Treatment strategies and survival of older breast cancer patients – a comparison between the Netherlands and Ireland
This article compares treatment strategy and relative survival for operable (non-metastatic) breast cancer in the elderly between The Netherlands and Ireland
Dr Mandy Kiderlen, PhD Student in Surgical Oncology/Geriatric Oncology, Leiden University Medical Center, the Netherlands, Dr Esther Bastiaannet, Epidemiologist, Departments of Oncology and Gerontology and Geriatrics, Leiden University Medical Center, the Netherlands, Dr Paul Walsh, Epidemiologist, National Cancer Registry of Ireland, Cork, Ms Maria B Kelly, Information Technology Specialist, National Cancer Registry of Ireland, Cork, Mr Chris Brown, Biostatistician, National Cancer Registry of Ireland, Cork, Prof Riccardo A Audisio, Surgical Oncologist/Honorary Professor, St Helens Teaching Hospital, University of Liverpool, UK, Dr Olaf M Dekkers, Internist/Postdoctoral Researcher, Department of Epidemiology, Leiden University Medical Center, the Netherlands, Dr Anton JM de Craen, Epidemiologist and Head, Department of Clinical Epidemiology Study Centre, Leiden University Medical Center, the Netherlands, Prof Cornelis JH van de Velde, Professor of Oncological Surgery, Department of Surgery, Leiden University Medical Center, the Netherlands, Dr Gerrit-Jan Liefers, Staff Surgeon, Department of Surgery, Leiden University Medical Center, the Netherlands and Dr Petra G Boelens, Staff Surgeon, Department of Surgery, Leiden University Medical Center, the Netherlands
Currently, about 40% of all new breast cancer cases in developed countries occur among women aged 65 and older.1 Life expectancy is increasing, diagnostic tools become more sensitive and screening programmes are more widely used and expanded. Consequently, the proportion of elderly breast cancer patients is expected to increase in the near future.2
Proper treatment for older breast cancer patients is difficult to define. Older women are frequently excluded from clinical treatment trials because of their age, comorbidity or logistical barriers.3 Moreover, the elderly who are included in trials are probably not representative for the general older population.4 Consequently, an evidence-based treatment strategy for older women with breast cancer is lacking. The only guidance for clinicians is from treatment guidelines that have been validated in younger and healthier women.5 Extrapolation from trials might not be valid since breast cancer biology differs in some respects in older patients, treatment tolerance varies, and there are substantial competing risks of mortality.2,6 Consequently, clinicians have to decide what is best for their patient: treatment according to the guidelines, or patient-tailored deviation from the guidelines.
In the last decade it has become more accepted to use observational data, preferably population-based, to assess treatment effects in older cancer patients.7 However, no strong conclusions can be drawn from these studies as bias due to confounding by indication is likely to be present, since specific (unknown) patient and tumour-related factors influence receipt of particular treatments.8
A recent observational study comparing locoregional treatment between six European countries and the US found that treatment strategy in The Netherlands and Ireland differed considerably on various items among older women with early stage breast cancer, indicating that older patients with early stage breast cancer in Ireland seemed to be slightly under treated, compared with The Netherlands. However, relative survival was not demonstrably different.9
The aim of the present study is to compare treatment strategy and relative survival for operable (non-metastatic) breast cancer in the elderly between The Netherlands and Ireland in more detail.
Materials and methods
Data
From The Netherlands Cancer Registry and National Cancer Registry Ireland (NCRI), all female patients aged 65 years and older diagnosed between 2001 and 2009 with invasive, non-metastasised breast cancer were selected. Tumour stage was defined by TNM classification of malignant tumours.10 Stage data were originally coded using sixth-edition TNM10 rules in the Netherlands and fifth-edition TNM11 rules in Ireland.
Each individual aspect of TNM is termed as a category:
T category describes the primary tumour site
N category describes the regional lymph node involvement
M category describes the presence or otherwise of distant metastatic spread.
Micrometastases (≤ 0.2cm) in regional nodes, classified as N1a in fifth-edition TNM were recoded to N0 for 21 Irish cases to conform to sixth-edition TNM rules. For surgical treatment, only the most extensive surgery registered was used for analysis. Axillary surgery was coded as yes or no.
Primary outcome was treatment strategy by stage. Treatments of interest were type of surgery (none, breast-conserving surgery (BCS), or mastectomy), radiotherapy (RT; yes or no), axillary surgery (yes or no), locoregional guideline adherence (details below), endocrine therapy (yes or no) and chemotherapy (yes or no). Secondary outcome measure was five-year relative survival in each country.
In both the Dutch and Irish breast cancer guidelines, primary surgical treatment with mastectomy or BCS followed by radiotherapy (RT) is recommended for non-metastasised breast cancer. In addition, it is recommended to assess axillary nodal status by performing a sentinel node procedure or axillary lymph node dissection.12,13,14 Therefore, locoregional treatment was considered guideline-adherent when a patient had BCS and RT or mastectomy with or without RT, in all cases followed by any axillary surgical procedure. In addition, the receipt of systemic therapy (adjuvant endocrine therapy and chemotherapy) was analysed.
Although routine cancer registry data on endocrine therapy in Ireland is known to be incomplete (National Cancer Registry of Ireland, unpublished data), because of difficulties associated with outpatient prescription of the drugs involved, linkage to a national database of drug prescription identified additional endocrine therapy for 21% of patients.
Linkage was not possible for about 15% of Irish patients, and for this group, ‘missing’ endocrine therapy was imputed (4% of all patients).
Data from both The Netherlands Cancer Registry and the NCRI are fully anonymised prior to being made available to researchers, therefore, no informed patient consent was required and there was no need for ethical committee approval.
Mortality follow-up was available to December 31, 2011 by linkage of cancer registry with national mortality data.
Statistical analyses
Analyses were performed in IBM SPSS Statistics 20 and Stata SE 12. Treatment strategies were analysed and grouped by tumour stage (I to III).
Differences in treatment between countries were tested by a Poisson regression model, adjusted for age (continuous), histological subtype, tumour grade, ER and PR status.
Relative survival was calculated by the Ederer II method.15 National life tables for each country were used to estimate expected survival. Results were presented as percentage relative survival after five years, and Relative Excess Risks (RER) derived from relative survival modelling, with The Netherlands as reference category.16
Results
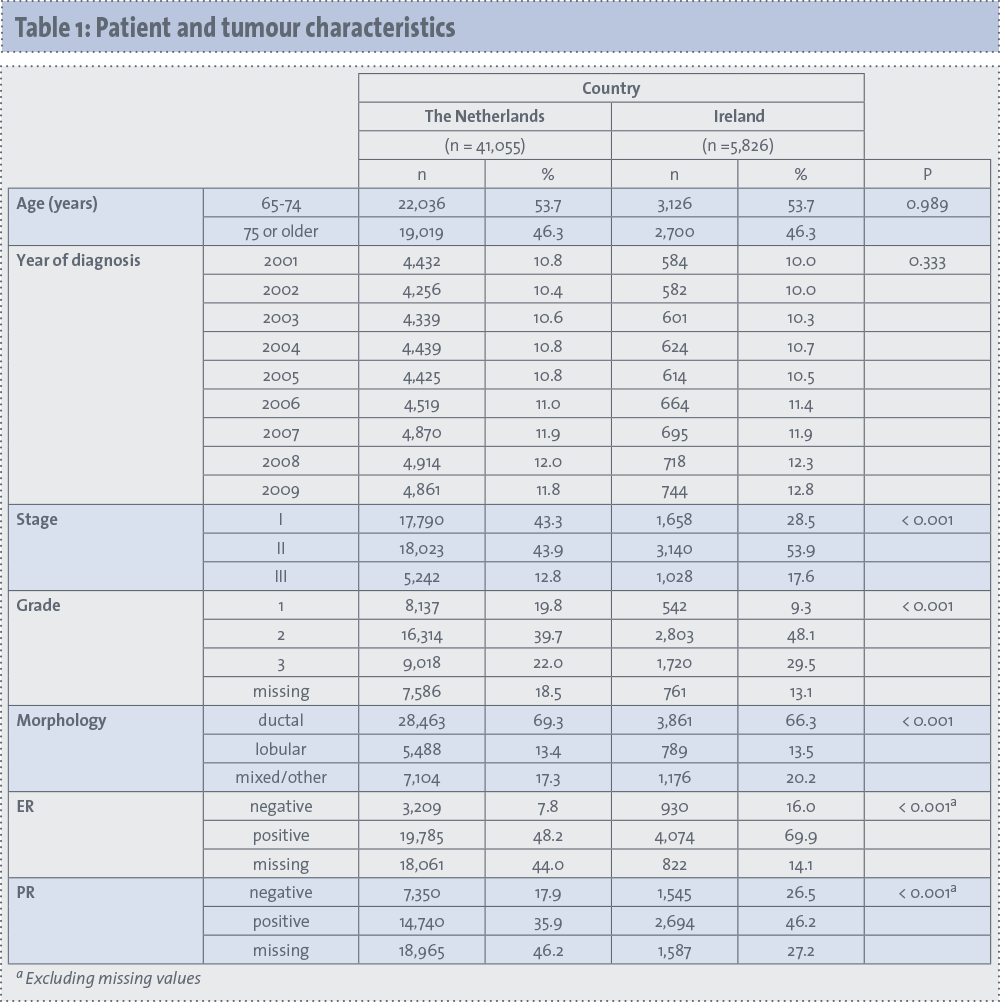
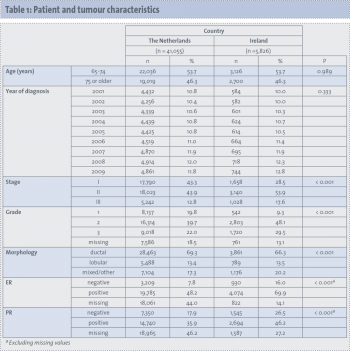
Overall, 41,055 patients from The Netherlands and 5,826 patients from Ireland were included. Patient and tumour characteristics are shown in Table 1. Median age for patients in The Netherlands was 74 years (range 65-102), and in Ireland 74.2 (range 65-99). Fewer early-stage tumours and more with advanced stage were observed in Ireland (p < 0.001). Recorded grade distribution differed significantly, with a higher proportion of higher grades in Ireland than in The Netherlands (p < 0.001).
(click to enlarge)
Hormone receptor status showed smaller differences, with slightly smaller proportions of oestrogen and progesterone receptor-positive tumours among Irish patients (81% and 64%, respectively, excluding missing or unknown values) compared with those from The Netherlands (86% and 67%; p < 0.001).
Locoregional treatment
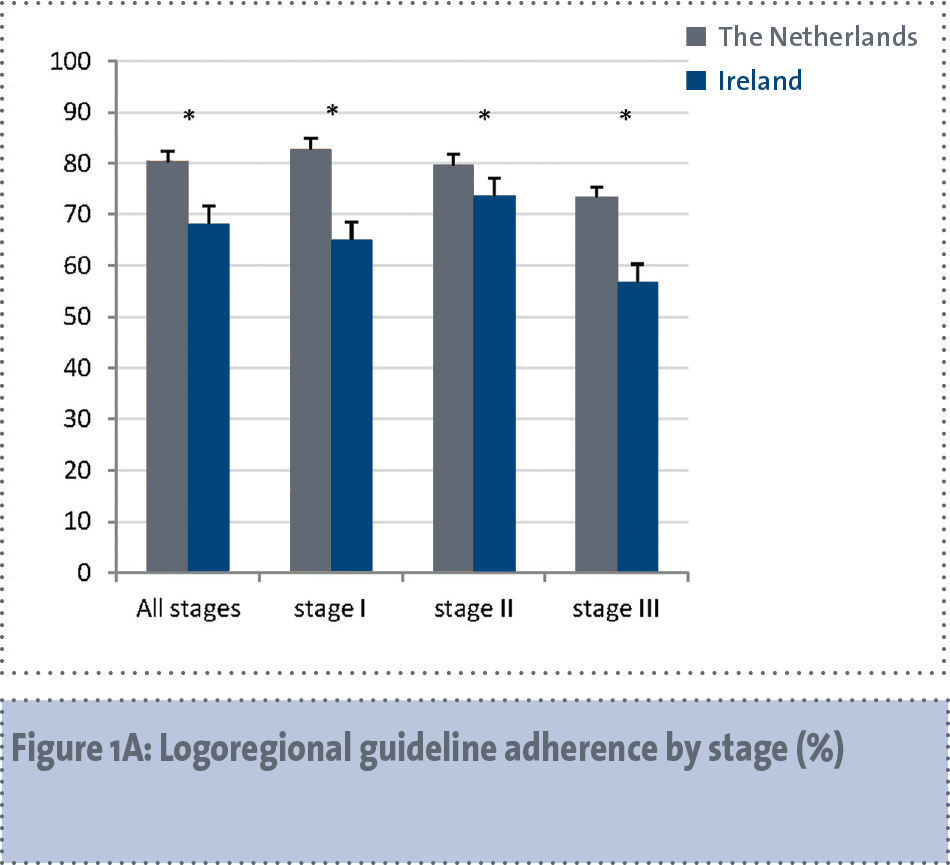
Figure 1A shows the proportions of patients receiving guideline-adherent locoregional treatment by country, grouped by stage. In The Netherlands, guideline-adherent treatment was performed in 80% with little variation between stages, whereas these proportions in Ireland ranged from 57% (stage III) to 74% (stage II).
(click to enlarge)
(click to enlarge)
(click to enlarge)
(click to enlarge)
Among patients who did not receive guideline-adherent locoregional treatment, 65% (The Netherlands) and 68% (Ireland), had no locoregional treatment at all, 6% (The Netherlands) and 13% (Ireland) had only BCS (without RT or axillary surgery), and 29% (The Netherlands) and 20% (Ireland) had adequate local treatment, but no axillary surgery.
Adjusted RRs for having guideline-adherent locoregional therapy in Ireland relative to The Netherlands were 0.79 (95% CI 0.76-0.81), 0.87 (0.85-0.89) and 0.72 (0.68-0.75) respectively for stage I, II and III (p < 0.001 for all stages).
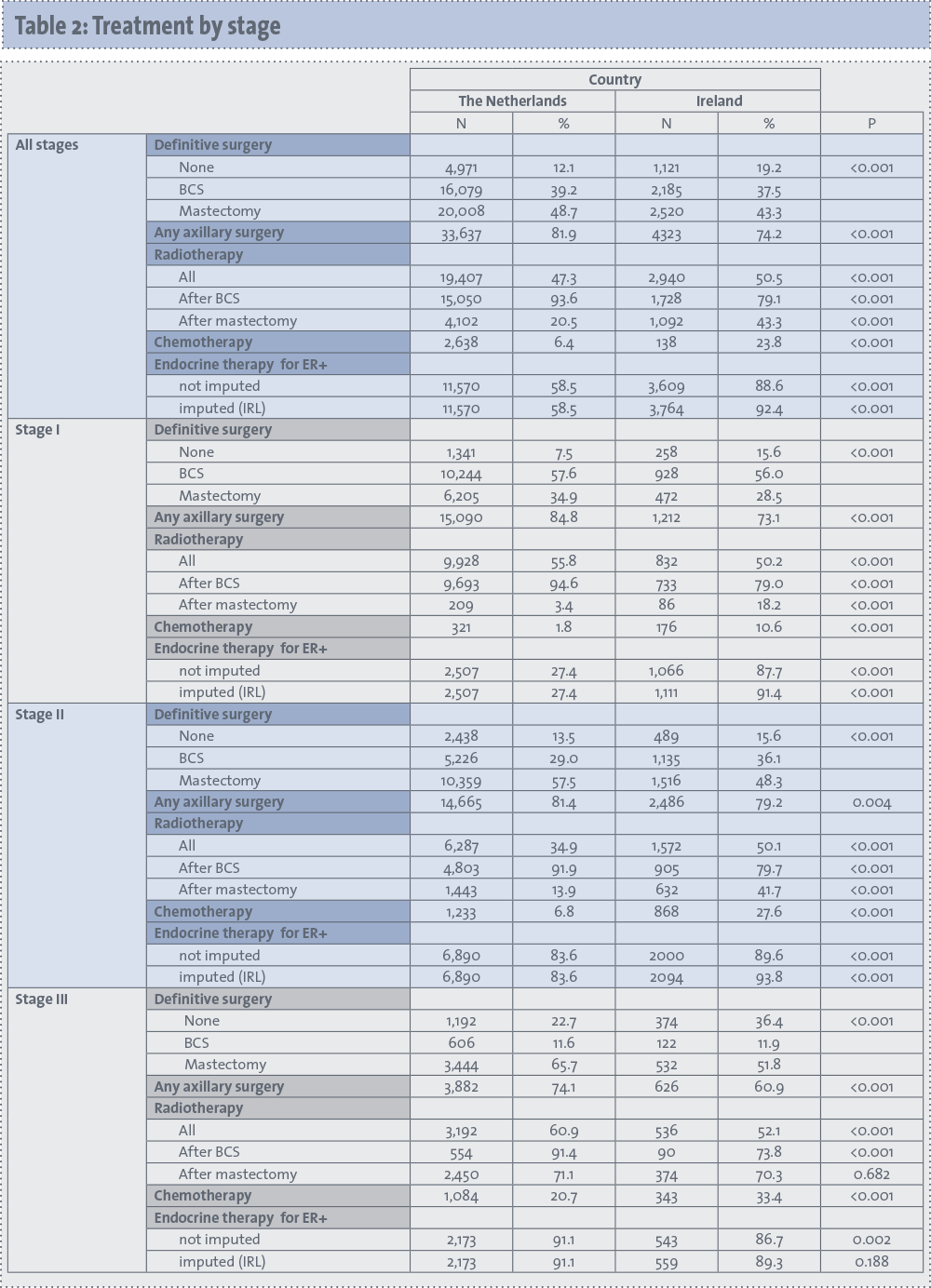
Looking more specifically at locoregional treatment (see Table 2), overall, more patients in Ireland had no breast surgery at all (19% versus 12% in The Netherlands), also stratified by stage (p < 0.001 in all stages).
(click to enlarge)
In The Netherlands, 82% underwent any axillary surgical procedure, as compared to 74% in Ireland. Also, in all three stage groups, fewer patients in The Netherlands than in Ireland did not undergo axillary surgery (p < 0.001).
Regarding radiotherapy (RT), among all patients, more patients received RT in Ireland than in The Netherlands, overall and after mastectomy (p < 0.001). For mastectomy patients, the difference was only seen in stage I (18% of patients had post-mastectomy RT in Ireland versus 3% in The Netherlands) and stage II (42% versus 14%; p < 0.001). In stage III patients, the difference in the receipt of RT attenuated and no difference was observed in post-mastectomy RT. However, in all stages, significantly fewer patients in Ireland received RT after BCS (79% versus 94% in The Netherlands, overall, p < 0.001).
Endocrine therapy
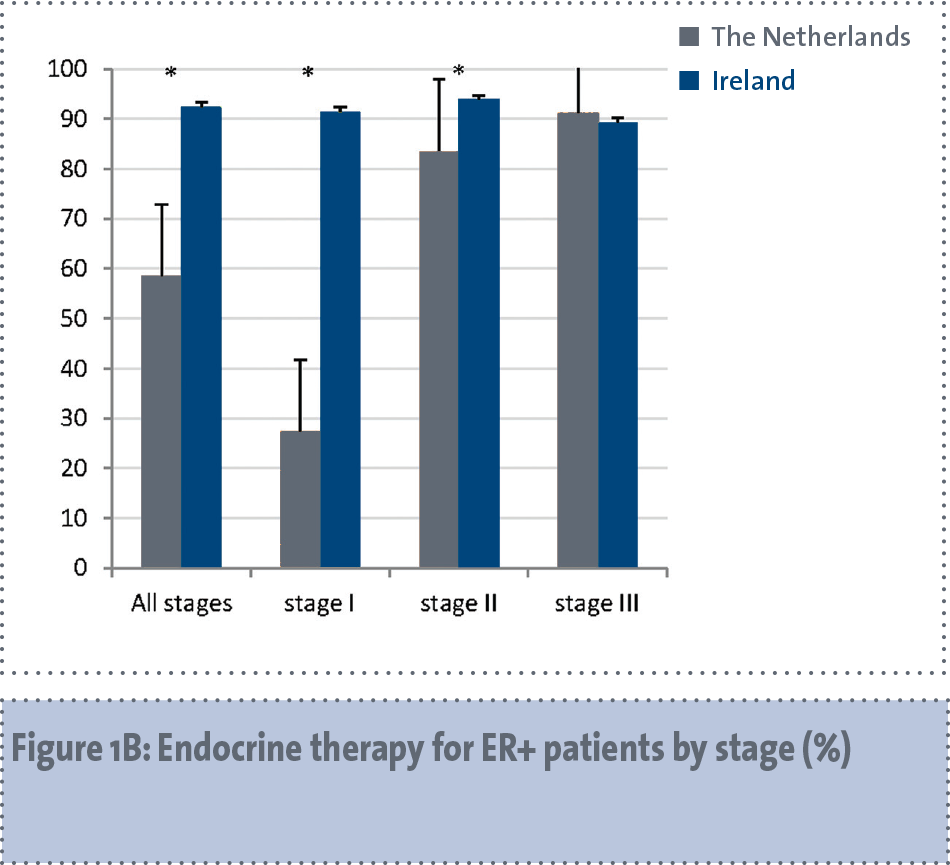
The overall proportion of oestrogen receptor-positive patients receiving endocrine therapy differed between the countries – 59% in The Netherlands versus 92% in Ireland (p < 0.001) for all stages combined. Patients with stage I disease were more than three times as likely to get endocrine therapy in Ireland (91% versus 27%; p < 0.001). The difference was smaller in stage II patients, 94% in Ireland versus 84% in The Netherlands (p < 0.001), and 89% versus 91% respectively in stage III patients (p = 0.188).
Adjusted RRs for having endocrine therapy in Ireland were 2.91 (95% CI 2.77-3.05), 1.11 (1.09-1.12) and 0.99 (0.96-1.02) respectively for stage I, II and III ER-positive patients. Among patients who did not receive any locoregional treatment at all, the proportions of endocrine monotherapy were 85% in The Netherlands and 86% in Ireland.
Chemotherapy
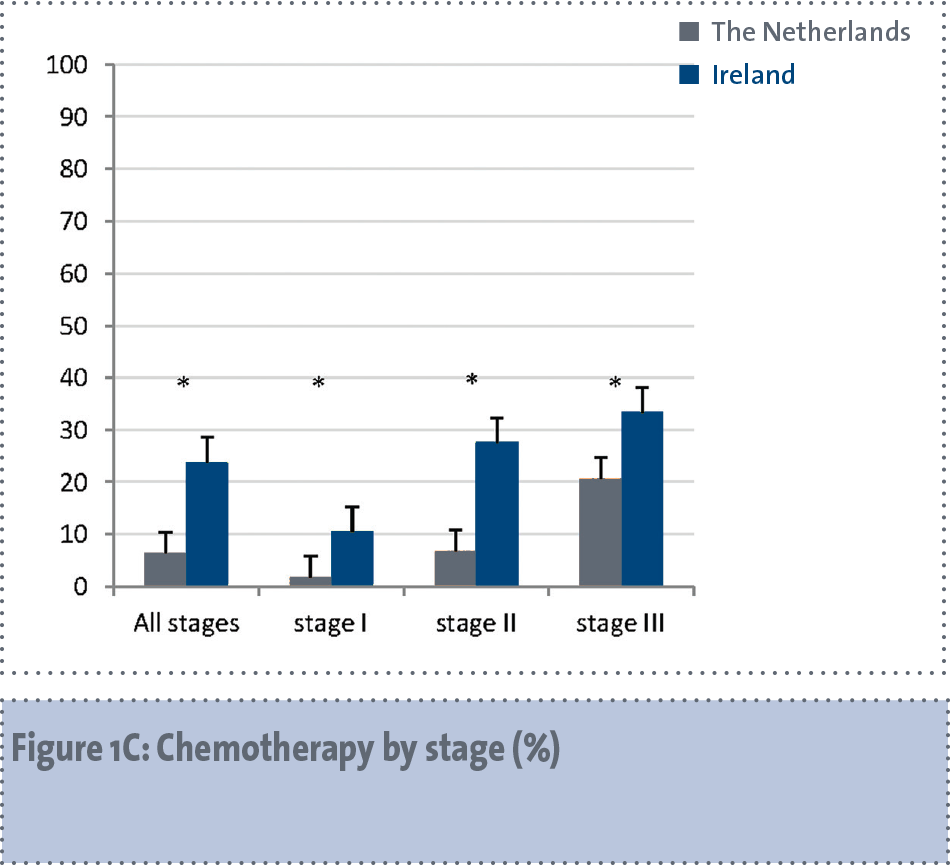
Overall, 6% of patients in The Netherlands and 24% of patients in Ireland received chemotherapy, and there a higher proportion of Irish patients received chemotherapy in all three stages (p < 0.001). Adjusted RRs for having chemotherapy in Ireland were 4.55 (95% CI 3.81-5.43), 3.35 (3.11-3.62) and 1.44 (1.31-1.58), respectively for patients with stage I, II and III.
Relative survival
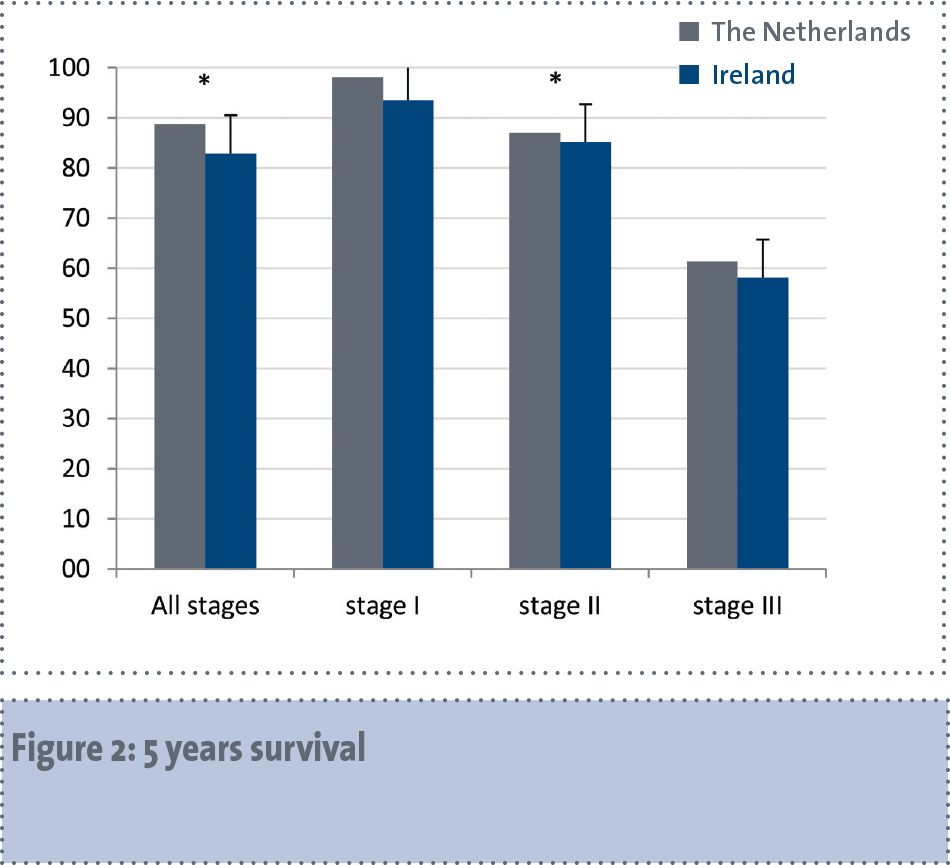
Median follow-up time was 4.5 years for The Netherlands and 4.3 years for Ireland. During the total follow-up period, 14,771 (36.0%) patients died in The Netherlands, compared to 2,191 patients (37.6%) in Ireland.
Five-year relative survival was 88.8% in The Netherlands and 82.9% in Ireland, for all stages combined (see Figure 2). This survival difference was statistically significant, also after adjustment for age, grade, stage, ER, PR and morphology (relative excess risk [RER] for Ireland, with The Netherlands as reference category: 1.22; 95% confidence interval (CI) 1.10-1.36). Grouped by stage, no survival difference was demonstrated in stage I patients (adjusted RER 1.00, 95% CI 0.59-1.70), but worse survival was confirmed for Irish patients in stage II (adjusted RER 1.20, 95% CI 1.02-1.42) and stage III (1.20, 95% CI 1.04-1.39).
Discussion
The current study, comparing treatment and relative survival of older breast cancer patients between two Western European countries with similar treatment guidelines, showed large differences in treatment approach for older breast cancer patients. A higher proportion of patients in The Netherlands received guideline-adherent locoregional treatment than in Ireland in all stages, but in Ireland the receipt of systemic treatments was higher in all stages of disease. Relative survival of patients in Ireland was significantly poorer than in The Netherlands, but adjusted models suggested the difference most marked for stage II and III patients.
The observed discrepancies in breast cancer treatment are consistent with findings of earlier international comparisons of older and other breast cancer patients across Europe and the US.9,17,18,19 Although international survival and treatment variations among breast cancer patients have recently been assessed on a global scale,20 no clear evidence was published on the potential role of different treatment strategies in influencing survival discrepancies among early-stage cases. However, it is interesting to speculate on reasons for the differences in patterns of care for the specific treatment modalities.
Some differences could be explained by discrepancies in guideline recommendations between the two countries. There are differences especially for post-mastectomy radiotherapy and chemotherapy, and for both of these, indications are broader in the Irish guidelines. These differences are reflected in our results, where we observed more patients from Ireland receiving these treatments, as compared to the patients from The Netherlands, also stratified by stage of disease. Secondly, physicians from The Netherlands may also be more likely to deviate from the guidelines when treating older breast cancer patients. Unfortunately, in our study it was also not possible to draw any reliable conclusion about the impact of differences in any of the specific treatment modalities, because of a potential bias due to confounding by indication when comparing the outcomes of patients with different treatments directly.
In a large population-based study in The Netherlands, guideline adherence of breast cancer treatment among younger and older breast cancer patients was compared between different regions, and although differences in adherence were observed, there were no significant survival differences between regions.21 In the current study we found less guideline-adherence on locoregional treatment in Ireland, and this was accompanied by a worse survival in Ireland. On the other hand, patients in Ireland received more systemic therapies (both endocrine therapy and chemotherapy), so no conclusion can be drawn based on the locoregional treatment only, because of a probably counterbalanced effect by adjuvant treatments.
To obtain the highest level of evidence on treatment benefits, the effect of each treatment modality should be investigated based on randomised assignment of treatment. However, randomised clinical trials (RCTs) tend to be slow, expensive, and insensitive to the heterogeneous contexts of the general population.22 The disadvantages of RCTs are probably even stronger in the older population, because of their limited mobility and large heterogeneity. Observational studies, using population-based registry data, are considered to be a better reflection of the ‘real world’.5,23 Although large study populations can be derived from registries, the observational design means that confounding by indication must be considered when studying treatment effects.
A limitation of our study was that the selected populations differed in some respects. Advanced stage and higher-grade cases were more frequently observed in Ireland. Although the analyses included patients aged 65 and older, this finding might be explained partly by differences in screening24,25 and possibly methods of grading between countries.
To achieve best practice for older breast cancer patients, possibly, attention should be shifted to other outcomes rather than survival to improve quality of care for this patient group. However, we could draw no conclusions on aspects such as quality of life, risk of recurrence or complications, as we did not have data on these aspects. In addition, due to full anonymisation of the datasets in this study, we were unfortunately not able to see if guideline-adherence was associated with hospital characteristics, such as the type (academic/teaching hospital, private/public clinic), and the presence of radiotherapy facilities.
The European Registration of Cancer Care or, in short, European Cancer Audit (EURECCA), aims to create a population-based audit structure that covers all breast cancer patients across Europe: anonymous patient and tumour data, including treatment and outcome information will be registered in a uniform way across countries, with the ultimate goal of defining high-quality care and monitoring the quality of care of all European cancer patients and so improving outcome of cancer care. EURECCA aims to investigate best practices and learn from them, as well as perform analysis on patient groups that deviate from guidelines such as the young and elderly.
In conclusion, in this population-based study comparing patterns of care and survival of older breast cancer patients on a national scale in The Netherlands and Ireland, we found large differences in treatment approach, with more guideline-adherence on locoregional treatment in The Netherlands, and more prescription of systemic therapy in Ireland.
Patients in Ireland had a worse relative survival as compared with the Dutch patients, although it was not possible to link this survival difference directly to differences in one or more of the specific treatment modalities. However, our finding should be a strong recommendation to perform more research on an international scale, with the ultimate goal to equalise the survival rates for breast cancer patients across Europe.
This article is adapted with permission from: Treatment Strategies and Survival of Older Breast Cancer Patients – An International Comparison between the Netherlands and Ireland. PLoS ONE 2015; 10(2): e0118074.
References
Wildiers H, Kunkler I, Biganzoli L, et al. Management of breast cancer in elderly individuals: recommendations of the International Society of Geriatric Oncology. Lancet Oncol 2007; 8: 1101-1115.
Biganzoli L, Wildiers H, Oakman C, et al. Management of elderly patients with breast cancer: updated recommendations of the International Society of Geriatric Oncology (SIOG) and European Society of Breast Cancer Specialists (EUSOMA). Lancet Oncol 2012; 13: e148-e160.
Townsley CA, Selby R, Siu LL. Systematic review of barriers to the recruitment of older patients with cancer onto clinical trials. J Clin Oncol 2005; 23: 3112-3124.
van de Water W, Kiderlen M, Bastiaannet E, et al. External validity of a trial comprised of elderly patients with hormone receptor-positive breast cancer. J Nat Cancer Inst 2014; 106: dju051.
Al-Refaie WB, Vickers SM, Zhong W, et al. Cancer trials versus the real world in the United States. Ann Surg 2011; 254: 438-442.
Mieog JS, de Kruijf EM, Bastiaannet E, et al. Age determines the prognostic role of the cancer stem cell marker aldehyde dehydrogenase-1 in breast cancer. BMC Cancer 2012; 12: 42.
Vandenbroucke JP. When are observational studies as credible as randomised trials? Lancet 2004; 363: 1728-1731.
Altman DG, Bland JM. Statistics notes. Treatment allocation in controlled trials: why randomise? BMJ 1999; 318: 1209.
Kiderlen M, Bastiaannet E, Walsh PM, et al. Surgical treatment of early stage breast cancer in elderly: an international comparison. Breast Cancer Res Treat 2012; 132: 675-682.
Greene FL, Page DL, Fleming ID. AJCC cancer staging manual, 6th ed. New York: Springer, 2002.
Fleming ID, Cooper JS, Henson DE, et al. AJCC Cancer Staging Manual, 5th ed. Philadelphia, PA: Lippincott-Raven, 1997.
CBO. Richtlijn Behandeling van het mammacarcinoom 2005.
O’Higgins N. National Quality Assurance Standards for Symptomatic Breast Disease Services – Developing Quality Care for Breast Services in Ireland. Dublin, Ireland: Health Information and Quality Authority, 2007.
Walsh TN, O’Higgins N. Breast Cancer Management Clinical Guidelines. Dublin, Ireland: Royal College of Surgeons in Ireland, 2000.
Hakulinen T, Seppa K, Lambert PC. Choosing the relative survival method for cancer survival estimation. Eur J Cancer 2011; 47: 2202-2210.
Dickman PW, Sloggett A, Hills M. Regression models for relative survival. Stat Med 2004; 23: 51-64.
Allemani C, Storm H, Voogd AC, et al. Variation in ‘standard care’ for breast cancer across Europe: a EUROCARE-3 high resolution study. Eur J Cancer 2010; 46: 1528-1536.
Garcia-Etienne CA, Tomatis M, Heil J, et al. Mastectomy trends for early-stage breast cancer: a report from the EUSOMA multi-institutional European database. Eur J Cancer 2012; 48: 1947-1956.
van Nes JG, Seynaeve C, Jones S, et al. Variations in locoregional therapy in postmenopausal patients with early breast cancer treated in different countries. Br J Surg 2010; 97: 671-679.
Allemani C, Sant M, Weir HK, et al. Breast cancer survival in the US and Europe: A CONCORD high-resolution study. Int J Cancer 2013; 132(5): 1170-81.
van de Water W, Bastiaannet E, Dekkers OM, et al. Adherence to treatment guidelines and survival in patients with early-stage breast cancer by age at diagnosis. Br J Surg 2012; 99: 813-820.
Sullivan P, Goldmann D. The promise of comparative effectiveness research. JAMA 2011; 305: 400-401.
Dreyer NA, Garner S. Registries for robust evidence. JAMA 2009; 302: 790-791.
RIVM. Bevolkingsonderzoek Borstkanker. 2012.
National Cancer Screening Service. The National Breast Screening Program, 2012.
 (click to enlarge)
(click to enlarge)