South Tipperary General Hospital instituted a ‘sepsis survival chain’ with the ultimate aim of reducing sepsis-related deaths
Ms Oonagh Keating, Assistant Director of Nursing, Surgical Directorate, South Tipperary General Hospital, Clonmel, Co Tipperary and Dr Marcella Lanzinger, Consultant Anaesthetist in Intensive Care Medicine, South Tipperary General Hospital, Clonmel, Co Tipperary
Sepsis is an aggressive life-threatening and multi-factorial disease state. Sepsis interrupts oxygen and nutrient supply to the tissues and vital organs such as the brain, intestines, liver, kidneys and lungs. The speed and appropriateness of therapy in the initial hours are likely to influence outcome.1 Sepsis is a medical emergency just like a heart attack or a stroke.
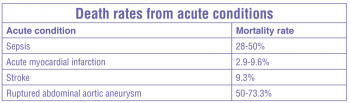
Sepsis has one of the highest death rates from acute disease. It is similar to the mortality rate from myocardial infarction in the 1960s. Medical advances and public information campaigns have significantly reduced mortality associated with coronary artery disease.
(click to enlarge)
South Tipperary General Hospital (STGH) has established a hospital-wide ‘sepsis survival chain’ that supports staff in consistently providing early goal-directed treatment for adult septic patients in all departments according to best current international standard of care. In this article we outline how a general hospital in Ireland became an active and enthusiastic member of the ‘Surviving Sepsis Campaign’.
The first step: MEWS
Four years ago in 2009, STGH launched its modified early warning system (MEWS). The merits of a number of national and international examples were adapted by the stakeholders to suit the needs of a then 300-bed Band 3 hospital with its associated staffing.
A MEWS alert prompted escalation of care. The clinical care pathways for chest pain and stroke at STGH ensured these patient groups received early goal directed treatment. Septic patients, however, did not yet have a dedicated pathway.
The second step: Recognising the problem
One year into the MEWS, staff was comfortable in its use but also increasingly frustrated with a perceived shortfall: there was a structural gap for direction of subsequent clinical care for septic patients.
MEWS ended with ‘escalate care’ with no formalised subsequent approach for the significant cohort of septic patients. A patient’s access to intensive care treatment (especially in the early phases of sepsis) could be preceded by a number of phone calls, diagnostics and treatment efforts. This was very frustrating and time consuming. A support structure to facilitate optimal clinical care similar to the MEWS was desired.
The third step: Identifying a solution
There were two freely available solutions to the problem: ‘The Surviving Sepsis Campaign’ and the ‘Sepsis Six Programme’ supported by the College of Emergency Medicine.
Surviving Sepsis Campaign
The Surviving Sepsis Campaign (SSC) is an initiative of the European Society of Intensive Care Medicine and the US Society of Critical Care Medicine. It was developed in 2002 (updated in 2008 and 2012) to improve the management, diagnosis, treatment and improve survival of sepsis worldwide. The campaign’s initial declared goal was to reduce mortality from sepsis by 25% in five years. The new goal for 2012 was to increase the number of hospitals contributing data to the SSC to 10,000 hospitals worldwide and to apply the guidelines to 100% of patients suspected to have severe sepsis or septic shock. It represents an unprecedented global effort to reduce death from sepsis.
The Sepsis Six Programme
In 2006 a group of people working on the implementation of the SSC guidelines in the UK developed a condensed version of the Resuscitation Bundle of the SSC. The group identified a set of six critical initial actions in the management of sepsis.
Bedside nurses can dramatically improve a patient’s chance of survival by ensuring that six simple things (Sepsis Six) are done in the first hour.3
The STGH Sepsis Survival Chain
The STGH Sepsis Task Group determined that a combination of a Sepsis Screening Tool, the Sepsis Six and the SSC bundles together with a comprehensive educational effort would provide the best chance of success and sustainable effort. It would fill the gaps in structured care with direct links to the MEWS and ongoing management in intensive care.
The STGH clinical care pathway for the management of severe sepsis and septic shock
During the development of the pathway it was recognised that adjustments would need to be made to account for differences in patient groups and location.
First, the SSC at the time was aimed at adult patients only; thus paediatric patients were excluded.
Second, physiological changes during pregnancy correspond with a significant change in vital signs and parameters. In consultation with the Department of Obstetrics, adjustments were made to the screening tool for recognition of sepsis to allow for pregnancy-related changes.
Third, the dataset available for patients on the wards differed significantly from the ED, where patients were generally presenting without prior data for comparison.
One generic pathway evolved into three specific pathways: for adult patients on the wards, adult patients in ED and maternity patients.
The Sepsis Screening Tool was modified in that we added a parameter for the recognition of the septic patient. This parameter is listed as “patient concern/looks unwell”. The inclusion of this parameter was to allow for assessment and escalation of care of a patient that was felt to be deteriorating without triggering any of the official alerts.
Audit of compliance and outcomes would be vital to the success of the campaign. In order to facilitate data collection, audit data collection was integrated into the pathway.
STGH guidelines for the management of severe sepsis and septic shock
These guidelines provide detailed recommendations also beyond the initial resuscitation. This not only facilitates the development of a critical care plan but also ensures a consistent approach across all teams in the management of these patients. This in turn makes it much easier for nursing staff to anticipate care needs and plan options.
The fourth step: Implementing the solution
Teamwork makes the dream work: The hospital-wide Surviving Sepsis Campaign
The sepsis campaign at STGH originated as a grassroots campaign. Staff were keen to set up a tool to facilitate a consistent approach to the treatment of septic patients.
In order for the STGH campaign to function, buy-in from all stakeholders was required. Led by our consultant intensivist, a group representing consultants, clinical risk manager, nursing staff from the clinical areas, the nurse practice development facilitator and assistant directors of nursing committed to establishing a hospital wide programme.
Departmental buy-in
The heads of departments of Medicine, Surgery, Anaesthesia and Gynaecology/Obstetrics, ICU and ED committed to instituting educational programmes for their staff with an emphasis on regular re-education to capture new staff members, particularly in July.
Administrative buy-in
Administration backed the campaign. The ‘Sepsis Six’ sheets are printed regularly and are an official component of the patient’s record. Events highlighting the campaign are supported.
Raising awareness
A sense of anticipation was created prior to launching formal education and documentation. As staff themselves had highlighted the need for more stringent management of septic patients they were very enthusiastic that action was being taken. After the MEWS, the Sepsis Pathway appeared a natural progression.
A large poster outlining the campaign is on display in the main hospital foyer. The poster highlights the focus on sepsis at the hospital. It is a source of interest to the public who often make reference to it in discussion with staff.
Education
Trainers volunteered from all grades of medical and nursing staff to facilitate a consolidated schedule of formal and informal training sessions on both days and nights.
Medical and nursing staff across the hospital were trained including ED, ICU, CCU, maternity and all adult wards.
Healthcare assistants FETAC level 5, and allied health professionals were included in the education. The RGN assigned to the patient retains responsibility for the patient’s nursing care.
Training on the pathway was incorporated into the induction programme for staff from July 2011. Nursing staff received refresher training as needed.
The introduction of the national early warning score (NEWS) at STGH in April 2012, with its associated educational programme, provided an opportunity to re-emphasise the STGH sepsis pathway and actions as prompted in the Sepsis Six trigger of the NEWS.
The recent update according to the 2012 Sepsis Guidelines will be the new focus of education in the tools of the Sepsis Survival Chain.
Launch of the Campaign
The pathway was launched in two phases. It was first piloted in the ED and the ICU. In April 2011 the Campaign was rolled out to the rest of the hospital.
Audit
Collection and analysis of data from bundle compliance is the key to improvement. An audit data collection tool is integrated into the pathway. Performance analysis and patient outcomes are defined audit goals.
Resource limitations
There were minimal additional resources available to launch the campaign. We utilised resources that were freely available. Champions were found to drive and sustain implementation. However we were not able to sustain the effort of data entry to the SSC database.
Transient staffing pools
Agency and locum staff are generally unfamiliar with the sepsis pathway in use at STGH. New agency nursing staff are given a brief overview at the beginning of the shift and asked to alert ward staff for assistance if they have a suspicion of sepsis. Locum doctors are prompted to adhere to the pathway and associated time limits and actions.
A similar problem of unfamiliarity had been experienced when MEWS/ViEWS was not widely utilised in other hospitals. It is therefore anticipated that as SSC pathways become more widespread these issues will diminish.
The sepsis pathway
The pathway document incorporates four pages in a booklet
Page 1: Definitions and rationale
Page 2: Sepsis – Screening tool with nursing goals
Page 3: Sepsis confirmation with doctor’s goals
Page 4: ‘Sepsis Six’ early goal-directed therapy and escalation of care.
All steps are ticked off on completion, timed and signed. Audit data collection is integrated.
Sepsis screening tool and nursing goals
Any healthcare provider that has a serious patient concern possibly due to infection or triggered by a MEWS alert of four can initiate the pathway. Vital signs and glucose levels are documented and assessed for suspicion of sepsis. If confirmed, care is to be escalated to a senior decision maker (registrar/consultant). By thus empowering staff, valuable time is saved.
Administration of oxygen,12-lead ECG, intravenous access, specified blood tests and specimens for microbiology are important goals that the nurse completes prior to arrival of the doctor.
Doctors’ goals
The doctor documents a focused history and examination. With arterial blood gas analysis and blood cultures taken, the doctor confirms recognition of sepsis or severe sepsis against defined criteria for SIRS and acute organ dysfunction on the check list.
Sepsis Six and initial resuscitation
Six essential interventions – ‘Sepsis Six’ – need to be completed within the first hour of recognition of sepsis. If septic shock is confirmed, intensive care expertise needs to be requested. Valuable time for the patient is gained by thus escalating communication and preparing optimal ongoing care with minimal delay.
Sepsis Six actions
100% oxygen
IV fluids
Blood cultures
IV antibiotics
Urinary catheter
Lactate, laboratory data, source evaluation
Step-by-step guidance is included for each action, with bullet point prompts and cautions.
Nursing and medical staff share responsibility for ensuring the pathway is completed.
Key points
Initiation by any healthcare provider
Escalation to senior decision maker (registrar/consultant) upon suspicion of sepsis
Access to intensive care expertise upon recognition of sepsis.
Resuscitation of septic shock and supportive therapy
Previously called the management bundle, this includes a set of actions to be applied after the initial resuscitation is complete. Generally, this phase will be led by intensive care expertise, ideally the patient will have been moved to a critical care unit for further treatment.
Feedback
Based on staff feedback, we note significant staff satisfaction on the nursing side with the Campaign. They welcome the ability to initiate care for their patients when they are concerned; the fact that the sepsis pathway empowers them to quantify their concern and voice it in a communal language. The Sepsis Campaign has become part of the culture at STGH.
It was recognised that areas with fewer opportunities to use the pathway will require more frequent education to maintain familiarity with the sepsis pathway.
We are confident that our Campaign is successful in ensuring appropriate care and reducing sepsis related death. Survive Sepsis has recently published findings that support our expectations. 2
The fifth step: sustaining the campaign
Audit will be essential to demonstrate that we are compliant with best practice. It will enable benchmarking and drive future organisational policy changes. Resources for data entry will need to be identified.
All involved have been most supportive and proactive in sustaining the sepsis campaign. This is sincerely acknowledged. September is sepsis awareness month and the STGH Sepsis Task Group is planning a series of internal and public events to highlight the campaign and strengthen our support base.
In the end – it is still just the beginning
“The thing about a guideline is that it is a nice reference text,” explained R Phillip Dellinger, lead author of the guideline and professor of medicine at the new Cooper Medical School of Rowan University in Camden, New Jersey.
“It doesn’t change bedside behaviour a lot or very fast,”4 he added.
We agree wholeheartedly and we encourage other hospitals to join in and set up their own sepsis campaign. We believe that all Irish hospitals could join the campaign with a national goal of reducing sepsis mortality and related illnesses in Irish patients.
Acknowledgements
The STGH Sepsis Task Group, Maria Barry ADON, Medical Directorate. Dr Niall Colwell, Coronary Care Unit, Marie Laste, Nurse Practice Development Facilitator, Dr Cyrus Mobed, Emergency Medicine, Fiona Ryan, CNM2, Intensive Care Unit, Mairead Vaughan, CNM3, Emergency Medicine, the STGH Critical Care Governance Group and all staff that have assisted providing education and sustaining the campaign.
In memoriam
Margaret Molony, clinical risk manager, who was instrumental in implementing the MEWS at South Tipperary General Hospital.
References
Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012. Crit Care Med 2013; 41: 580-637
Daniels R, Nutbeam T, McNamara G, Galvin C. The sepsis six and the severe sepsis resuscitation bundle: a prospective observational cohort study. Emerg Med J 2011;28:507-512 doi:10.1136/emj.2010.095067
Robson WP, Daniel R: The Sepsis Six: helping patients to survive sepsis. Br J Nurs 2008 Jan 10-23; 17(1): 16-21
Bridget M. Kuehn: Guideline Promotes Early, Aggressive Sepsis Treatment to Boost Survival, MSJ JAMA 2013; 309(10): 969-970. doi:10.1001/jama.2013.1295
 (click to enlarge)
(click to enlarge)