Carpal tunnel syndrome (CTS) affects up to 5% of the population. It may be acute which is usually trauma-related. It may be sub-acute where in the six-to-12-month period following trauma or elective hand surgery, the patient may present with CTS. Most commonly it presents in a chronic state where the most common symptom is paraesthesia or numbness in the distribution of the median nerve. Other symptoms include feelings of clumsiness and weakness in the affected hand, often made worse with activity. The patient will often describe the hand as feeling ‘thick’ or ‘woody’. Typically the symptoms are worse at night, likely due to the flexed wrist position. This often wakes the patient. Pain, which may radiate proximally, is variable.
What is the initial management?
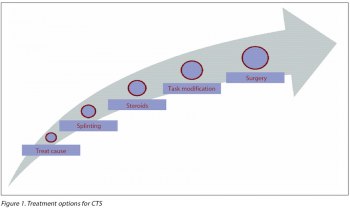
Approximately one-third of patients with carpal tunnel symptoms have associated medical conditions such as inflammatory arthritis, diabetes, pregnancy, amyloidosis, hypothyroidism, acromegaly, to name but a few.1 If possible, treat the underlying cause.
Splinting
An initial trial of full-time splinting with the wrist in neutral for three to four weeks followed by part-time night splinting is recommended.2
Steroid injections
Inject at the level of the proximal wrist crease, on the ulnar side of palmaris longus (absent in around 20%) at a 45° angle aiming for the third web space. Steroids are much more effective given into the carpal tunnel rather than intra-muscularly or systemically.2
Those likely to benefit from splinting or steroids:
• Short-duration symptoms around three months
• Intermittent symptoms
• Absence of clinical findings – numbness, wasting
• Reversible cause.
Steroid injections should be avoided prior to planned electrodiagnostic testing as the presence of steroids may alter test results. In certain cases a steroid injection may be diagnostic.2
Outcome of steroids:
• About one-third of patients are symptom-free at 12 months
• Ten per cent are symptom-free long term.2
Steroid injections and wrist splinting achieve similar results in isolation – the combination of both methods does not improve the outcome.2
Task modification
This reduces metacarpophalangeal joint (MCPJ) flexion and therefore limits lumbrical muscle movement into the carpal tunnel. An ergonomic programme may reduce the incidence of carpal tunnel disease by 60%, eg. adjusting work station height or the angle or diameter of tools and their handles may be effective in controlling the symptoms of CTS. Task modification advice is almost never given.3
(click to enlarge)
When is it time to refer to a surgeon?
Acute CTS should be referred without delay. Persistent median nerve compression, as seen with the more common presentation of chronic CTS, may lead to permanent nerve scarring with motor weakness or sensory loss.
The indications for surgery are when conservative measures have failed, when there is evidence of advanced disease:
• Long-term symptoms, ie. longer than three months
• Persistent numbness in the distribution of the median nerve
• Muscle wasting, ie. abductor pollicis brevis evident in the thenar muscle mass.
What patients are suitable for surgery?
The vast majority of open carpal tunnel releases are done under local anaesthesia.
A suitable patient would be:
• Sufficiently mobile and able to lie on a theatre table
• Co-operative
• Able to tolerate local anaesthesia.
Patients with a likely underlying synovitis, eg. with RA, need a more extensive release and would require a general anaesthetic.
What are the surgical options?
Surgery is the mainstay of treatment giving relief in up to 95% of cases. All surgery releases the transverse carpal ligament on the volar aspect of the wrist. The majority of carpal tunnel releases are open with an incision at the base of the hand. The vast majority of these cases are done under local anaesthesia. A field block to the area with lignocaine or bupivacaine (around 10mls in total) is usually sufficient. A tourniquet is well tolerated by most patients for about 12-15 minutes.
Sutures are removed 10-14 days post-operatively. The other option is endoscopic with can be through one or two ports.4,5 This is done under general anaesthesia. The premise of this is to divide the transverse carpal ligament while leaving the overlying skin intact. The open method remains the gold standard and is the most widely used.5,6
Situations where the problem is in both arms
Fifty per cent of cases are bilateral. The following are risk factors for bilateral disease:
• Female sex
• Obesity (BMI > 30)
• Age 41-60
• Diabetes mellitus
• Square wrists (width = height) as opposed to rectangular.
What can the patient expect after surgery and how should these expectations be managed?
In the absence of complications, the patient can expect almost immediate relief of nocturnal symptoms, in particular, giving the patient a good night’s sleep. The hand is wrapped in a padded dressing allowing full movement of all the fingers at all times. The padded dressing is swapped for a lighter dressing after the first week. Some surgeons use a plaster of Paris splint in the first two weeks.
Recovery can be up to six weeks depending on what type of work the patient does. Sutures are removed at 10-14 days. Following this, the scar is massaged daily for about eight weeks and daily activities are resumed as tolerated.
Existing symptoms such as numbness in the distribution of the median nerve or weakness in the thenar muscles will likely recover to some degree but this is variable both in its timing and extent. If aches and pains were part of the clinical picture, again recovery from this is variable and unpredictable. Releasing the pressure on the median nerve prevents further deterioration in the long term.
Is physiotherapy considered?
Hand therapy is rarely required in the absence of any complications. It may be required if the carpal tunnel compression was as a consequence or co-existing with a condition such as arthritis.
What follow-up is required?
Patients are seen two weeks post-operatively for removal of sutures. Following this, there is a six-week and six-month review.
 (click to enlarge)
(click to enlarge)