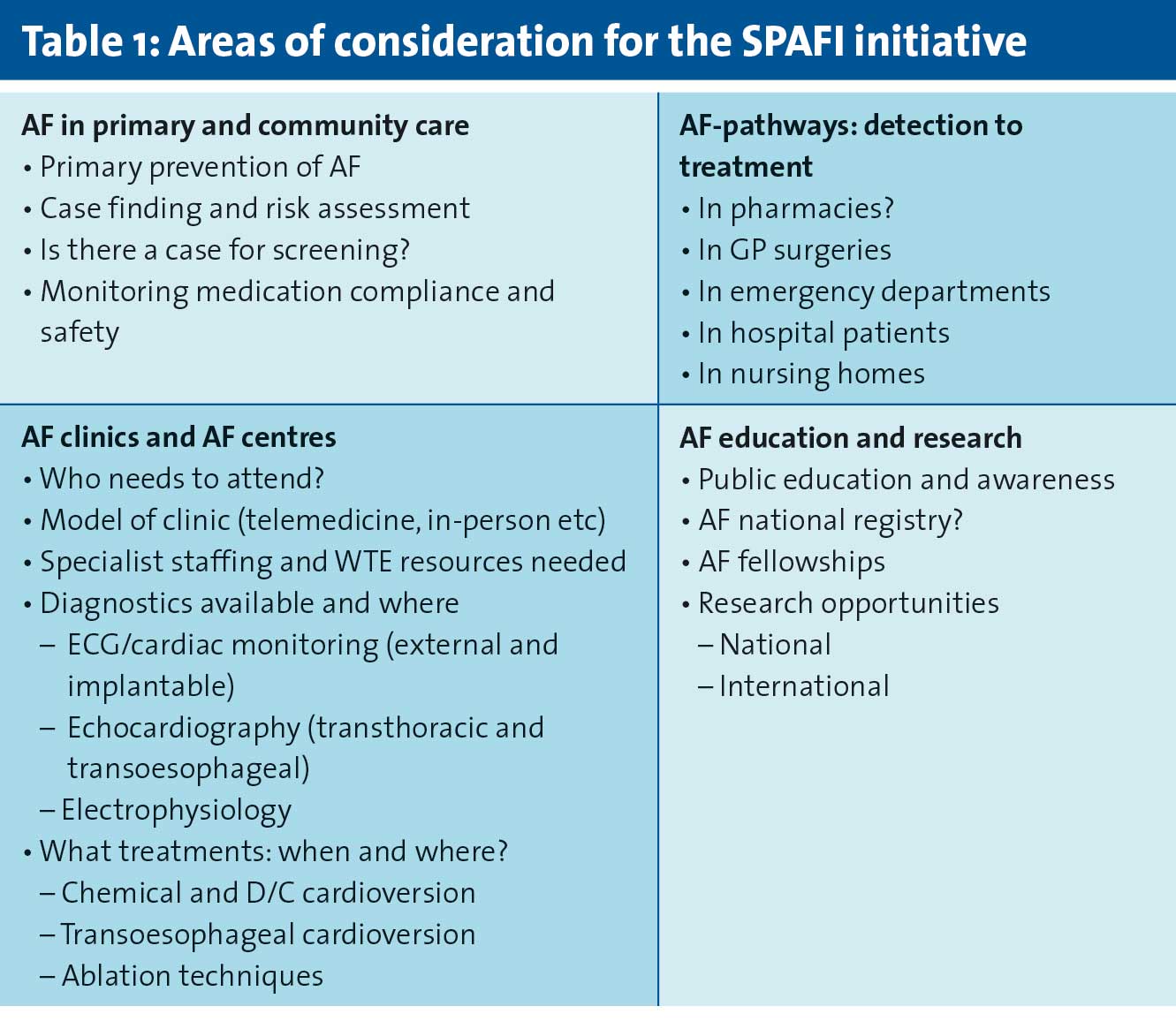
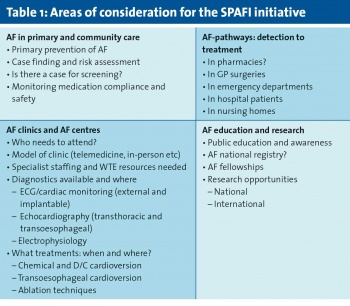
SPAFI takes its name in part from the seminal ‘stroke prevention in atrial fibrillation’ trial in the 1990s, one of the first to show the benefit of anticoagulation with warfarin in preventing stroke in AF. Much progress has of course been made in drug therapy since that time with the advent of modern anticoagulants (NOACs or DOACs depending on the professional body you speak to, though hopefully an agreed class nomenclature is imminent), and SPAFI has a broader goal to create a consensus clinical document for AF in Ireland (see Table 1).
(click to enlarge)
Addressing these areas needs broad specialty expertise, and SPAFI has put together a steering group of cardiologists, geriatricians and stroke physicians, GPs, public health doctors, pharmacists, health economists and nurses (ANPs and research) with an interest in AF, to focus on relevant areas of expertise and underpin a national approach to AF with a clear and economically articulated strategy.
This is a large task and the group is not an exclusive one but rather an initial one to get ‘working groups’ formulated around major questions for the future treatment of AF in Ireland which will consult widely.
The initiative has the support of the ICGP, the Irish Heart Foundation (IHF), Irish Pharmacy Union (IPU), Royal College of Physicians of Ireland (RCPI), HSE national stroke, older persons and chronic disease management programmes, the Irish Cardiac Society (ICS), Irish Physicians in Geriatric Medicine and Stroke Clinical Trials Network Ireland, and has received positive feedback from international colleagues as the potential model to be adopted elsewhere to tackle AF effectively.
To launch the initiative, an inaugural meeting of the group was held at the RCPI on November 8. An array of national and international speakers addressed: The challenge of atrial fibrillation in Ireland (Dr Niamh Hannon), ‘What’s new or missing in the EHRA practical guide to NOAC use in AF ?’ (Prof Jan Steffel), ‘Educating the AF patient – what have we learned? (Dr Lien Desteghe) and ‘Can we prevent or cure AF?: an ageing conundrum’ (Prof John Camm).
AF: primarily a disease of primary care
AF is primarily a condition encountered or picked up routinely in primary care and is more often than not asymptomatic. The new GP agreement is including opportunistic pulse-checking in older adults (> 65) as a means of improving our detection rate of atrial fibrillation, basing its approach on the finding that opportunistic pulse-checking was shown to be both feasible and cost-effective in an Irish setting.
When such screening was implemented in the west of Ireland in over-65s, a prevalence of 10.9% was found in 7,500 patients who underwent opportunistic pulse-checking and while many of these cases were already diagnosed, an incidence of 17/1,000 new cases was detected.4
Other more systematic continuous screening studies in Ireland in high-risk patients with no prior history of AF have found an incidence of 14% of any AF, if a CHADS2 > 2 was used as the baseline criteria for systematic screening.5 A similar high-risk patient screening study is currently underway in Galway and there is much for us to address both nationally and internationally when it comes to case-finding or screening for AF.
Debate about screening
Much is debated about screening for AF. While as a condition it fulfils many of the original, yet perhaps outdated, Wilson and Jungner WHO criteria for a screening programme,6 the exact pathophysiology and relationship to disease is still not fully understood. For example, on the one hand one doesn’t want to be over-calling a systemic risk in small and possibly innocent short runs of AF which many people may ordinarily and physiologically have, but on the other hand one doesn’t want to miss the dangerous forerunner of a serious stroke.
In between lies the issues of ‘disease creation’ versus recognising an ‘at-risk tendency’ and prequel of persistent AF, and that AF in itself may be a marker of systemic cardiovascular risk not confined to the atrium.
We already have a greater awareness that the risk of developing AF is increased by obesity, alcohol overuse, hypertension, family history and hyperthyroidism and that the observation of frequent atrial premature contractions (APCs) on cardiac monitoring is a risk for subsequent development of atrial fibrillation. AF may therefore have both a preventable and pre-disease phase where focused multi-faceted interventions including lifestyle, medication and electrophysiology can prevent development of the arrhythmia. Prevention of AF needs more research and clinical focus.
We are also beginning to recognise that the risk of stroke and thromboembolism in AF may not be a static one. It is very likely that other conditions such as malignancy, infection or chronic inflammation increase this risk in the fibrillating atrium in ways not yet fully appreciated, but very plausible with the increased circulating cytokines, antibodies and pro-coagulant factors associated with such conditions all making for a thicker ‘cement’ entering a ‘faulty cement mixer’.
Uncertainties
While ESC guidelines on the management of AF are quite clear on who we should anticoagulate for stroke prevention,7 and are due to be updated next year, there are still some uncertainties about who can or should case-find and diagnose AF, who should initiate and is ‘qualified’ to initiate treatment, who needs a specialist clinic opinion and who is truly at low risk and doesn’t need anticoagulation but may need monitoring and what that monitoring should entail.
A number of national and international GP-and pharmacy-led projects have demonstrated an ability to case-find AF,8 but the pathway between case-finding, confirmatory diagnostics and initiation of treatment is not well agreed or described nationally. This does need definition as AF is an emergency even when not symptomatic and requires an immediate risk-benefit analysis and initiation of anticoagulation where appropriate. There is no certainty at time of diagnosis that the AF has not been there for some time already, or that a thrombus has not already formed in the left atrial appendage and is at the point of embolisation.
This is a common quandary that arises with regard to the management of stroke prevention in AF in primary care and emergency departments in my experience. While an echocardiogram is a stated guideline for evaluation of the AF patient, an agreed clinical pathway would be more pragmatic and useful in the first instance and is something we hope to evolve quickly from SPAFI.
The ‘low-risk patient’ – AF and stroke risk
While the risk of stroke is a paramount consideration in AF and much has improved with successive iterations of vascular risk scores such as CHADS2 and CHA2DS2-VASc, the C-statistic of such scores remains poor at a 0.60 average, and while addition of biomarkers NT Pro-BNP and highly sensitive cardiac troponin raises this predictability to a modestly healthier 0.71,9 they are still approximates of risk and do not assess an individual atrium’s thrombogenicity when fibrillating nor at the time of diagnosis.
Analysis from real-life registries has validated the use of other clinical factors such as renal function as well as ethnicity to improve risk-benefit analysis of anticoagulation in apparent low-risk patients10 and to predict both risk of stroke and risk of bleeding more accurately. Many other biomarkers like interleukin-6 and fibroblast-derived growth factor are also showing promise in both detecting AF and predicting risk of stroke in AF.11
Echocardiographic analysis of the fibrillating atrium including morphology of the left atrial appendage, left atrial reservoir strain and ‘P-wave to A’ time on tissue Doppler imaging (PA-TDI) can give further useful clues as to what might be a highly thrombogenic atrium even on transthoracic echocardiography.12
However, this is not readily available in primary care with current technology, is a time-consuming and expensive examination, invasive and requiring IV sedation in the case of transoesophageal echocardiography and imaging criteria are as of yet unproven as a population-based method of risk stratification.
It is very likely that risk scores for stroke in AF such as CHA2DS2-VASc will be modified or changed in the ESC guidelines in the near future, especially when evaluating apparent low-risk patients.
The zero sum game: AF and CHA2DS2-VASc = 0 patient? (including females < 65)
The current ESC guidelines13 definitely recommend no treatment with a CHA2DS2-VASc score of zero in men and one in women (also a true zero as the score for female sex is only a consideration > 65yrs). The guidelines are clear that antiplatelets have no role in stroke prevention in AF, a view strongly supported by the findings of the ACTIVE-W study where dual antiplatelets (DAPT) were inferior to anticoagulation with vitamin-K antagonists, in stroke prevention.14
However, this does not mean that patients with AF and a score of zero have no risk of stroke; they do. This annual risk is probably less than 1% in this overall population15 though it has been reported as high as 2.4%.16 Within this ‘low-risk’ population however, it may be hard to assess the true risk accurately in the individual and of course such risk may change in circumstances where there is an added hypercoagulable state, eg. a malignancy or when undergoing surgery and even perhaps during infection.
A dilemma remains therefore on how to treat such patients. As these patients are younger by definition, then lifestyle advice, weight reduction and careful monitoring of blood pressure may help reduce paroxysmal episodes or development of persistent AF which is desirable. Ablation should be considered as an option in all symptomatic and younger patients without structural abnormality, but a decision to anticoagulate can remain difficult in such apparently low-risk patients.
Current guidance on the issue should be tempered with specialist cardiac/stroke-prevention opinion, with biomarkers and transoesophageal echocardiographic evaluation, as while the risk of stroke is probably much less than 1% in such patients it is not zero, a fact that needs explaining to patients as the relatively rare occurrence of stroke in this population is difficult to accept as ‘rare bad luck’ when a known risk was present and seemingly untreated.
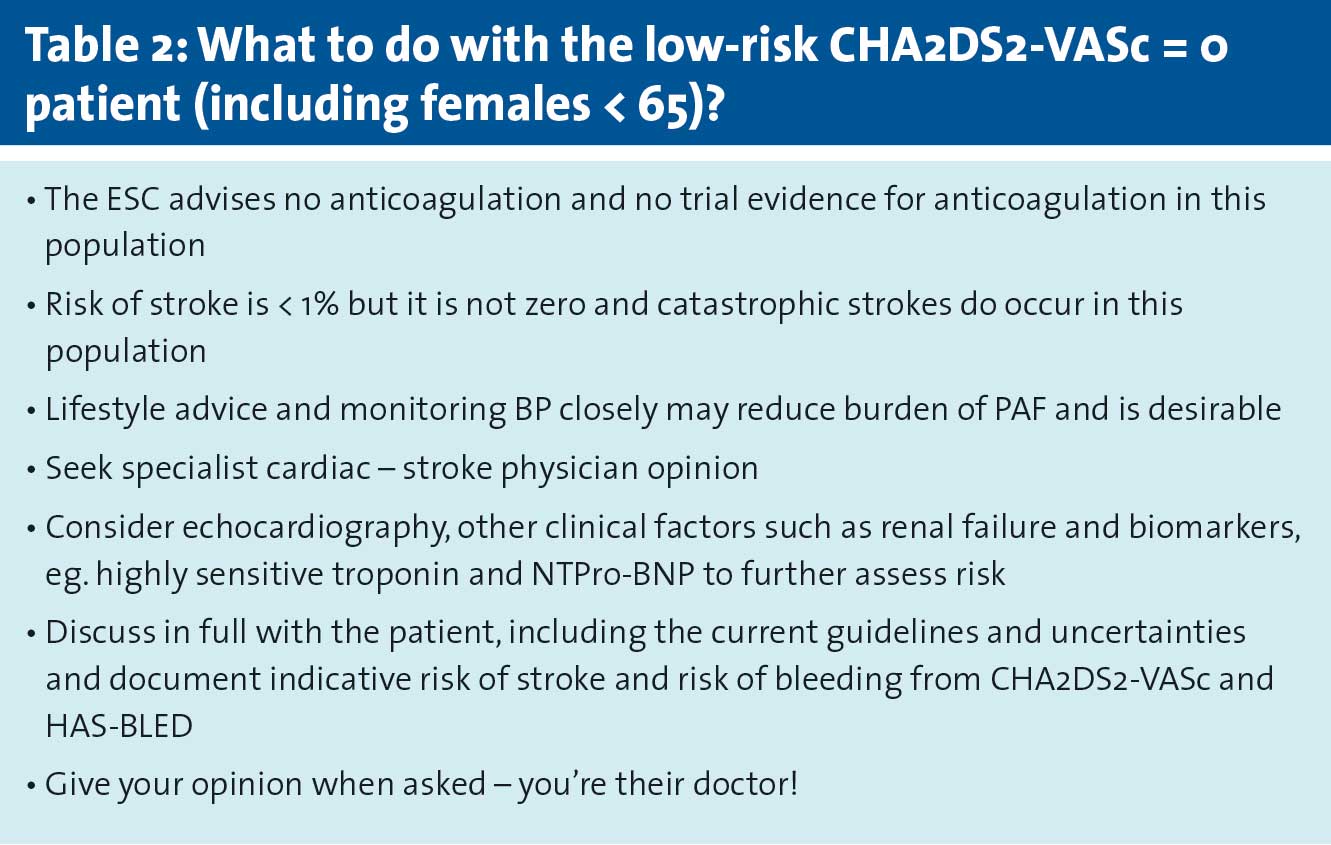
Certainly in the ‘zero’ CHA2DS2-VASc patient where the risk of bleeding, as determined by HAS-BLED, is low and other factors are present that may increase thrombogenic risk, or where cardiac opinion or imaging is suggestive of a ‘dangerous’ atrium, it seems reasonable to consider anticoagulation outside the guideline. This is especially the case where other risk factors – not accounted for in CHA2DS2-VASc but established from registry work as risk factors, such as renal failure – are present or where biomarkers associated with increased risk of stroke in AF such an NTPro-BNP are raised.
It is important to document the discussion in all cases with an indicative risk of stroke and bleeding explained to patients together with an explanation of the lack of individual certainty in this group with available risk scores. This will usually in my experience prompt a patient to ask your advice. That is after all why patients are consulting you and not Google. A pragmatic approach to the ‘low risk’ (CHA2DS2-VASc = 0 male or 1 [female sex only]) patient is suggested in Table 2.
(click to enlarge)
Rónán Collins is clinical lead of the National Stroke Programme and inaugural co-chair of SPAFI
Donoghue OA, et al. Atrial fibrillation is associated with impaired mobility in community-dwelling older adults. J Am Med Dir Assoc. 2014; 15(12): 929-33
Chugh SS, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014; 129(8): 837-47
Smyth B, Marsden P, Corcoran R, et al. Atrial Fibrillation screening in general Practice (March 2015). Health service Executive
Collins R et al. Stroke Prevention: community based remote screening for atrial fibrillation in high risk cohorts. Eur Stroke J 2017:2 (IS).AS04-023:p164
Fang MC, Go AS, Chang Y et al. Comparison of risk stratification schemes to predict thromboembolism in people with nonvalvular atrial fibrillation. ATRIA Study Group. J Am Coll Cardiol. 2008; 51(8): 810-5
Wilson JMG, Jungner G. Principles and Practice of Screening for Disease, World Health Organization, 1968
Kirchhof P, et al. 2016 ESC guidelines for the management of atrial fibrillation
S McCool, P Logan. Irish Pharmacy Union pilot to detect hypertension and atrial fibrillation in the community 2018 report
Ruff CT, et al. Cardiovascular Biomarker Score and Clinical Outcomes in Patients With Atrial Fibrillation: A Subanalysis of the ENGAGE AF-TIMI 48 Randomized Clinical Trial. JAMA Cardiol. 2016;1(9):999-1006
Fox KA, et al. Improved risk stratification of patients with atrial fibrillation: an integrated GARFIELD-AF tool for the prediction of mortality, stroke and bleed in patients with and without anticoagulation. BMJ Open 2017;7:e017157. doi:10.1136/ bmjopen-2017-017157
Chua et al. Data-driven discovery and validation of circulating blood-based biomarkers associated with prevalent atrial fibrillation. Eur Heart J. 2019; 40(16): 1268-1276
Leung M, et al. Left atrial function to identify patients with atrial fibrillation at high risk of stroke: new insights from a large registry. Eur Heart J. 2017 Dec 28. doi: 10.1093/eurheartj/ehx736
Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace2016:18(11): 1609-1678
Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial. ACTIVE Writing Group of the ACTIVE Investigators. Lancet. 2006; 367(9526): 1903-12
Manolis AS, et al. Stroke Risk Stratification Schemes in Atrial Fibrillation in the Era of Non- Vitamin K Anticoagulants: Misleading and Obsolete, At Least for the “Low-Risk” Patients? Curr Drug Targets. 2017;18(16):1852-1865
Huang D, Anguo L, Yue WS, Yin L, Tse HF, Siu CW. Refinement of ischemic stroke risk in patients with atrial fibrillation and CHA2 DS2 -VASc score of 1. Pacing Clin Electrophysiol. 2014; 37(11): 1442-7
 (click to enlarge)
(click to enlarge)