Testosterone deficiency should be considered in men with suggestive signs and symptoms, particularly those who are older or with comorbidities such as type 2 diabetes or obesity
Late onset testosterone deficiency or hypogonadism is a deficiency of testosterone in men as they age. It is the second most common endocrine disorder in men after type 2 diabetes. It can lead to a range of signs and symptoms that can significantly affect quality of life and is a risk factor for type 2 diabetes and osteoporosis, among other conditions.
There are a number of causes for testosterone deficiency as outlined below. This module focuses on the adult male with low testosterone levels due mainly to age and in some cases lifestyle. With increased awareness of the link between ageing and symptoms of testosterone deficiency, GPs are being asked more often about screening and treatment.
From a GP perspective it is important to know who should be screened with respect to signs, symptoms and comorbidities.
Testosterone deficiency, or hypogonadism, is defined as the absence or reduction of hormone secretion, or other physiological activity of the testes. It can be ‘classical’ or secondary to age and comorbidities and known as late onset hypogonadism.
It may result from:1,2,3
• Problems with the testes: primary (hypergonadotropic) testosterone deficiency
• Problems with the hypothalamus and pituitary gland: secondary (hypogonadotropic) testosterone deficiency
• Problems with the hypothalamus/pituitary and testes (combined primary and secondary testosterone deficiency)
• Impaired action/suppression of testosterone, also known as testosterone resistance.
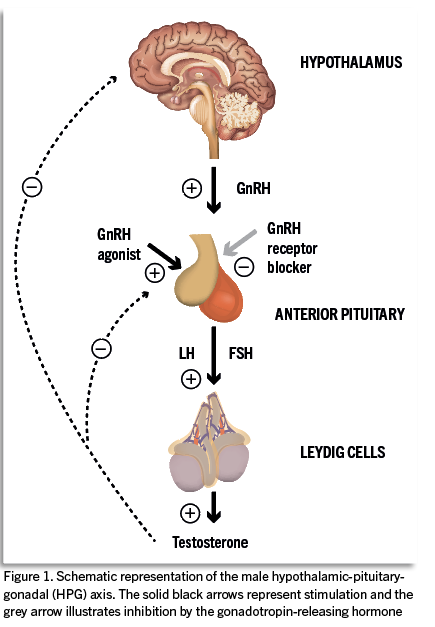
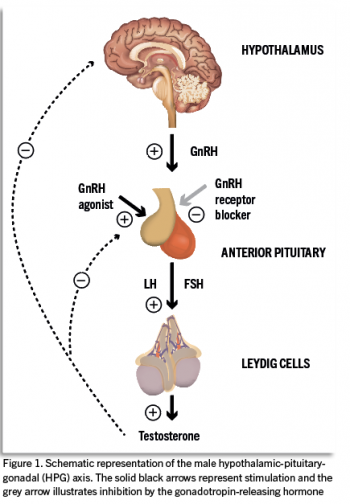
See Figure 1 for illustration of the male hypothalamic-pituitary-gonadal (HPG) axis. Classical testosterone deficiency can be further subdivided into primary, secondary and combined primary/secondary causes. Primary hypogonadism occurs when there is a direct problem with the testes, such as in Klinefelter syndrome, or acquired for example, following chemotherapy.
(click to enlarge)
Secondary causes, such as pituitary disease or Kallman syndrome, occur when the signalling from the hypothalamic-pituitary-testicular axis is interrupted. Classical testosterone deficiency is almost always treated, usually commenced under specialist supervision.
Primary (hypergonadotropic hypogonadism)
With this type, the pituitary gland produces more luteinizing hormone (LH) and follicle-stimulating hormone (FSH) – known as gonadotropins – in response to low testosterone levels. In primary hypogonadism, testosterone levels can be within the normal range and gonadotropins are high.
Congenital conditions that can lead to primary hypogonadism include:
• Absence of testicles at birth (anorchia)
• Undescended tests (cryptorchidism)
• Leydig cell hypoplasia (underdevelopment of Leydig cells in the testicles)
• Klinefelter’s syndrome (a genetic condition in which people are born male with an extra X chromosome: XXY instead of XY)
• Noonan syndrome (a rare genetic condition that can cause delayed puberty, undescended testicles or infertility)
• Myotonic dystrophy (part of the muscular dystrophies group of inherited disorders)
Acquired conditions that can lead to primary hypo-
gonadism:2
• Testicle injury or removal
• Orchitis, which is inflammation of one or both testicles. This is most often the result of a bacterial infection, such as a sexually transmitted infection. It can also be due to a viral infection, such as mumps
• Chemotherapy or radiation therapy involving the testicles
• Certain tumours
• Use of anabolic steroids.
Causes of secondary male hypogonadism3
This is known as hypogonadotropic hypogonadism because there are low levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
Congenital conditions that can lead to secondary hypogonadism include:
• Isolated hypogonadotropic hypogonadism: a condition that causes low levels of gonadotropin-releasing hormone from birth)
• Kallmann syndrome: a rare genetic condition that causes loss of the development of nerve cells in your hypothalamus that produce gonadotrophin-releasing hormone. It can also cause a lack of smell
• Prader-Willi syndrome: a rare genetic multisystem disorder than can cause hypothalamus dysfunction.
Acquired conditions that can lead to secondary hypogonadism include:
• Hypopituitarism. This condition may result from an adenoma, infiltrative disease, infection, injury, radiation therapy or surgery that affects the pituitary gland
• Hyperprolactinaemia
• Haemochromatosis
• Brain or head injury
• Cushing’s syndrome
• Cirrhosis of the liver
• Kidney failure
• HIV/AIDS
• Alcohol use disorder
• Poorly managed diabetes
• Obesity
• Obstructive sleep apnoea
• Certain medications, including oestrogens, psychoactive drugs, metoclopromide, opioids, leuprolide, goserelin, triptorelin and newer androgen biosynthesis inhibitors for prostate cancer.
Late onset testosterone deficiency
Late onset testosterone deficiency is a type of hypogonadism which occurs as a result of ageing and associated comorbidities (this can also affect women). In these circumstances, men suffer a gradual decline in testosterone production or impaired action due to deterioration of hypothalamic-pituitary function and Leydig cell function (where testosterone is produced in the testes). There can also be a case of testosterone resistance where there is a down regulation of the androgen receptor similar in principle to insulin resistance. This results in many associated clinical signs and symptoms.
Serum testosterone levels decline slowly between 40 to 70 years of age, at an approximate rate of 0.8 per cent per year.4 While estimates vary, prevalence of testosterone deficiency was found to be 3.1% to 7% in a sample of American men less than 70 years old. This increased to 18.4% in 70-year-olds.5 Other studies have shown that it occurs in 20% to 39% of men aged 40-79 years.6,7,8 The incidence of testosterone deficiency is even more prevalent when there are other comorbidities such as obesity, type 2 diabetes and hypertension, or with extended drug exposure to agents such as opiates or chemotherapy.7
Typically, a middle-aged man may present with low mood or increased anxiety. On further questioning, he may reveal a history of reduced libido or the inability to maintain erections. Without prompting, it may never have crossed his mind to mention such symptoms, or to ask for help.
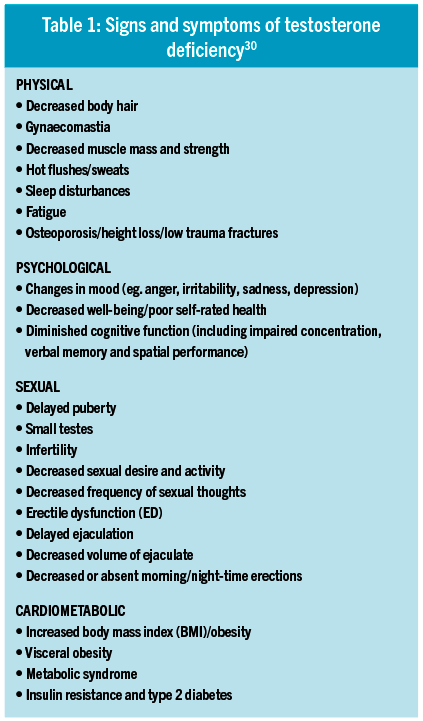
The symptoms fall into four main categories:
• Physical: Loss of strength, central weight gain, loss of muscle mass, and increased fatigue
• Psychological: Fluctuations in mood, increased anxiety, and loss of confidence
• Sexual: Erectile dysfunction, loss of morning erections and reduced libido
• Cardiometabolic: Visceral obesity, metabolic syndrome, type 2 diabetes (see also Table 1).
(click to enlarge)
Assessment of testosterone deficiency
The diagnosis of symptomatic testosterone deficiency requires the presence of characteristic signs and symptoms,1,9,10,11,12plus reduced serum concentrations of total testosterone or free testosterone.9
These symptoms can be assessed quickly and easily using the ADAM (Androgen Deficiency in the Ageing Male; log on to: www.testosterone.ie) or use the AMS (Ageing Male Symptoms) questionnaires. As the symptoms listed earlier are common, they are often seen as part of the ‘natural process of getting old’, and in many cases testosterone deficiency is overlooked. The three most common symptoms of testosterone deficiency are ED, loss of early morning erections and low sexual desire.12,13
It is very important to screen high-risk groups for testosterone deficiency, These include men with erectile dysfunction, type 2 diabetes, a BMI > 30 or a waist circumference > 102cm, loss of libido or on medications such as antipsychotics, opioids or antiepileptics.
All male patients with hypogonadism should be evaluated for being overweight or obese and all male patients with type 2 diabetes should be evaluated for testosterone deficiency. Men with true hypogonadism and obesity who are not seeking fertility should be considered for testosterone therapy in addition to lifestyle intervention, since testosterone in these patients results in weight loss, decreased waist circumference and improvements in metabolic parameters (HbA1c, lipids, blood pressure).14
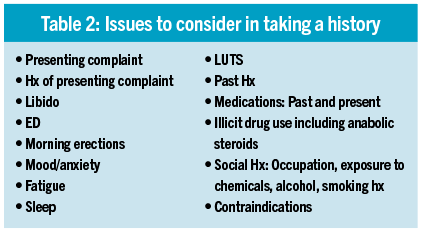
If a man presents with signs/symptoms of testosterone deficiency, a detailed history should be taken. This should include age, fertility concerns (exogenous testosterone reduces sperm production) and sexual history. The clinician must be satisfied that the patient is not seeking treatment for aesthetic purposes, such as bodybuilding (see Table 2).
(click to enlarge)
Testosterone history template
Enquire about previous and current prescription and non-prescription drug use. Assess and exclude systemic illness, ongoing acute disease, malabsorption and malnutrition.11
Each patient should be screened for comorbid conditions such as type 2 diabetes, metabolic syndrome, cardiovascular disease (CVD), erectile dysfunction (this can be a sign of undiagnosed CVD), depression and lower urinary tract symptoms (LUTS). These can all be associated with low testosterone. The most common comorbidities associated with low testosterone are (in order from strongest association to least) – obesity, diabetes, hypertension, hyperlipidaemia and osteoporosis.8
The clinical examination should include measuring body mass index, waist circumference, genital exam, secondary sexual characteristic assessment, checking breast tissue and also a digital rectal exam.9,11
Contraindications to treatment
Contraindications for testosterone treatment are known or suspected prostate cancer, raised haematocrit, raised prostate-specific antigen (PSA), severe obstructive sleep apnoea, severe congestive cardiac failure (CCF), breast cancer, desire to have children, and if using testosterone undecanoate, past or present liver tumours.11
Following the history and physical examination, investigations should be undertaken to determine if the man may have testosterone deficiency.
Initial investigation: Total testosterone
Total testosterone (TT) consists of 60% testosterone very tightly bound to sex hormone binding globulin (SHBG), 38% loosely bound to albumin and 2% free testosterone (FT). Bioavailable testosterone is free plus albumin-bound testosterone, which is 4%. Symptoms of testosterone deficiency correlate more closely with levels of FT.15
Total testosterone involves a fasting sample between 7am and 11am on two separate occasions to rule out acute illnesses:9,11
• TT less than 8nmol/L = testosterone deficiency
• TT 8-12nmol/L, with symptoms = likely testosterone deficiency. Repeat sample in two to four weeks and calculate FT11
• TT 12-35nmol/L = normal.
The aim of the therapy should be to achieve levels in the mid-normal range of 15-30nmol/L.
Follicle-stimulating hormone (FSH), luteinising hormone (LH) and SHBG should be measured if TT is low.16 If LH is high, this would indicate a primary cause. If LH is low/normal then it is likely to be a secondary cause. An MRI brain (pituitary) scan may be considered, especially in cases of profoundly low testosterone, ie. below 5.2nmol/L. Prolactin should also be measured as hyperprolactinaemia will interfere with gonadotropin-releasing hormone and thus reduce testosterone. If prolactin is high consider an MRI of the pituitary gland to assess for a prolactinoma.
SHBG is measured to calculate FT levels. FT can be calculated using the free testosterone calculator available at www.pctag.uk/testosterone-calculator. If FT is less than or equal to 0.225nmol/l, the man is considered to be deficient.
Other investigations
Other investigations include PSA (less than 4), full blood count (haematocrit less than 54%), fasting lipids, fasting blood glucose/HbA1c, renal and liver function tests. It’s very important to assess for obstructive sleep apnoea. Osteoporosis should be considered, particularly if hypogonadism is confirmed.
In summary, if someone presents with signs/symptoms of testosterone deficiency, lab tests indicate a low TT or FT level, and an alternative cause is ruled out, then lifestyle advice is recommended. The patient should aim to optimise exercise, nutrition, sleep and stress management, particularly if there are comorbidities such as type 2 diabetes, metabolic syndrome or obesity. Recent evidence suggests that lifestyle changes in older patients will have limited effects on testosterone production, but it is important for general health and should be integrated into the treatment plan.17
If despite these interventions there is no improvement and other conditions that may present similar to testosterone deficiency are ruled out, then discussion regarding a trial of treatment with testosterone is an option. This is unless the patient wishes to maintain fertility, in which case referral to a specialist for human chorionic gonadotropin (hCG) or selective oestrogen receptor modulator (SERM) treatment is an alternative.
These are off-licence therapies and should only be considered if symptoms are significantly impacting the patient’s quality of life. They may also be an option if the patient is young – under 35 – and/or has a low LH.
Treatment
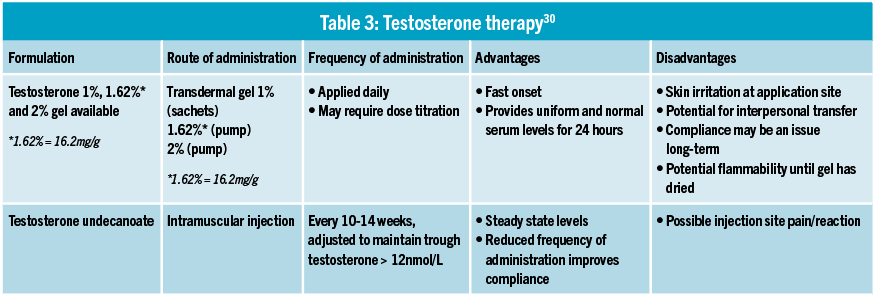
Testosterone preparations are available in two forms in Ireland, transdermal gel and intramuscular (IM) injection. If commencing treatment initially, gel applications are advised due to shorter half-life (see Table 3). Be mindful to inform the patient that there is a small possibility of cross-transfer with the gel applications from hands or clothes.
(click to enlarge)
Care should be taken with gel use around pregnant women and children. Longer-acting IM injections are in the form of an undecanoate with a long half-life and are repeated on average every 10-14 weeks.
Short-term side-effects
• Haematology: Due to stimulation of bone marrow and renal production of erythropoietin there can be occasional polycythaemia/erythrocytosis. The risk is greater for IM injection route than for transdermal administration, as mentioned below, this requires monitoring18
• Gynaecomastia: Very rare and usually reversible
• Testicular atrophy/infertility: Usually reversible with cessation of treatment
• Skin reactions: Common with both transdermal applications and IM injection
• Acne: Can be common.
More information on side-effects and their frequency can be found in the SPC of each product at www.medicines.ie
Follow-up and monitoring
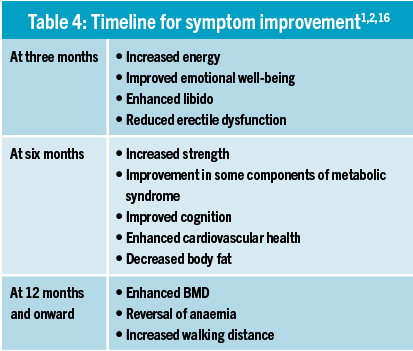
A trial of six months minimum to achieve maximal benefit is advised.19 If symptomatic improvement is not initially seen, prior to stopping therapy, testosterone levels should be checked. In one study it was found that despite treatment with testosterone for hypogonadism, participants had sub-therapeutic testosterone levels < 10.41nmol/L. Dose escalation or switching to a different agent can help as some patients absorb better than others.8 If the patient fails to see a benefit after this (and adherence if on gel application is assessed and not an issue) then discontinue treatment.
Patients should be evaluated at three, six, and 12 months initially (see Table 4) and then every 12 months thereafter to assess serum testosterone levels (therapeutic range 15-30nmol/L), confirm symptomatic improvement, and check for any changes in haematocrit and PSA levels. PSA increases of greater than 1.4ng/ml/year over a one-year period or a velocity of greater than 0.4ng/ml/year over two consecutive years warrants urological evaluation and three-monthly reviews. Haematocrit levels should remain below 54%. Dose adjustments or periodic venesection may be required to achieve this.
(click to enlarge)
Safety of testosterone
Physicians unfamiliar with testosterone therapy may be uncertain regarding its safety in long-term use, particularly around the areas of prostate cancer and CVD. There are no studies demonstrating increased risk of prostate cancer, benign prostatic hyperplasia or LUTS. If a patient already has an underlying undiagnosed prostate cancer, testosterone therapy could stimulate a rise in PSA which, with monitoring as stated earlier, would be picked up early, likely improving the outcome for the patient. Studies have shown no significant increase in PSA following testosterone therapy in hypogonadal men, however regular monitoring is needed to ensure that PSA remains within normal levels.20
Any sign of prostate cancer is considered a contraindication to testosterone therapy. However, there is emerging evidence that challenges this thinking. Recent evidence suggests that this therapy in men with untreated prostate cancer was not associated with prostate cancer progression in the short- to medium-term.21 Larger studies are needed to corroborate these findings.
The effect of testosterone therapy on lipid profile is poorly understood, but most studies show no changes with physiological replacement doses.22
There may be a slight decrease in both total and high-density lipoprotein (HDL) cholesterol, which may affect the total/HDL ratio and may be clinically significant.23
A meta-analysis reviewing adverse effects of testosterone therapy in more than 2,700 men treated for three months to three years found no adverse cardiovascular outcomes, and in fact there are data to suggest that testosterone therapy in men with clinically low testosterone levels is cardioprotective.24,25
Treatment benefits
Aside from symptomatic improvements, evidence has showed that there are benefits in relation to various physiological conditions. Metabolic syndrome and osteoporosis are shown to be of higher prevalence in men with testosterone deficiency, regardless of age.26 It is also known that exogenous testosterone therapy has a favourable impact on body mass, insulin sensitivity and blood pressure.27
Testosterone has a direct effect on glucose metabolism and higher T levels in ageing males are associated with greater insulin sensitivity and a reduced risk of metabolic syndrome.28 It has also been shown that androgens reverse the downward spiral of muscle mass loss and increase of fat mass.
Older men (60-75) at risk of sarcopenia have the same response to the anabolic effects of testosterone as their younger counterparts, ie. skeletal muscle fibre hypertrophy and an increase in size of motor neurons.29
When testosterone therapy was combined with lifestyle advice versus lifestyle advice alone in hypogonadal men with diagnoses of impaired glucose tolerance or newly diagnosed type 2 diabetes, there were significant improvements in HbA1c, muscle mass, fat loss and sexual function in the therapy group after two years.17,19
With the increasing burden of type 2 diabetes, metabolic syndrome and obesity, along with the expected inversion of the population pyramid in coming years, it is wise to bear testosterone deficiency in mind. Those with suggestive signs/symptoms should be screened, particularly those who are older or with comorbidities.
References
Khera M et al. Diagnosis and Treatment of Testosterone Deficiency: Recommendations From the Fourth International Consultation for Sexual Medicine (ICSM 2015). J Sex Med 2016;13:1787-804
Bawor M et al. Testosterone suppression in opioid users: a systematic review and metaanalysis. Drug Alcohol Depend 2015;149:1-9
Morrison D et al. Testosterone levels during systemic and inhaled corticosteroid therapy. Respir Med 1994;88:659-63
Feldman H et al. Age trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts male aging study. J Clin Endocrinol Metab. 2002 Feb; 87(2):589-98
Araujo AB et al. Prevalence of symptomatic androgen deficiency in men. J Clin Endocrinol Metab. 2007 Nov; 92(11):4241-7
Carruthers M et al. Time for international action on treating testosterone deficiency syndrome. Aging Male. 2009 Mar; 12(1):21-8
Traish AM et al. Testosterone Deficiency. Am J Med. 2011; 24(7):578-87
Mulligan et al. Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J Clin Pract. 2006 Jul; 60(7):762-9
Lunenfeld B et al. Recommendations on the diagnosis, treatment and monitoring of hypogonadism in men. Aging Male 2015;18:5-15
Hackett G et al. UK policy statements on testosterone deficiency. Int J Clin Pract 2017 Mar;71(3-4). doi: 10.1111/ijcp.12901. Epub 2017 Mar 20.
Dohle GH et al. Guidelines on Male Hypogonadism. European Association of Urology 2017. Available at: http://uroweb.org/guideline/male-hypogonadism/ (Accessed September 2017)
Dean JD et al. The International Society for Sexual Medicine’s process of care for the assessment and management of testosterone deficiency in adult men. J Sex Med 2015;12:1660-86
British Society of Sexual Medicine. Guidelines on the management of sexual problems in men: the role of androgens 2010. Available at: http://bssm.org.uk/ (Accessed June 2017)
The American Association of Clinical Endocrinologists (AACE) and American College of Endocrinology: 2017 Clinical Practice Guidelines for Comprehensive Medical Care of Patients with Obesity
Antonio L et al. Low Free Testosterone is Associated with Hypogonadal Signs and Symptoms in Men with Normal Total Testosterone. J Clin Endocrinol Metab. 2016 Jul;101(7):2647-57
Hackett G et al. The British Society for Sexual Medicine guidelines on adult testosterone deficiency with statements for UK practice. J Sex Med 2017;14:1504-23
Hackett G et al. Type 2 Diabetes and Testosterone Therapy. World J Mens Health. 2019 Jan;37(1):31-44
Coviello AD et al. Effects of graded doses of testosterone on erythropoiesis in healthy young and older men. J Clin Endocrinol Metab. 2008 Mar; 93(3):914-9
Wittert G et al. Testosterone treatment to prevent or revert type 2 diabetes in men enrolled in a lifestyle programme (T4DM): a randomised, double-blind, placebo-controlled, 2-year, phase 3b trial. Lancet Diabetes Endocrinolo. 2021 Jan; 9(1):32-45
Coward RM et al. Prostate-specific antigen changes and prostate cancer in hypogonadal men treated with testosterone replacement therapy. BJU int. 2009 May; 103(9):1179-83
Morgantaler A et al. Testosterone therapy in men with untreated prostate cancer. J Urol. 2011 Oct;186(4):1559
Rhoden EL et al. Risks of testosterone-replacement therapy and recommendations for monitoring. N Engl J Med. 2004 Jan 29;350(5):482-92
Emmelot-Vonk MH et al. Effect of testosterone supplementation on functional mobility, cognition and other parameters in older men: a randomised controlled trial. JAMA. 2008 Jan 2;299(1):39-52
Fernandez-Balsells MM et al. Clinical review 1: Adverse effects of testosterone therapy in adult men: a systematic review and metanalysis. J Clin Endocrinol Metab. 2010 Jun;95(6)2560-75
Sharma R et al. Normalisation of testosterone level is associated with reduced incidence of myocardial infarction and mortality in men. Eur Heart J. 2015 Oct 21;36(40):2706-15
Blouin K et al. Contribution of age and declining androgen levels to features of the metabolic syndrome in men. Metabolism. 2005; 54(8): 1034-40
Laaksonen DE et al. The metabolic syndrome and smoking in relation to hypogonadism in middle-aged men: a prospective cohort study. Clin Endocrinol Metab. 2005 Feb;90(2):712-9
Muller M et al. Endogenous sex hormones and metabolic syndrome in aging men. J Clin Endocrinol Metab. 2005 May;90(5):2618-23
Bhasin S et al. Drug insight: Testosterone and selective angrogen receptor modulators as anabolic therapies for hronic illness and aging. Nat Clin Pract Endocrinol Metab. 2006 Mar;2(3):146-59
A practical guide on the assessment and management of testosterone deficiency in adult men Based on the 2017 British Society for Sexual Medicine (BSSM) guidelines on adult testosterone deficiency, with statements for UK practice. Accessible at: https://bssm.org.uk/wp-content/uploads/2023/02/BSSM-Practical-Guide-High-Res-single-pp-view-final.pdf
 (click to enlarge)
(click to enlarge)