Across the globe, diabetes caused 1.5 million deaths in 2012 and higher-than-optimal blood glucose caused an additional 2.2 million deaths by increasing the risks of cardiovascular and other diseases. Evidence suggests that many of these deaths (43%) occur prematurely, before the age of 70 years, and are largely preventable.1
While regular screening and patient education are ingredients in managing and reducing type 2 diabetes, implementing lifestyle behaviour changes are perhaps the most influential interventions that can be made. These steps include adopting a healthy diet, increasing physical activity and breaking the sedentary trap, and reducing smoking and alcohol intake. All of these behaviour changes are unequivocally supported in research literature.
Current challenge in health consultations
Nevertheless, when introducing these changes into the health consultation, evidence – including qualitative and observational research – suggests that the patients’ perspectives are not taken into account and that “clinicians often promote or recommend specific treatments rather than consider patients’ preferences during the decision-making process”.2
The challenge for health professionals is to support their patients in adopting and maintaining these complex lifestyle behaviours (and managing positive environments) to help prevent type 2 diabetes and to reduce the impact and prevalence of the condition. However, these behaviours are not easy to implement and maintain, requiring ongoing support, self-monitoring, skills building and most of all an increase in motivation and determination to succeed.
The use of talking therapies to support individuals in making these lifestyle adaptations are increasingly important for health professionals, and evidence-based approaches are now often reported as beneficial. Calls for patient-centred approaches to increase the efficacy of lifestyle and medication self-management have become more prevalent in recent years.
This movement from a medical approach to one that increases the level of engagement and self-responsibility (and self-control) towards change seems like an obvious step and one that has benefits for the individual and health systems alike. Motivational interviewing3 (MI) is one approach that is recommended to be incorporated as a behaviour change technique in diabetes self-management.4
The approach of MI in promoting the person’s ability to self-manage health behaviour change (and medication adherence) has gained support from a range of large-scale reviews and over 530 controlled studies that have now been published on applying MI.
In relation to diabetes specifically, a number of studies have supported the potential efficacy of MI as an intervention in improving glycaemic control and dietary self-care-related confidence in overweight/obese men and women with type 2 diabetes.5
What is MI and how can it help?
Motivational interviewing was first developed as a person-centred approach in the early 1980s, focusing on application in the addictions field. Since then, its impact has been recognised across a range of cessation behaviour settings and even more broadly into lifestyle behaviour change, rehabilitation, probation and corrections to name but a few.
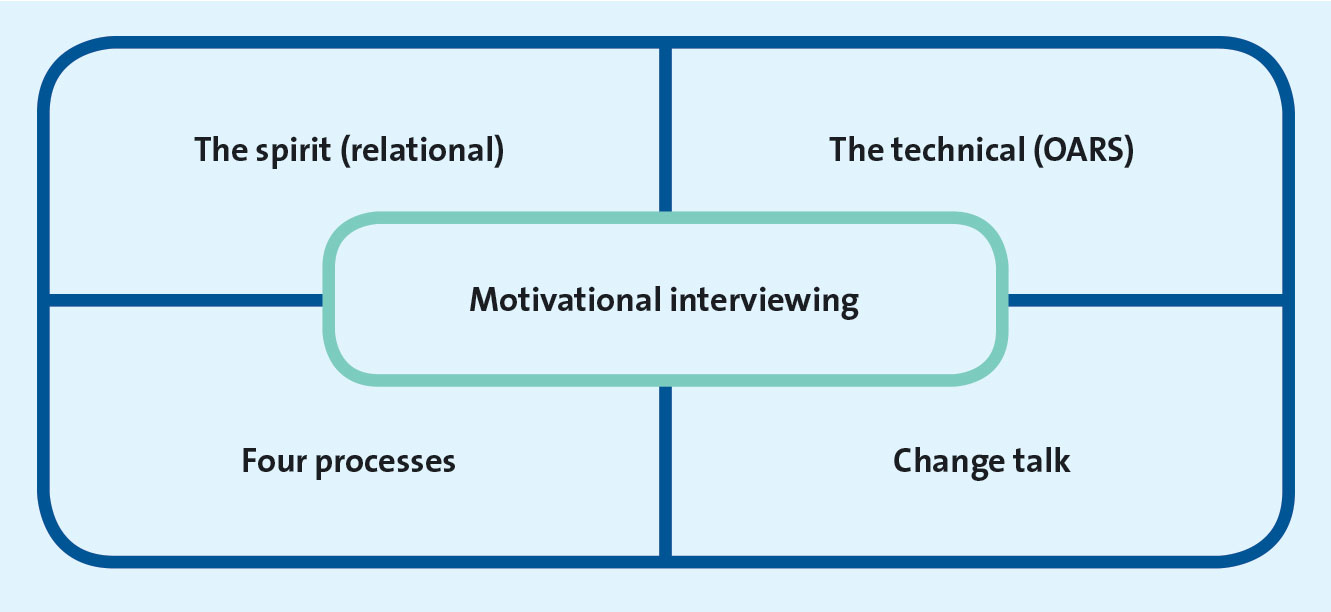
Dozens of books have been published describing its value to children as well as adults, individual and groups settings, in schools, mental health treatment programmes and even sports coaching. Across all of these settings, the approach remains well defined and its core components easily identifiable when delivered with competence (see Figure 1).
(click to enlarge)
In health behaviour change settings, motivational interviewing is focused on developing a collaborative relationship between the health professional and patient in order to explore and resolve ambivalence about changing behaviour. This includes eliciting the patient’s personal perspectives as well as perceived barriers toward change.
The complexity of lifestyle behaviours and medication adherence, and their inter-relationship and influence, usually require an exploration of the issues that the patient feels ambivalent about. Helping the patient better understand the importance of these behaviours, readiness to make the change and confidence toward maintaining those changes is a core approach within an MI conversation.
The underpinning spirit of motivational interviewing is often described as being pivotal to its efficacy, and includes collaboration between the patient and health professional, emphasising empathy rather than sympathy, evoking resources from the individual rather than imposing information and education, and acceptance of their situation rather than judging, blaming or attaching the health professional’s values.3
To operationalise the spirit, the technical (micro) skills of motivational interviewing (OARS) are used and are:
• Open questions
• Affirmations
• Reflective listening
• Summarising.
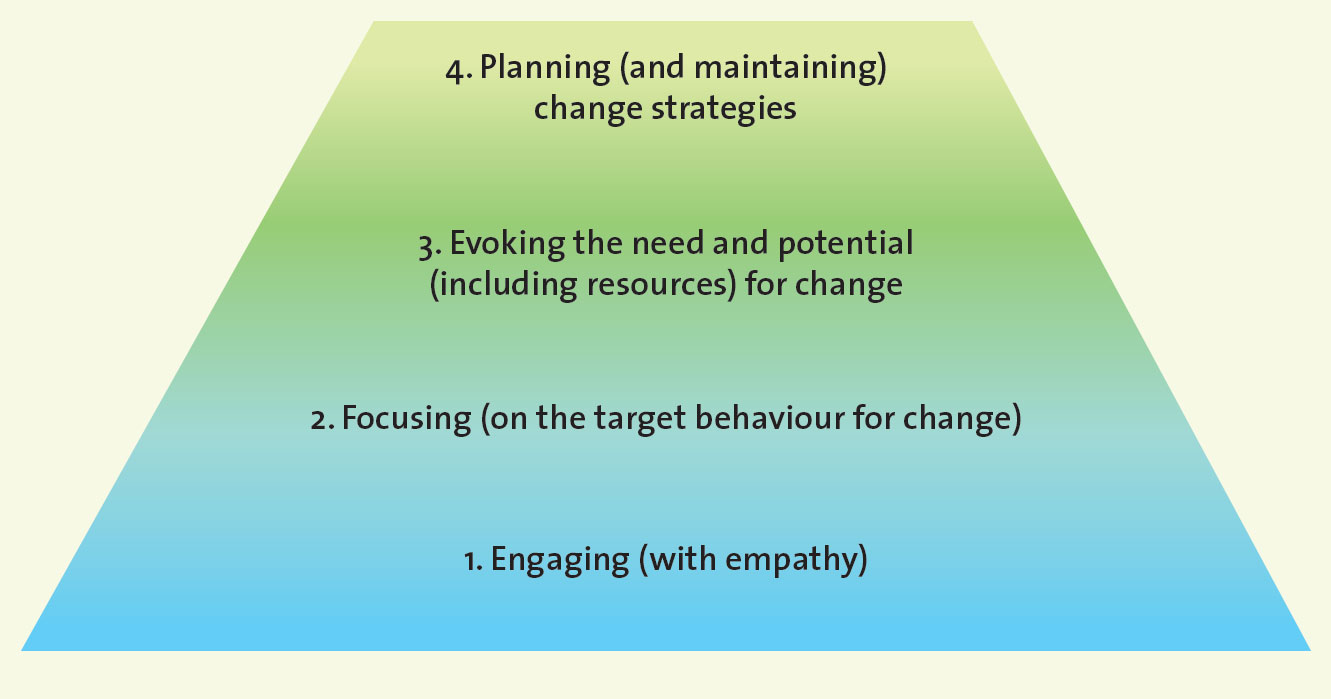
In addition to the spirit and technical components of MI, the approach is also underpinned by the four processes which provide a framework illustrating the direction and progression of clinical sessions: engaging; focusing; evoking; and planning (see Figure 2) and provide a framework around which the practitioner can work strategically and with direction, avoiding a set of communication traps often seen in health settings.
(click to enlarge)
In a diabetes consultation, motivational interviewing is effective in exploring collaboratively patient ambivalence toward specific health behaviours, but perhaps it is most useful in helping first map the priority, or target behaviour, which will be focused upon in the often time-limited health consultation.
Developing clarity in what to focus on and how to implement this change also includes developing strategies for managing relapse and setbacks, which is commonplace when any change is required.6 This includes building patient autonomy and self-determination toward change and unsurprisingly it is the latter which is proposed as the most appropriate theoretical framework to underpin the approach.7
Structure of an MI session in diabetes
For those with diabetes, there is a complex set of health behaviours that require consideration in the avoidance or ongoing management of the condition. In MI sessions, the early stages would include an ‘equipoise’ conversation to clarify past experiences, current attitudes and values of the individual toward change.
This ‘values-matching’ as opposed to ‘stage-matching’ approach is helpful in building engagement in a respectful and non-judgemental style. Using a range of open questions and reflective listening,8 the MI practitioner would help develop a shared picture of the target behaviour(s) and begin to better understand the patient’s ambivalence toward change, not rushing to stamp it out, but rather understand its source and appreciate its impact.
There should be an understanding of how the target behaviour compares to other options. This could include for example, gaining an understanding of the subject’s history of change attempts and perception of personal and practical resources and environments that are missing or require further work.
An important tool commonly used in motivational interviewing is that of scaling rulers. In early phases an ‘importance to change’ ruler (typically 0 = not important; to 10 = essential) could be introduced to gain an insight into the patient’s current position. This helps add clarity between the panoply of potential changes and helps focus toward one priority in the first instance.
As a greater sense of language towards change9 emerges, this can signal a movement to either exploration of decisional balance (the pros and cons of change or status quo) or indeed toward action planning. There is a difference between how important change is and how ready the individual is to do something about the change, and therefore the latter can be explored again using a scaling ruler (0-10) to elicit the readiness language and greater commitment toward action planning.
Once the signs of readiness have emerged in relation to the agreed target behaviour, progression towards action planning can be introduced. In any significant lifestyle change, relapse and setbacks are inevitable6 so there is still a need to maintain vigilance of the signals of ambivalence and reluctance.
In the action planning phase, strategies for managing setbacks should be standard – unfortunately they are not! The action planning phase in motivational interviewing takes account of what previous experiences the individual has had, ideas and resources they have for the next attempt, who will support this change and when they will recognise whether change has been effective. Again, a blend of open questioning, reflective listening and summarising is used in this phase to challenge (with empathy) the individual and to develop their own autonomy toward this lifestyle change.
Ensuring treatment fidelity and delivery
While questions remain over how many of the approximately 530 controlled trials actually delivered motivational interviewing as intended,10 it is clear that when fidelity is ensured, the impact of MI in supporting the autonomy and self-management of lifestyle factors is positive.
There are a number of validated tools available to assess the reliability and consistency of those delivering MI (eg. MITI, MIKAT) and many recent studies of MI training have reported the need for ongoing mentoring and self-reflection as a mechanism for embedding MI skilfulness into practice.11 The aim for trainers and service providers should be to better understand not just the ‘what’ of patient-centred approaches, but also the ‘how’ to deliver it.
Complex behaviours such as physical activity adoption and diet management require active follow-ups as opposed to passive static reviews. They also require action planning and relapse management. Similarly, those delivering talking therapies such as motivational interviewing require ongoing ‘check-ups’ to ensure delivery as intended against recognised criteria.
Reflecting on practice over time can help account for skills ‘drift’ in a similar way that ‘active’ follow-ups with our patients can help manage setbacks and modify change goals.
In conclusion
For several decades there have been calls for approaches that move away from expert-driven, medical models of care in the context of behavioural change and for patients’ values, preferences, and experiences to have a greater emphasis in clinical interactions in an effort to promote patient-centred care.12
Motivational interviewing has been found to be an effective talking therapy which focuses on the individual’s own resources and ability to change, yet it takes practice and skill to use it effectively. Services keen to embed MI should consider how the system can support an approach such as this in a sustained manner with high-quality delivery.
References
World Health Organisation (2016) WHO Global report on diabetes. ISBN 978 92 4 156525
Elwyn G, Dehlendorf C, Epstein RM, et al. Shared Decision Making and Motivational Interviewing: Achieving Patient-Centered Care Across the Spectrum of Health Care Problems. Annals of Family Medicine, 2014; 12(3); 270-275
Miller WR, Rollnick S. Motivational Interviewing: Helping people change. 3rd edition, 2013 Guilford. ISBN 9781462507573
Chen SM, Creedy D, Lin H-S, Wollin J. Effects of motivational interviewing intervention on self-management, psychological and glycemic outcomes in type 2 diabetes: A randomized controlled trial. International Journal of Nursing Studies. 2012; 49: 637-644
Miller ST, Oates VJ, Brooks MA, et al. Preliminary Efficacy of Group Medical Nutrition Therapy and Motivational Interviewing among Obese African American Women with Type 2 Diabetes: A Pilot Study, 2014
Naar-King S, Earnshaw P, Breckon J. Towards a Universal Maintenance Intervention: Integrating Motivational Interviewing with Cognitive-Behavioural Strategies for Maintenance of Behaviour Change. Cognitive and Behavioral Practice, 2013; 27(2): 126-137.
Deci EL, Ryan RM. Self-determination theory in health care and its relations to motivational interviewing: a few comments. International Journal of Behavioral Nutrition and Physical Activity, 2012; 9(24): 1-16
Breckon JD. (2015) Motivational Interviewing to promote physical activity and nutrition behaviour change. In, Doing Exercise Psychology (Anderson M & Hanrahan S, Eds). Human Kinetics, Champaign, Ill. ISBN: 9781450431842
Amrhein PC, Miller WR, Yahne CE, Palmer M, Fulcher L. Client commitment language during motivational interviewing predicts drug use outcomes. Journal of Consulting and Clinical Psychology, 2003; 71(5): 862-878.
Christie, D. & Channon, S. (2014) The potential for motivational interviewing to improve outcomes in the management of diabetes and obesity in paediatric and adult populations: a clinical review. Diabetes, Obesity and Metabolism, 16, 381–387.
Madson MB, Mohn RS, Zuckoff A, et al. Measuring client perceptions of motivational interviewing: factor analysis of the Client Evaluation of Motivational Interviewing scale. Journal of Substance Abuse Treatment, 2013; 44: 330-335
12. Robinson JH, Callister LC, Berry JA, Dearing KA. Patient-centered care and adherence: definitions and applications to improve outcomes. Journal of American Academic Nurse Practitioners, 2008; 20(12): 600-607
 (click to enlarge)
(click to enlarge)