Glioblastoma multiforme (GBM) is both the most common and most aggressive primary brain malignancy.1 Despite advances in treatment, prognosis remains poor, with patients surviving an average of 15-18 months from time of diagnosis.2 Given the nature of this malignancy, it is also associated with proportionately high morbidity. There is a slight male preponderance, and the median age at diagnosis is 64 years.3 In Ireland, the average annual incidence of GBM is about 120 cases.1
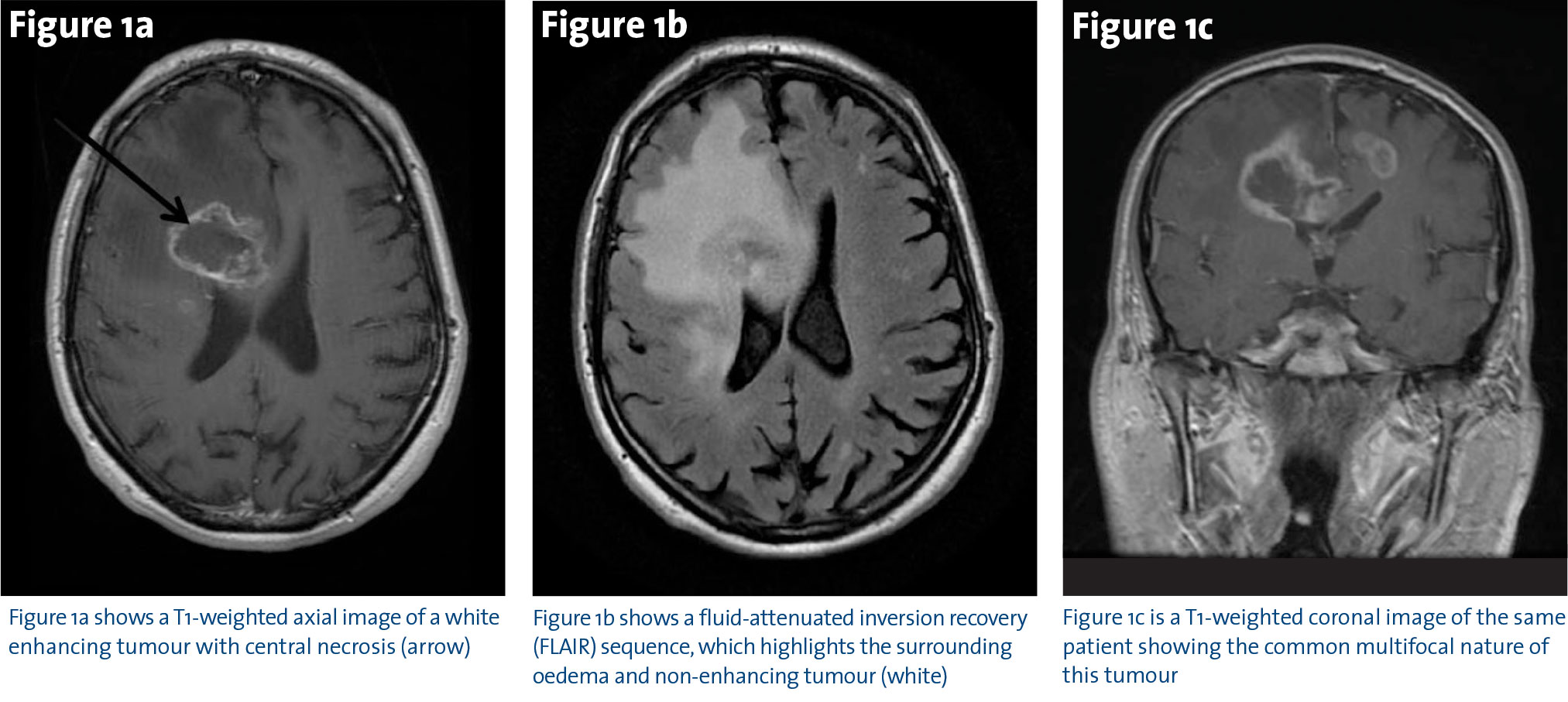
Most patients present with a short history of confusion, headaches and progressive neurological dysfunction depending on the tumour location. Magnetic Resonance Imaging (MRI) is the investigation of choice and typically shows a contrast-enhancing mass (Figure 1a), with extensive tumour-related oedema, which is best seen on Fluid-Attenuated Inversion Recovery (FLAIR) sequences (Figure 1b).
Unlike other malignancies, the clinical outcome for primary brain tumours is less dependent on stage and more closely linked to tumour grade. The World Health Organization grades primary brain tumours from I-IV, and the most recent update now classifies tumours based on histology and molecular biomarkers. Therefore, grade IV tumours or GBMs are now broadly divided into two categories depending on the presence of mutations in the isocitrate dehydrogenase (IDH) enzyme, which is involved in the citric acid cycle.4 IDH-wildtype tumours comprise approximately 90% of cases and generally correlates with de novo GBM, predominately seen in patients over 55 years.4 The IDH-mutant subtype predominantly occurs in younger patients with a history of preceding lower grade glioma.4 Patients whose tumours have mutations in IDH are associated with significantly improved overall survival (OS) irrespective of other prognostic factors (two to three-fold).
The standard course of treatment for GBM in accessible tumours is surgery followed by radiotherapy (RT) and chemotherapy ie. temozolomide. Surgery is usually diagnostic and therapeutic. Maximal resection without neurological compromise is the aim, but many tumours are multifocal (Figure 1c).
(click to enlarge)
The available evidence suggests that aggressive resection is associated with improved functional status and possibly with prolonged survival.5 Most, but not all, observational studies find that extent of resection is a strong prognostic factor in patients with high-grade glioma, even after adjusting for variables known to be related to both surgical decision-making and outcome, such as age, functional status, and tumour size and location.
Adjuvant radiotherapy (RT) has been shown to improve local control and survival after resection, compared with surgery or chemotherapy alone.6 In the past is was noted that older approaches using whole brain RT (WBRT) lead to the highest risk of recurrent high-grade glioma within 2cm of the original tumour site in up to 90%of cases.7 Hence, modern RT fields are usually limited to the tumour site and surrounding area using 60 Gray (Gy) in 30 fractions over six weeks.
Systemic anti-cancer therapy
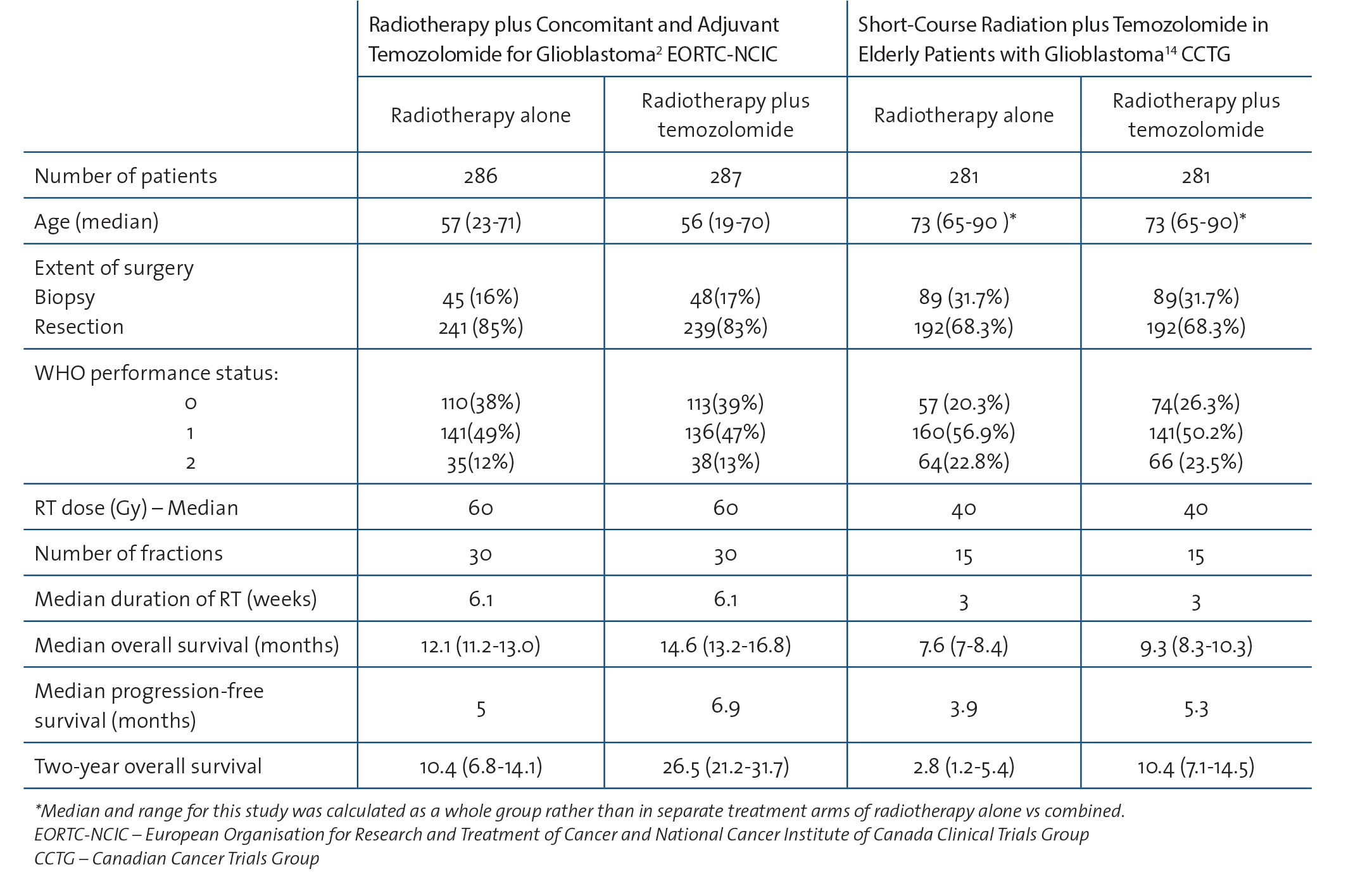
The oral alkylating agent temozolomide (TMZ) has been an integral part of the treatment of GBM for over 10 years. In the pivotal randomised phase III trial conducted by the European Organisation for Research and Treatment of Cancer (EORTC) and National Cancer Institute of Canada Clinical Trials Group (NCIC) there was a 37% relative reduction in the risk of death for patients treated with RT plus TMZ compared with those who received RT alone.2 The study also showed a 2.5-fold increase in the two-year OS, from 10% with RT alone to 27% with radiotherapy plus temozolomide – indicating that a minority of patients derive disproportionately more benefit and have relatively longer survival.2,8
TMZ is given daily, orally, at a dose of 75mg/m2 of body surface area daily during radiation followed by 150mg/m2 daily for five days out of 28 for six cycles. This agent is generally well tolerated and the dose is usually increased to 200mg/m2 from cycle 2. Common side-effects include myelosuppression, constipation and myalgia. Most patients have some fatigue without significant nausea. There is a low risk of alopecia and serious complications such as febrile neutropaenia. Patients with tumours that have hypermethylation of the O6-methylguanine-DNA-methyltransferase (MGMT) gene have improved outcome on average. The MGMT gene encodes for a DNA repair protein, which normally functions by removing alkyl products from the O6 position on guanine. Hypermethylation of MGMT leads to gene silencing and loss of expression of the MGMT protein with a result that malignant cells are less able to repair themselves following DNA damage.9 Methylated MGMT may be a predictive marker of sensitivity to alkylating agents such as TMZ.10
GBM in the elderly
As is the case for many diseases, treatment for the elderly with GBM poses a challenge. Although GBM is predominantly a disease of older people, most clinical trials have generally enrolled younger patients. For example, the pivotal EORTC-NCIC study included only patients with GBM less than 70 years.8
Age is associated with worse OS for several reasons.11,12,13 Firstly, due to their frailty, elderly patients may not be fit for (or offered) intensive therapy. A retrospective analysis of 138 patients between 2006 and 2012 showed a worse performance status in the elderly age group and noted that combination therapy was more commonly given to non-elderly patients (76.8%) than to elderly patients (32.1%, p < 0.0001).12 Hence, there has been a reluctance to offer combination therapy to older patients due to lack of proven benefit and concerns about toxicity.
Against this background, the Canadian Cancer Trials group published an important study in 2017, which showed that TMZ in combination with short course RT (40Gy in 15 fractions) was more effective than short course RT alone in patients 65 years or older.14 The magnitude of this benefit was similar to that seen in the earlier EORTC-NCIC trial (see Table 1). It is apparent that the progression-free survival (PFS) was better in both groups with combination therapy. Although cross-trial comparisons are challenging, it appears, however, that those receiving TMZ plus hypofractioned RT (2017 trial) did less well than younger patients treated with combination therapy in the older trial. This creates some uncertainty about whether to use a longer course of RT (60Gy in 30 fractions) in fitter older patients.
Table 1: Comparison of randomised studies of RT +/- TMZ in GBM(click to enlarge)
Tumour-treating fields
Another entirely novel approach is tumour-treating fields (TTF), which utilises low intensity, intermediate frequency, alternating electric fields to target tumour cells. This requires use of the Novocure device – a cap worn on a shaved head 18-24 hours per day. It has been suggested that this treatment works by interfering with the process of cell division.15 Alternating electric fields arrest cell proliferation in animal tumour models and human brain tumours leading to disruption of cytokinesis in rapidly dividing cells and eventual apoptosis.
A randomised phase III trial showed that TTF alone was equally effective as physician’s choice of chemotherapy in recurrent GBM, but there was improved tolerability and decreased toxicity in the TTF group.16 Following on from this success, the addition of TTF to TMZ-RT was investigated in 315 patients who were newly diagnosed.17 Patients who received TTF with RT-TMZ had a median PFS of 7.1 months compared to 4.0 months in those who received RT-TMZ (p = 0.001). Median OS was also improved: 20.5 months versus 15.6 months (p = 0.004) respectively. This was undoubtedly a major improvement, but wider adoption of this new therapy was been limited by the practical challenges in maintaining scalp electrodes and wearing the device for more than 18 hours a day. To date, this treatment is not yet available in Ireland.
Bevacizumab
For patients with recurrent GBM, there are few established treatments. Bevacizumab is a humanised monoclonal antibody which inhibits vascular endothelial growth factor (VEGF), a crucial mediator in tumour angiogenesis.18 Its effect has been demonstrated in numerous solid malignancies, including cancers of the colon and ovary.19
The use of bevacizumab for recurrent glioblastoma has been predominantly investigated in phase II trials, such as the randomised study published by Friedman et al, which showed promising results for bevacizumab compared to historical controls (median PFS for bevacizumab alone was 4.2 months and median OS 9.2 months).20 One of the main reasons to consider bevacizumab is that it has been associated with stable or decreasing corticosteroid use over time and possible improvements in patients’ quality of life. Following on from this and other smaller phase II trials, bevacizumab was licensed for treatment of recurrent GBM in the US. However, the EU was more cautious; likely because of the modest response rates and lack of phase III data.
Given its target, serious adverse events include haemorrhage and venous thromboembolism; complications to which patients with GBM are particularly vulnerable. The anatomical location of GBM also means that patients who experience intratumoural haemorrhage are likely to experience higher morbidity and mortality, relative to patients with extra-cranial sites of cancer. Interestingly, intracranial haemorrhage occurred in only two (2.4%) patients in the bevacizumab-alone group in a study in 2009 by Friedman et al, which comparing the use of bevacizumab alone versus in combination with irinotecan.20
The optimum dose of bevacizumab has not been defined from randomised trials. In a recent retrospective study in Beaumont Hospital led by Gleeson et al,21 it was found that reduced intensity bevacizumab was associated with similar overall survival to standard dosing. This has important implications for value in cancer care.
Novel agents in GBM
Despite previous lack of success, there remains substantial interest in developing novel agents for the treatment of GBM. We will discuss some of the most pertinent to current practice at present – dendritic cell vaccines, checkpoint inhibitors, BRAF inhibitors and IDH-1 mutation-targeting drugs.
Dendritic cell vaccines
A dendritic cell (DC) vaccine is defined as a dendritic cell loaded with antigens. The first trial of DC vaccines for cancer was published in 1996.22 Peripheral blood mononuclear cells (PBMCs) are commonly used to develop the vaccine,23 and are usually obtained by leukapheresis. DCs are loaded with tumour-associated peptides, whole antigens from DNA or RNA, whole antigen-protein or tumour lysate/whole tumour cells. Dendritic cell maturation is a complex process that occurs in response to proinflammatory cytokines and pathogen-associated molecular patterns (PAMPs). They are then administered to patients in order to induce an antigen-specific T cell mediated anti-tumour response.24 The process is complex and costly.
Dendritic cell vaccines have been successfully employed in other cancer types – for example sipuleucel-T (Provenge) for the treatment of metastatic, castration-resistant prostate cancer.25 Results of ongoing phase II trials of dendritic cell vaccines in GBM are eagerly awaited.
Checkpoint inhibitors
Checkpoint inhibitors, which target programmed death-ligand 1 (PD-L1) have been successfully used in several cancer types. Nivolumab and pembrolizumab are both now used in the treatment of malignant melanoma and lung cancer. PD1 is expressed in the majority of GBMs, suggesting its use as a potential drug target. Despite initially promising results from early trials, in the randomised phase III CHECKMATE-143 trial, nivolumab did not improve OS compared to bevacizumab for GBM.26 Ongoing trials of nivolumab in combination with galunisertib (a kinase inhibitor of TGFβRI) and other agents are being conducted in patients with GBM.27
IDH inhibitors
Mutations in IDH 1 and 2 occur in solid tumours including glioma, and result in production of the oncometabolite 2-hydroxyglutarate (2-HG). This metabolite promotes tumourigenesis. Targeted inhibitors of mutant IDH have already shown promise in patients with IDH-mutant acute leukaemia,28 and are now being investigated in glioma. AG-881 is an oral, potent, brain-penetrant inhibitor of IDH1/2 that reduces 2-HG by up to 98% in glioma models.
As presented at the 2018 annual meeting of the American Society of Clinical Oncology (ASCO),29 this agent appears to have a favourable safety profile at doses < 100mg, and the activity is now being explored in an ongoing perioperative glioma study. The molecular mechanisms of the mutant IDH1 glioma are not fully understood, and the implications of mutant IDH1 inhibition are still a matter of ongoing research.30
BRAF inhibitors
BRAF inhibitors are another area of interest. BRAF is a proto-oncogene with a key role in many cancers, including glioma, and has been successfully targeted in other cancers, particularly in melanoma.31 There have been a number of case series of activity with BRAF inhibitors such as Vemurafenib in GBM.32 A paper in 2016 showed that half the patients with GBM (n = 6 ) had a BRAF mutation and experienced tumour regression with vemurafenib.32 Ongoing research is focussing on novel combinations with better CNS penetration.
EGFR-targeting drugs
Another area of interest in glioma is targeting the epidermal growth factor receptor (EGFR). There is a strong rationale for this, given that this pathway has been shown to be activated in many GBMs. Despite this, agents used in other cancers to target EGFR have been overall disappointing in GBM. Against this background at the recent ASCO meeting in June 2018, the updated results of the INTELLANCE-2 trial were presented. The primary endpoint of this phase II trial was to assess the OS of patients with EGFR amplified GBM when treated with Depatux-M, a tumour-specific antibody-drug-conjugate. This approach allows for toxic chemotherapeutic agents to be released directly into malignant cells upon antibody binding, providing a theoretically more targeted treatment with less systemic side-effects.
Eligible patients were those with EGFR-amplified GBM at first recurrence post-TMZ and this study was open in two sites in Ireland – Beaumont Hospital and Cork University Hospital.33 The latest results show that there was a 40% one-year survival for patients receiving the combination of Depatux-M and TMZ, compared to those who received either TMZ or lomustine alone, who had a significantly lower one-year survival (28%).33 Further results of this study are pending as well as first results for the INTELLANCE-1 study, for newly diagnosed GBM, which was also open in Beaumont.
Conclusion
Glioblastoma is an aggressive primary brain tumour, associated with significant morbidity and limited survival. Radical debulking surgery followed by radiation and the oral alkylating agent temozolomide have improved survival for patients with newly diagnosed tumours. Most patients have disease progression and treatment for recurrent disease is more challenging. However, clinical trials are ongoing to develop novel targeted therapies. In the future it is hoped that a greater access to clinical trials in Ireland will lead to more individualised treatment approaches.
References
National Cancer Registry Ireland. Cancer trends no 28: Primary brain cancer. NCRI, Cork. 2015. Available at: https://www.ncri.ie/sites/ncri/files/pubs/Cancer%20Trends%20-%20Brain.pdf. Accessed 15/8/2018
Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005; 352(10): 987-996
Ostrom QT, Gittleman H, Xu J, et al. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2009-2013. Neuro Oncol 2016; 18(suppl5): v1-v75
Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol 2016; 131(6): 803-820
Sanai N, Berger MSJN. Glioma extent of resection and its impact on patient outcome. Neurosurgery 2008; 62(4): 753-766
Chang C, Horton J, Schoenfeld D, et al. Comparison of postoperative radiotherapy and combined postoperative radiotherapy and chemotherapy in the multidisciplinary management of malignant gliomas. A joint Radiation Therapy Oncology Group and Eastern Cooperative Oncology Group study. Cancer 1983;52(6):997-1007
Ahmed R, Oborski MJ, Hwang M, et al. Malignant gliomas: current perspectives in diagnosis, treatment, and early response assessment using advanced quantitative imaging methods. Cancer Manag Res 2014; 6: 149
Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: Five-year analysis of the EORTC-NCIC trial. Lancet Oncol 2009; 10(5): 459-466
C-H Fan W-LL, H Cao, C Wen, L Chen & G Jiang. O6-methylguanine DNA methyltransferase as a promising target for the treatment of temozolomide-resistant gliomas. Cell Death and Disease 2013: 4: e876
Monika E, Hegi RS. Withholding temozolomide in glioblastoma patients with unmethylated MGMT promoter – still a dilemma? Neuro-Oncology 2015: 1425-1427
Tanaka S, Meyer FB, Buckner JC, et al. Presentation, management, and outcome of newly diagnosed glioblastoma in elderly patients. J Neurosurg 2013; 118(4): 786-798
Morgan E, Norman A, Laing K, Seal MJCO. Treatment and outcomes for glioblastoma in elderly compared with non-elderly patients: a population-based study. Curr Oncol 2017; 24(2): e92
Álvarez de Eulate-Beramendi S, Álvarez-Vega MA, Balbin M, Sanchez-Pitiot A, et al. Prognostic factors and survival study in high-grade glioma in the elderly. Br J Neurosurg 2016; 30(3): 330-336
James R Perry, Normand Laperriere, Christopher J O’Callaghan, et al. Short-course radiation plus temozolomide in elderly patients with glioblastoma. N Engl J Med 2017: 376; 1027-1037
Kiron ED. Alternating electric fields arrest cell proliferation in animal tumor models and human brain tumors. Proceedings of the National Academy of Sciences 2007: 104(24); 0152-10157
R Stupp WE, Kanner AA, Steinberg D, et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomised phase III trial of a novel treatment modality. European Journal of Cancer 2012: 48(14); 2192-2202
Roger Stupp ST, Andrew A Kanner, et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma. Journal of American Medical Association 2015: 314(23); 2535-2543
Beal K, Abrey LE, Gutin PHJRO. Antiangiogenic agents in the treatment of recurrent or newly diagnosed glioblastoma: analysis of single-agent and combined modality approaches. Radiat Oncol 2011; 6(1): 2
Morris PG. Bevacizumab is an active agent for recurrent high-grade glioma, but do we need randomised control trials? Anticancer Drugs 2012: 23(6); 579-583
Friedman HS, Prados MD, Wen PY, et al. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol 2009; 27(28): 4733-4740
Gleeson JP KN, Karadawi N, et al. Reduced-intensity bevacizumab in progressive glioblastoma multiforme (GBM) is associated with similar overall survival versus standard dosing. Paper presented at: Irish Society of Medical Oncology 2017; Dublin
Ridgway DJCi. The first 1000 dendritic cell vaccines. Cancer Invest 2003; 21(6): 873-886
Reichardt VL, Brossart P, Kanz LJBr. Dendritic cells in vaccination therapies of human malignant disease. Mol Ther Methods Clin Dev 2004; 18(4): 235-243
Figdor CG, de Vries IJM, Lesterhuis WJ, et al. Dendritic cell immunotherapy: mapping the way. Nat Med 2004;10(5):475
Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med 2010; 363(5): 411-422
Reardon D, Omuro A, Brandes A, et al. OS10.3 Randomized phase 3 study evaluating the efficacy and safety of nivolumab vs bevacizumab in patients with recurrent glioblastoma: CheckMate 143. Neuro Oncol 2017; 19(suppl3): iii21-iii21
Xue S, Hu M, Iyer V, et al. Blocking the PD-1/PD-L1 pathway in glioma: a potential new treatment strategy. J Hematol Oncol 2017; 10(1): 81
Okoye-Okafor UC BB, Cartier J, et al. New IDH1 mutant inhibitors for treatment of acute myeloid leukemia. Nature Chemistry Biology 2018: 878-886
Ingo K, Mellinghoff MP-P, Katherine B. Peters, et al. Phase 1 study of AG-881, an inhibitor of mutant IDH1/IDH2, in patients with advanced IDH-mutant solid tumors, including glioma. Paper presented at: ASCO Annual Meeting 2018; Chicago, US
Rohle D, Popovici-Muller J, Palaskas N, et al. An inhibitor of mutant IDH1 delays growth and promotes differentiation of glioma cells. Science 2013; 340(6132): 626-630
Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature 2002; 417(6892): 949
Kleinschmidt-DeMasters BK, Aisner DL, Birks DK, et al. Epithelioid GBMs show a high percentage of BRAF V600E mutation. Am J Surg Pathol 2013; 37(5): 685
van den Bent M, Eoli M, Sepulveda JM, et al. LTBK-04 first results of the randomized phase II study on depatux–m alone, depatux-m in combination with temozolomide and either temozolomide or lomustine in recurrent EGFR amplified glioblastoma: First report from Intellance 2/Eortc trial 1410. Neuro-oncology 2017; 19(suppl6): vi316-vi316
 (click to enlarge)
(click to enlarge)