Unique quality of life issues in rural dwelling colorectal cancer survivors in Ireland
Colorectal cancer survivors face many issues on their cancer journey, often compounded by distance from servcies
Ms Audrey Alforque Thomas, Postdoctoral Research Fellow, Health Promotion Research Centre, NUI, Galway, Prof Pamela Gallagher, Senior Lecturer in Psychology, School of Nursing and Human Sciences, Dublin City University, Dublin, Mr Alan O’Céilleachair, Lecturer, Centre for Policy Studies, University College Cork, Cork, Ms Alison Pearce, Postdoctoral Research Fellow, National Cancer Registry Ireland, Cork, Ms Linda Sharp, Epidemiologist, National Cancer Registry Ireland, Cork and Mr Michael Molcho, Lecturer, School of Health Sciences, NUI Galway
How far colorectal cancer patients live from medical services is associated with their clinical outcomes. Increasing distance to a hospital or to their general practitioner (GP) is associated with later stage at diagnosis of colorectal cancer,1,2 lower likelihood of receiving treatment,3,4 reduced likelihood of attending a specialist centre,4,5 and shortened survival.6,7 The association of remoteness from hospital with clinical outcomes is well-documented; however, the association with patient-reported outcomes is less well understood. A recent study of long-term colorectal cancer survivors in Australia showed a negative relationship between remote residence and cancer-specific quality of life (QoL), but remoteness was not the focus of their study.8 More research investigating how distance to hospital is related to colorectal cancer survivors’ QoL is needed.
In addition to QoL disparities by remoteness from hospital, disparities by gender have been noted in relation to colorectal cancer survivors. However, the evidence base is limited and inconsistent. Some studies report no gender difference in psychological or social QoL.9,10 A study of rural US cancer patients, including those with colorectal cancer, found that women had a higher total QoL than men.11 Other research suggests that female colon cancer survivors report more physical functioning concerns than male survivors.12
Study objectives
Two conceptual frameworks that may inform the study of remoteness and QoL are the stages of cancer survivorship and distance decay. Mullan’s13 model of cancer survivorship, created 30 years ago, is still used14 to conceptualise the three seasons or stages of cancer. The acute stage encompasses diagnosis and treatment. The extended stage refers to remission or completion of treatment. These first two stages rely on specialised oncology care. The permanent stage is marked by reduced likelihood of cancer recurrence and the movement toward GPs, primary health providers, and community hospitals.15
Distance decay, that interactions between two entities decreases with distance,16 has been applied to distance to hospital and patient healthcare utilisation.17 The relationship between distance from hospital and the first two stages (acute and extended) of cancer survivorship are very clear: those patients who live remote from the treating hospital have less advantageous clinical outcomes. Less well understood is how the survivor in the permanent stage might be impacted by distance from treating hospital.
In this study, we investigate how remoteness from hospital is related to the QoL of colorectal cancer survivors in the permanent stage, and if there are gender differences in the relationship between remoteness from hospital and QoL.
Methods
Setting
This study was conducted in Ireland, which has a relatively low population density at 66 people per square kilometre. For comparison, the population density the United Kingdom is 259 people per square kilometre. Ireland’s 4.6 million people are spread over more than 70,000km2, suggesting that Irish cancer patients may have to weigh the convenience of a local hospital with the perceived quality of a high-volume cancer centre, as others have done in different settings.18,19
Tumour-directed treatment of colorectal cancer patients is increasingly available in local Irish hospitals by high-volume practitioners. From 2000 a decreasing percentage of colorectal cancer patients were travelling for surgery. At the same time, a greater proportion of surgeries were performed by surgeons with high case volume, which has been shown to improve clinical outcomes. Similarly, radiotherapy has become increasingly available outside of Dublin and Cork.20 Supportive care in the permanent stage of cancer is only briefly addressed in the National Cancer Control Strategy; however, the intention is to encourage local supportive care separate from the Specialist Cancer Centres.21
Design and participants
In March 2010, survivors of primary, invasive colorectal cancer (ICD-10 C18-C20) were identified in the National Cancer Registry. Individuals were included if they were diagnosed between October 2007 and September 2009, were alive, and had been managed at one of 15 centres throughout the country for which we had ethical approval. The pool of eligible patients was 2,899, but decreased by 159 when a manual review of recent deaths was conducted. The clinician of each eligible patient was contacted. Clinician information was returned on 1,609 patients, 283 of whom were not eligible to participate. Eligible individuals had a good understanding of English, were aware they had cancer, were well enough to participate, and were cognitively able to give informed consent, as assessed by their clinicians.
Surveys, informed consent forms, study information leaflets, and letters of invitation to participate were sent to 1,273 eligible individuals. Responders returned a survey and completed informed consent form by post. Non-responders were sent two reminder letters and surveys at fortnightly intervals.
Measures
Quality of life measures
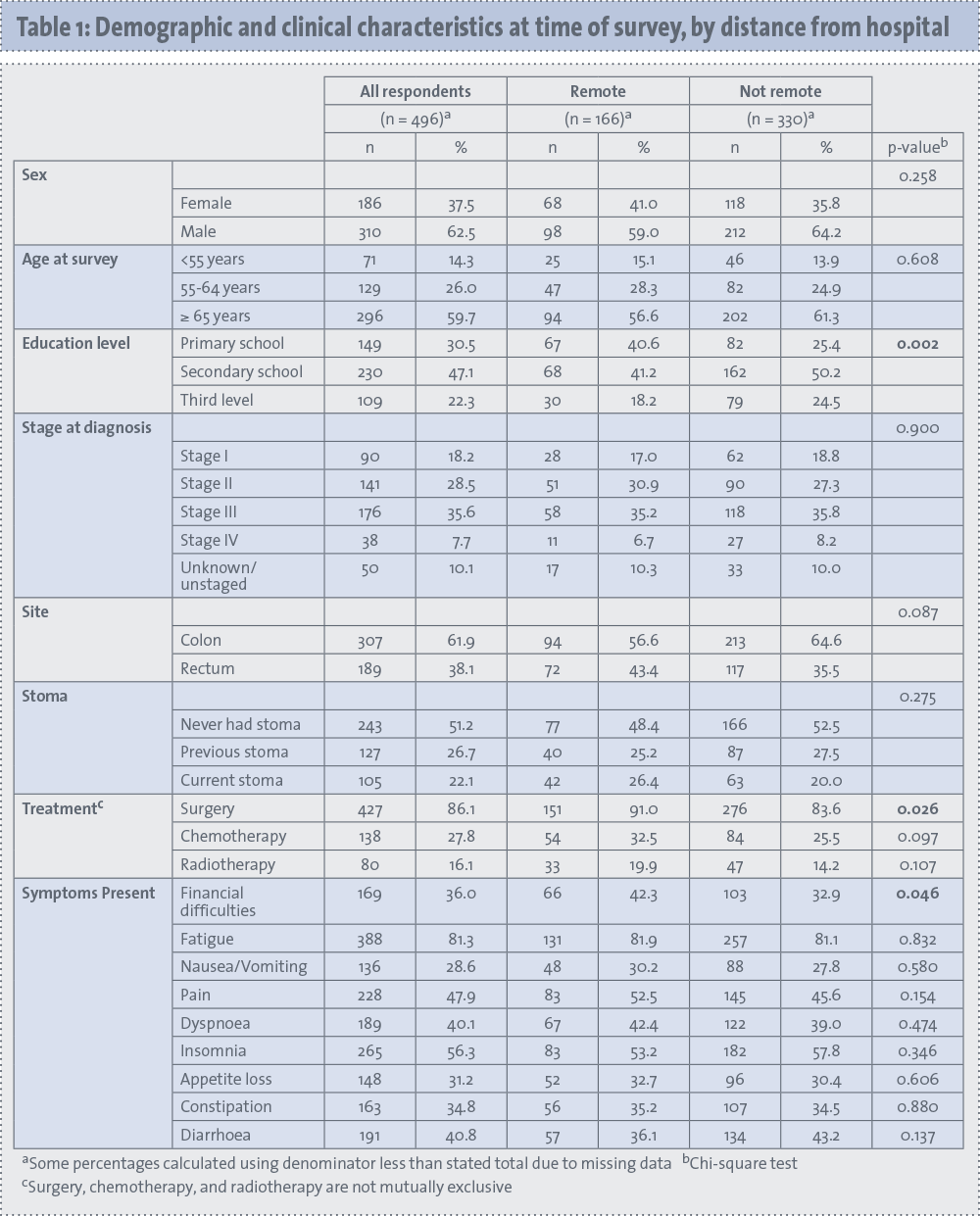
Colorectal cancer survivors were asked to complete the QLQC30, which is a widely-used QoL instrument developed by the European Organisation for Research and Treatment of Cancer (EORTC).22,23 It measures global health status (GHS) and five functional domains. Physical functioning concerns the respondent’s ability to perform routine physical activities. Role functioning is defined as the respondent’s ability to pursue work and leisure activities. Items on emotional functioning are about feeling tense, irritable, depressed, or being worried. Cognitive functioning is defined as concentration and memory. How illness interferes with family life and social activities are considered social functioning. GHS is comprised of self-ratings of the respondent’s overall health and quality of life. GHS and each functional domain were scored, with the procedure outlined by EORTC (see Table 1).24
(click to enlarge)
Distance from each participant’s residence to their hospital was calculated based on their postal address at the time of diagnosis, as recorded by the National Cancer Registry, and the hospital where they were treated (for surgery, other hospital admittance, chemotherapy, radiotherapy, or follow-up), as reported on the survey. Bazzoli and colleagues,25 studying different areas in the US, divided distance to hospital into tertiles and used the last tertile to define ‘remote residence’. In addition, the authors have used this measure of remoteness in a composite variable for rurality in Ireland.26 Thus, for the present study, distance from residence to hospital was divided into tertiles and the last tertile (ie. residing farthest from the hospital) was classified as ‘remote residence’, while the remaining two tertiles are classified together as ‘not remote’. In this study, a respondent defined as ‘remote’ lived farther than 30.81km from their treating hospital.
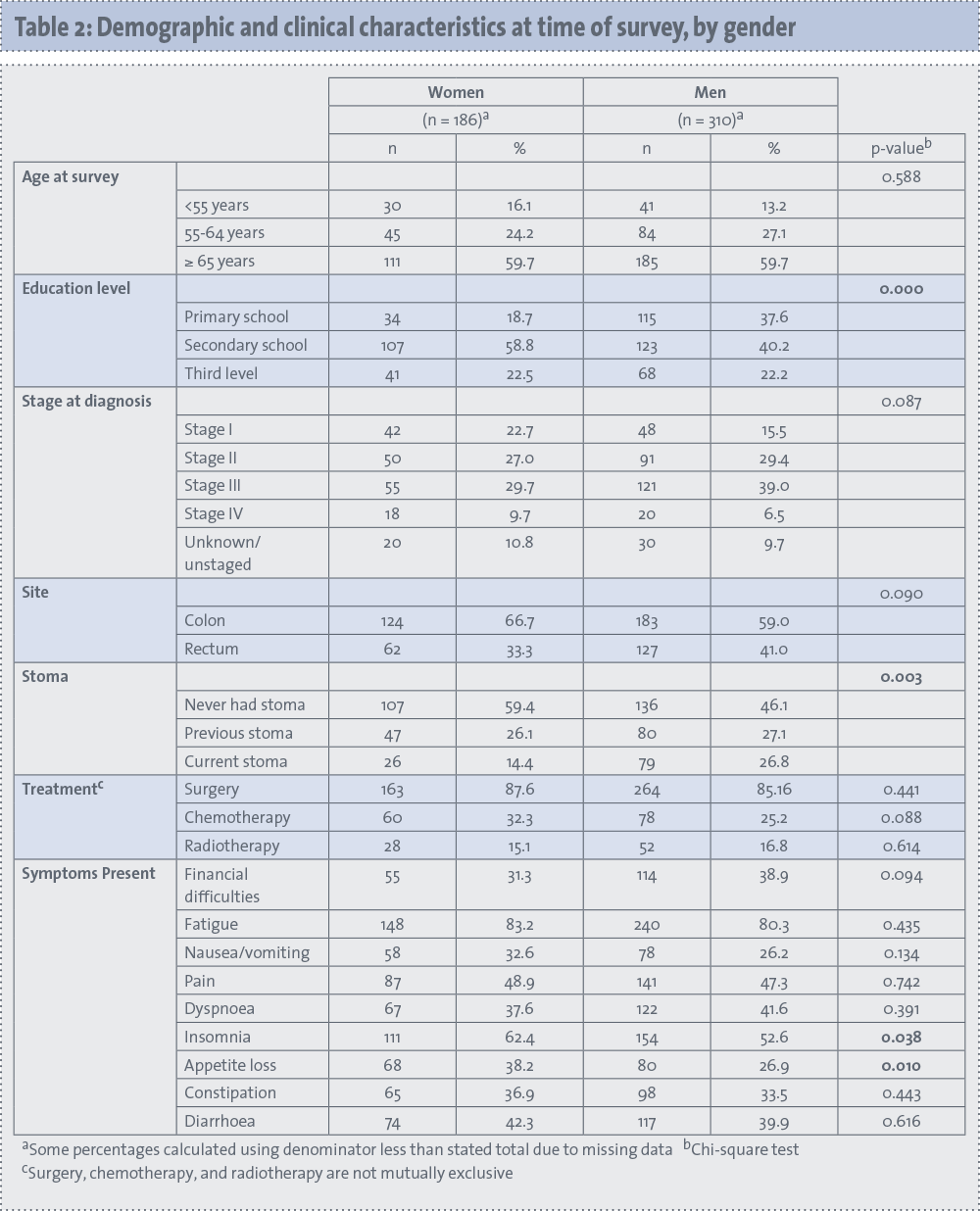
Respondents living 30.81km or closer to their treating hospital are defined as ‘not remote’. The gender of each participant was obtained from the registry (see Table 2).
(click to enlarge)
Confounding variables
The clinical variables (site, stage at diagnosis, and treatment) were acquired from the registry. The previous or current presence of a stoma was self-reported on the survey.
According to reviews of colorectal cancer survivors, QoL is related to age, education (when the model is not adjusted for income), and symptoms.27,28 Age at survey was obtained from the registry and divided into three categories: less than 55 years old, 55-64 years old, and 65 and older. Income data was not available, so highest level of education was taken from the survey and categorised as primary, secondary, and third-level.
Symptom variables, including the measure of financial difficulties, were self-reported in the QLQ-C30. Each symptom scale or item was coded as ‘have symptom’ or ‘do not have symptom’.
Analysis
Chi-square tests were used to determine significant differences in demographic and clinical variables between responders and non-responders, remote and non-remote responders, and men and women responders.
Since the QoL domain scores were skewed, Wilcoxon-Mann-Whitney tests were used to determine if there were differences by remote residence. If significant differences were detected in this bivariate analysis, those QoL domains were tested in multivariate analysis.
Linear regression was used to assess the relationship between the QoL scales and distance from hospital, while controlling for demographic and clinical variables. To account for the skewness of the QoL outcomes, regression models were bootstrapped, and bias-corrected and accelerated confidence intervals were calculated.
While the confidence intervals can be used to determine significance at the 0.05 level, a precise p value is not calculated with this type of model. Selection of variables for the multivariate models was based on previous literature and bivariate analysis of the current sample. If, for a specific demographic or clinical variable, there was a significant difference (p < 0.05) in remote and non-remote respondents, that variable was added to the multivariate model.
The final multivariate model was used to estimate each QoL domain that was significantly related to remoteness in the bivariate analysis. The final model was run on three samples: the full sample, men, and women. All statistical analyses were conducted in Stata 12.1.29
Results
Study sample
Of the 1,273 eligible colorectal cancer survivors invited to participate, 496 returned surveys, yielding an adjusted response rate of 39%. Non-responders tended to be older than responders: while 26% of responders were 74 years old or older, 37% of non-responders were in this older age group (p < 0.001). Responders and non-responders did not significantly differ on gender, tumour site, treatments received, stage at diagnosis, or time since diagnosis.
Table 1 shows demographic and clinical variables for the survey sample. Since remoteness was defined by tertiles, 33% of the sample was categorised as remote. The sample was 63% male. The mean age of participants was 67.4 (±11.6) years. The colon (ICD-10 C18-C19) was the site of the primary tumour for 62% of the sample. About half of the respondents (49%) reported ever having a stoma, including 22% with a stoma at the time of the survey. Among the current symptoms survivors were experiencing at the time of the survey, the most common were fatigue (81%), insomnia (56%) and pain (48%).
Table 1 also reports these variables by distance from hospital (remote and not remote). Remote respondents had lower education levels than non-remote respondents. While 41% of the remote respondents reported completing secondary school, this figure was 50% (p = 0.002) for non-remote respondents. More remote respondents had had surgery (p = 0.026). Financial difficulties were more common among remote respondents (p = 0.046).
In Table 2, demographic and clinical variables are presented by gender. A greater proportion of women (59%) than men (40%) report having a secondary school education (p < 0.001). More women (59%) than men (46%) had ever had a stoma (p = 0.005). Also, women more often reported problems with insomnia (p = 0.038) and appetite loss (p = 0.010).
Bivariate analysis
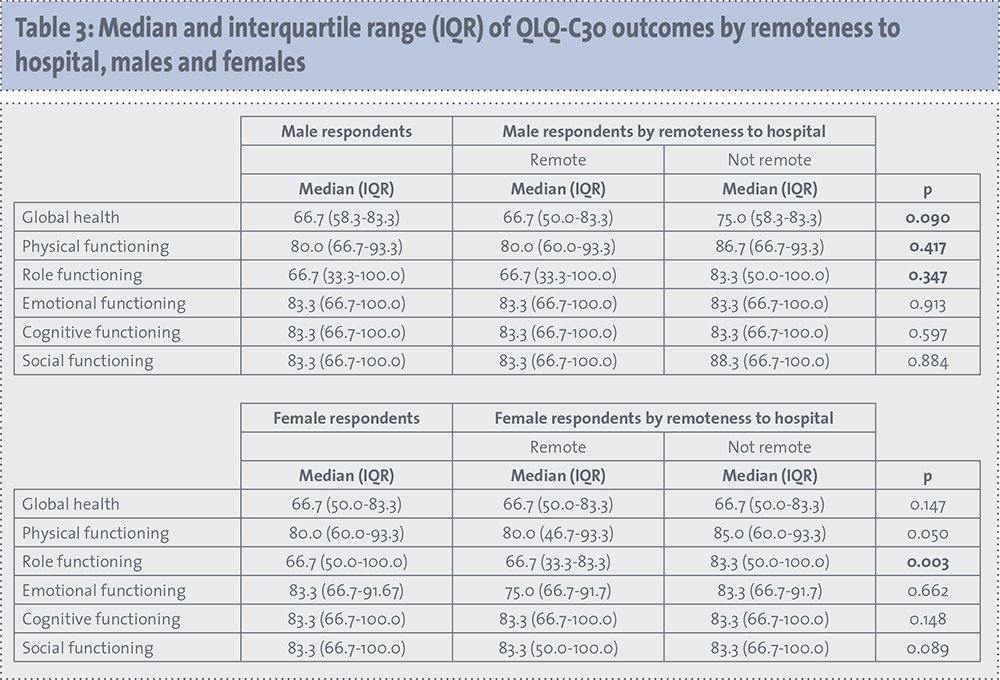
The median and interqaurtile range for each Qol domain for the full sample, by remote residence, showed that remote colorectal cancer survivors reported lower GHS (p = 0.013) and lower physical (p = 0.045) and role functioning (p = 0.007). Remote residence was not associated with cognitive, social, or emotional functioning.
Summary statistics for each QoL domain for men and for women, by remote residence, is presented in Table 3. As with the analysis for the full sample, the overall pattern was of remote respondents having lower QoL scores than non-remote respondents. Remote women reported lower role functioning (p = 0.003) than non-remote women. Differences in physical functioning in women approached significance (p = 0.050), as did global health status (GHS) in men (p = 0.090).
(click to enlarge)
Multivariate analysis
The multivariate regression models control for gender, age, education, and symptoms, which have been significantly related to QoL in the literature, as well as cancer-directed surgery, was found to significantly differ for remote and non-remote respondents. There was no relationship between remote residence and cognitive, emotional, or social functioning, for the total sample, for men, or for women.
Survivors who were remote from the treating hospital had significantly lower physical functioning (p < 0.05) and role functioning (p < 0.05) than those who were non-remote. Having had surgery was related to lower GHS (p < 0.05). Fatigue, pain, dyspnoea, and appetite loss were associated with lower scores on all QoL domains. Financial difficulties and diarrhoea were negatively related to GHS and role functioning. Nausea and vomiting was also associated with decreased role functioning.
For women, remote residence was significantly associated with lower scores on physical functioning (p < 0.05) and role functioning (p < 0.05). Remote men had significantly lower GHS (p < 0.05). Dyspnoea was negatively related to GHS, physical functioning, and role functioning for women and for men. For both genders, fatigue, pain, and appetite loss had significant negative relationships to some QoL domains. Financial difficulties and diarrhoea were only associated with decreased QoL in men.
Discussion
Controlling for demographic and clinical variables, colorectal cancer survivors who live farther from their treating hospitals reported lower physical and role functioning. A further analysis by gender reveals that these findings hold for female colorectal cancer survivors. For men, physical and role functioning were not significantly lower for remote colorectal cancer survivors; however, GHS was significantly reduced in this group. Distance decay may affect survivors differently based on which of the three stages of cancer survivorship (acute, extended, or permanent) they are experiencing.
Previous studies have shown the negative effect of distance decay in the acute and extended stages of cancer survivorship. This study suggests that this disadvantage extends into the permanent stage. Furthermore, this study has the unique aspect of highlighting gender differences; while both genders are affected, remoteness is related to different QoL domains for men and for women.
The results suggest that remote colorectal cancer survivors, women in particular, have more trouble with daily activities, as evidence by their lower physical functioning scores. Encouraging routine physical activity is a critical part of colorectal cancer survivorship care. A wealth of studies link physical activity with increased QoL among colorectal cancer survivors.30,31,32 Clinicians may need to emphasise this with women in particular, as there is some evidence that women colorectal cancer survivors may be less likely than men to take up physical activity.30 Underlying physical health problems impact daily work, both inside and outside the home. The lower role functioning scores for remote female colorectal cancer survivors suggest that they may feel unable to work or that they are limited in their work.
The study revealed important gender differences in cancer survivors’ QoL, contributing to the limited evidence base in this area. This suggests that if researchers do not examine men and women survivors separately, they run the risk of overlooking the particular needs of one group. For example, in the present study, no difference was found between remote and non-remote survivors in terms of GHS; however, when separate models were run for each gender, a difference between remote and non-remote men emerged. Men living remote from hospital had lower GHS than those living closer to hospital.
In an article advocating gender analysis in health planning and programming, Vlassoff and Moreno33 contend that taking gender into account will make health services more relevant and effective.
The study’s findings that aspects of QoL were lower for remote survivors could be explained by remote survivors viewing hospital visits for post-treatment follow-up as ‘optional’, especially in comparison to appointments for tumour-directed treatments and given related research that showed that carers of colorectal cancer patients had significant time and out-of pocket costs related to travel.34 As such, these services in the permanent stage of cancer are possibly even more prone to the effects of distance decay. Further exploration of this explanation was not possible due to lack of data on attendance of and default on follow-up visits. Nonetheless, a local, accessible GP is an important option in remote survivors’ follow-up in the permanent stage.35
In order to feel confident in being responsible for cancer survivors’ follow-up, GPs have expressed the need for co-ordination with specialists and written guidelines for surveillance testing.36 In addition, the roles of oncology specialists and GPs must be clearly defined.37
Colorectal cancer survivors face myriad and difficult challenges daily. Concurring with the existing literature,38 our findings demonstrate that high proportions of colorectal cancer survivors, even in the permanent stage, continue to experience symptoms such as fatigue, pain, insomnia, and dyspnoea.
Previous studies have shown that colorectal cancer-related symptoms are significantly related to QoL39 and depression.40 In this study, two of the most commonly reported symptoms, fatigue (81%) and pain (48%), were significantly associated with decreased QoL scores in some domains for all respondents, for men, and for women.
Dyspnoea, which affected 40% of the respondents, was significantly related to QoL domains in all multivariate models presented. Appetite loss was also associated with significant decreases in QoL domains for both genders.
Good health behaviours are associated with a decrease in colorectal cancer survivors’ symptoms. In particular, physical activity has been linked to lower fatigue, pain, and insomnia.31 All healthcare providers could be more cognizant of the common symptoms of fatigue, pain, and insomnia in colorectal cancer survivors, and take proactive steps to ameliorate these conditions. Addressing these symptoms should help increase physical and overall QoL. It is notable that financial difficulties and diarrhoea, significantly related to GHS and role functioning in the full sample, were significantly related to QoL domains for men but not women. Men and women may experience the same symptoms, but the relationship of those symptoms to QoL could differ by gender.
Several limitations of this study should be noted. The response rate to the survey was 39%. In a comparison of responders and non-responders, however, only differences in age were significant. The younger age of responders versus non-responders may affect the overall QoL scores since age has been shown to have a significant relationship with colorectal cancer survivors’ QoL.27,38 However, there were no differences in age between remote and non-remote respondents, and between men and women, so internal validity should be unaffected.
The issue of sexual function of colorectal cancer survivors has been brought up as a needed topic for further research41,42 but was not investigated in this study.
Conclusion
Remote colorectal cancer survivors in Ireland have unique needs in terms of their QoL, and physical and role functioning. Targeted resources for improving these outcomes may decrease the disparity associated with distance decay.
Survivorship plans could be a collaborative effort between oncology specialists and GPs to help ensure that local GPs are more aware of, and attuned to, the needs of colorectal cancer survivors. These results suggest that individual survivorship plans take gender into account, to forestall known problem areas.
Future research could prospectively study clinical and patient-reported outcomes among remote cancer survivors whose post-treatment follow up is done by their local GP compared to those who continue to commute to the treating hospital.
This paper addresses evidence gaps around how remoteness and gender influence QoL, and physical and role functioning in colorectal cancer survivors. Given the many issues colorectal cancer survivors face on their cancer journey, providing targeted services during the permanent stage may improve specific aspects of and overall quality of life.
References
Fazio L, Cotterchio M, Manno M, et al. Association Between Colonic Screening, Subject Characteristics, and Stage of Colorectal Cancer. Am J Gastroenterol 2005;100:2531-9
Jones AP, Haynes R, Sauerzapf V, et al. Travel times to health care and survival from cancers in Northern England. Eur J Cancer 2008; 44: 269-74
Campbell NC, Elliott AM, Sharp L, et al. Impact of deprivation and rural residence on treatment of colorectal and lung cancer. Br J Cancer 2002; 87: 585-90.
Jones AP, Haynes R, Sauerzapf V, et al. Travel time to hospital and treatment for breast, colon, rectum, lung, ovary and prostate cancer. Eur J Cancer 2008; 44: 992-9.
Goldsbury D, Harris MF, Pascoe S, et al. Socio-demographic and other patient characteristics associated with time between colonoscopy and surgery, and choice of treatment centre for colorectal cancer: a retrospective cohort study. BMJ Open 2012; 2.
Baade PD, Dasgupta P, Aitken JF, et al. Distance to the closest radiotherapy facility and survival after a diagnosis of rectal cancer in Queensland. Med J Aust 2011; 195: 350-4.
Cramb SM, Mengersen KL, Turrell G, et al. Spatial inequalities in colorectal and breast cancer survival: premature deaths and associated factors. Health Place 2012; 18: 1412-21.
Dunn J, Ng SK, Breitbart W, et al. Health-related quality of life and life satisfaction in colorectal cancer survivors: trajectories of adjustment. Health Qual Life Outcomes 2013; 11: 46.
Lundy JJ, Coons SJ, Wendel C, et al. Exploring household income as a predictor of psychological well-being among long-term colorectal cancer survivors. Qual Life Res 2009; 18: 157-61.
Ramsey SD, Andersen MR, Etzioni R, et al. Quality of life in survivors of colorectal carcinoma. Cancer 2000; 88: 1294-303.
Schultz AA, Winstead-Fry P. Predictors of quality of life in rural patients with cancer. Cancer Nurs 2001; 24: 12-9.
Phipps E, Braitman LE, Stites S, et al. Quality of life and symptom attribution in long-term colon cancer survivors. J Eval Clin Pract 2008; 14: 254-8.
Mullan F. Seasons of Survival: Reflections of a Physician with Cancer. NEJM 1985; 313: 270-3.
A National Action Plan for Cancer Survivorship: Advancing Public Health Strategies. Center for Disease Control and the Lance Armstrong Foundation 2004. www.cdc.gov/cancer/survivorship/pdf/plan.pdf (accessed Mar 11, 2014).
Mullan F. Re-entry: The educational needs of the cancer survivor. Health Educ Q. Published Online First: 1984. http://psycnet.apa.org/psycinfo/1984-32234-001 (accessed Feb 14, 2014).
Taylor PJ. Distance decay models in spatial interactions. 1975. www.getcited.org/pub/101710242 (accessed Mar 14, 2014).
Arcury TA, Gesler WM, Preisser JS, et al. The Effects of Geography and Spatial Behavior on Health Care Utilization among the Residents of a Rural Region. Health Serv Res 2005; 40: 135-56.
Baldwin L-M, Cai Y, Larson EH, et al. Access to cancer services for rural colorectal cancer patients. J Rural Heal 2008; 24: 390-9.
Bain NS, Campbell NC, Ritchie LD, et al. Striking the right balance in colorectal cancer care – a qualitative study of rural and urban patients. Fam Pract 2002; 19: 369-74.
Archampong D, Borowski D, Wille-Jørgensen P, et al. Workload and surgeon’s specialty for outcome after colorectal cancer surgery. Cochrane Database Syst Rev 2012;3: CD005391. doi:10.1002/14651858.CD005391.pub3
McIntyre, Peter. Ireland’s Bumpy Road to a World-Class Cancer Service.
Cancer World 2004 :54-8.
Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993; 85: 365-76.
Groenvold M, Klee MC, Sprangers MA, et al. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol 1997; 50: 441-50.
Fayers P, Aaronson N, Bjordal K, et al. The EORTC QLQ-C30 Scoring Manual. 3rd ed. Brussels: European Organisation for Research and Treatment of Cancer 2001. www.eortc.be/qol/files/SCManualQLQ-C30.pdf (accessed Oct 1, 2013).
Bazzoli GJ, Lee W, Hsieh H-M, et al. The Effects of Safety Net Hospital Closures and Conversions on Patient Travel Distance to Hospital Services. Health Serv Res 2012; 47: 129-50.
Thomas AA, Timmons A, Molcho M, et al. Quality of Life in Urban and Rural Settings: A study of head and neck cancer survivors. Oral Oncol: In Press.
Jansen L, Koch L, Brenner H, et al. Quality of life among long-term (≥ 5 years) colorectal cancer survivors – systematic review. Eur J Cancer 2010; 46: 2879-88.
Bloom JR, Petersen DM, Kang SH. Multi-dimensional quality of life among long-term (5+ years) adult cancer survivors. Psychooncology 2007; 16: 691-706.
StataCorp. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP 2011.
McGowan EL, Speed-Andrews AE, Rhodes RE, et al. Sport participation in colorectal cancer survivors: an unexplored approach to promoting physical activity. Support Care Cancer 2013; 21: 139-47.
Grimmett C, Bridgewater J, Steptoe A, et al. Lifestyle and quality of life in colorectal cancer survivors. Qual Life Res 2011; 20: 1237-45.
Courneya KS, Friedenreich CM, Quinney HA, et al. A randomized trial of exercise and quality of life in colorectal cancer survivors. Eur J Cancer Care (Engl) 2003; 12: 347-57.
Vlassoff C, Moreno CG. Placing gender at the centre of health programming: challenges and limitations. Soc Sci Med 2002; 54: 1713-23.
Hanly P, Céilleachair AÓ, Skally M, et al. How much does it cost to care for survivors of colorectal cancer? Caregiver’s time, travel and out-of-pocket costs. Support Care Cancer 2013; 21: 2583-92.
Lengerich EJ, Kluhsman BC, Bencivenga M, et al. Development of community plans to enhance survivorship from colorectal cancer: Community-based participatory research in rural communities. J Cancer Surv 2007; 1: 205-11.
Giudice MED, Grunfeld E, Harvey BJ, et al. Primary Care Physicians’ Views of Routine Follow-Up Care of Cancer Survivors. J Clin Oncol 2009; 27: 3338-45.
Snyder CF, Earle CC, Herbert RJ, et al. Trends in Follow-up and Preventive Care for Colorectal Cancer Survivors. J Gen Intern Med 2008; 23: 254-9.
Arndt V, Merx H, Stegmaier C, et al. Restrictions in quality of life in colorectal cancer patients over three years after diagnosis: A population based study. Eur J Cancer 2006; 42: 1848-57.
Ramsey SD, Berry K, Moinpour C, et al. Quality of life in long term survivors of colorectal cancer. Am J Gastroenterol 2002; 97: 1228-34.
Gray NM, Hall SJ, Browne S, et al. Predictors of anxiety and depression in people with colorectal cancer. Support Care Cancer 2013: 1-8.
Traa MJ, De Vries J, Roukema JA, et al. Sexual (dys) function and the quality of sexual life in patients with colorectal cancer: a systematic review. Ann Oncol 2012; 23: 19-27.
Milbury K, Cohen L, Jenkins R, et al. The association between psychosocial and medical factors with long-term sexual dysfunction after treatment for colorectal cancer. Support Care Cancer 2013; 21: 793-802.
 (click to enlarge)
(click to enlarge)