With alcohol linked to over 60 medical conditions, screening for alcohol misuse is critical in clinical practice and interventions should be based on the stage of dependence determined
Dr Larkin Feeney, Consultant Psychiatrist, Cluain Mhuire Community Mental Health Service, Blackrock, Co Dublin, Dr Leonard Douglas, Senior Registrar, Cluain Mhuire Psychiatric Service, Blackrock, Co Dublin and Dr Máiréad Redahan, GP, Medical Centre, Dublin
In Ireland we rank fifth highest in the average consumption of pure alcohol per drinker (at 11.9 litres compared to an average of 9.4 litres in OECD countries).1 With alcohol being linked to more than 60 medical conditions,2 this ensures that GPs are constantly confronted with the patient for whom alcohol is a major modifiable factor.
Screening for alcohol misuse is critical in clinical practice.3 Early detection leading to brief interventions can reduce ongoing problems associated with alcohol misuse. Simply asking about alcohol use can have a positive effect on drinking behaviour.
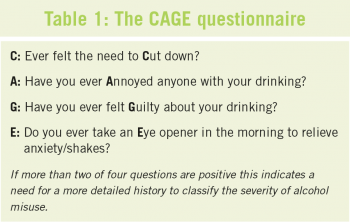
The CAGE questionnaire is a well known four question screening tool for alcohol misuse (see Table 1). The 10-item AUDIT questionnaire can also be used to screen for alcohol misuse and determine where on the scale from low risk to dependence a patient lies (see Table 2).
(click to enlarge)
(click to enlarge)
Classifying severity of alcohol misuse
First it is important to place the patient’s drinking on the scale low risk to dependence.
Low risk: consumption within the recommended safe drinking levels (less than 11 units for women and 17 for men per week)4
Hazardous drinking: a level of consumption above the recommended levels, but without any harmful consequences to date
Harmful drinking: consumption above the recommended levels with harmful consequences.
Dependent drinking:5 this is where the substance begins to profoundly affect the user in physiological, behavioural, social and psychological ways. The strong desire or compulsion to drink alcohol, coupled with the use of alcohol taking on a much higher priority than other behaviours which previously were valued by that individual, often has significant effects on the individual’s health, relationships as well as social consequences for the individual and society at large.
Dependence is a condition with biological, social and psychological roots, which each treatment modality addresses in differing ways. Depending on patterns of drinking and individual differences, one patient drinking excessively may show signs and symptoms of dependence while another may not. The presence or absence of a diagnosis of dependence is therefore important to ascertain. For dependent drinkers the advice will usually be to aim for abstinence, and the interventions needed to attain this may be more intensive from the outset.
It is not a ‘one size fits all’ approach but that of trying to tailor the best fit to the patient. Many approaches are implementable in, and appropriate to, a primary care setting.
Dependent drinking is characterised by the ICD-10 by the presence of three or more of the following:
A strong desire or compulsion to drink alcohol
Difficulty controlling drinking
Physiological withdrawal symptoms
Development of tolerance to the effects of alcohol
Primacy of drinking behaviour with neglect of other interests
Persistent drinking despite clear evidence of associated harm.
The AUDIT questionnaire is useful in determining where on the scale from low risk to dependence a patient lies and the intervention needed.6
If a diagnosis of dependency is made, the Severity of Alcohol Dependence Questionnaire (SADQ)28 can then be used to quantify the severity of dependence present which can inform the level of treatment required.
Choosing an intervention
Once the presence and level of alcohol misuse is determined it is now necessary to try to help the patient implement a change in their behaviour.
To modify behaviour we need to look to the psychology of addiction for direction. Behaviour and motivation to change are complex and influenced by many factors. These factors can be internal such as knowledge about risks, assumption about drinking, self-belief, optimism about alternatives, craving and guilt.
These factors can also be external such as those that perpetuate or normalise the behaviour (role models, peer behaviour, cost, lack of consequences). Psychological interventions and public health measures try to tackle these problems at several levels depending on where a patient is in the process of behavioural change.
The Stages of Change model of behaviour change7 is very useful in formulating what intervention will be most suitable at this time for a patient.
In essence, patients need help to:
Become aware they have a problem (pre-contemplation)
Motivate themselves to modify their drinking behaviour (contemplation and preparation)
Maintain any changes which are commenced (action and maintenance).
Each stage requires a different management plan.
The interventions
Brief interventions are in their simplest a form non-judgmental advice to promote awareness of the adverse effects of drinking and to motivate change. Research has shown that brief interventions are effective and have the strongest evidence base.8 They can be as effective as more extensive therapies (especially for those with hazardous drinking).9
Although there are differing forms of brief interventions, six key components have been noted in successful treatments. These are useful to consider and are referred to as the ‘FRAMES’.
Feedback: The patient receives a frank assessment and evaluation of the problem
Responsibility: Drinking is construed as a behaviour which is a choice. One can choose not to drink
Advice: The patient is given clear advice on changing behaviour
Menu: The doctor should offer a range of alternate goals and strategies. Not ‘a one size fits all’ approach
Empathy: express empathy and be non-judgemental
Self-efficacy: Instill optimism in the patient that the chosen goals can be achieved.
It is worth reviewing one’s own practice with the above in mind in order to ensure we maximise our ability to impact on a patient’s behaviour.
Motivational interviewing is another form of brief intervention that is well supported by the literature.10,34 Motivational interviewing at its heart tries to accelerate change, by creating a motivation for change by highlighting discrepancies between present behaviour and important personal goals. Motivational interviewing techniques are useful tools which aid many GPs. It is particularly useful in the preparation, contemplation and precontemplation stages of change. Motivational interviewing requires training which is becoming increasingly available to primary care teams.
Cognitive behavioural therapy and relapse prevention therapy are more suited to the addict who has recently given up or is attempting to maintain abstinence (action and maintenance). They work on trying to help the patient understand their patterns of relapse so at time of high risk/stress they have strategies to prevent relapse. These are usually provided by community addiction services. Interventions based on the 12-step approach (AA) are effective for many. This approach regards addiction as a relapsing illness with complete abstinence as the only treatment goal.
Family therapies are useful in getting patients into therapy and helping them remain in treatment (contemplation + pre-contemplation + action). This can be useful for patients who are reluctant to engage in therapy. Family therapy/interventions are available within some community alcohol services. A family member can enter family therapy prior to the affected individual engaging. Al-Anon can also be helpful for families.
Pharmacological agents are another way to effect and maintain behavioural change.
Case studies
Case one
A 25-year-old female presents to the GP practice for removal of sutures five days post a forehead laceration.
On taking a history while removing the sutures placed in A&E she related how the injury occurred after tripping in high heels after having a ‘few drinks’. Indeed, 28% of all injuries that present to A&E in Ireland are alcohol related.11
You see this as an opportunity to ask more about her alcohol use and she admits to having a bottle of wine usually three or occasionally four nights per week and might have two bottles of wine on a Saturday night. She feels it never affects her work performance as an IT consultant and feels many of her friends, both male and female, have a similar drinking pattern.
You calculate that your patient is consuming somewhere between 48 and 72 units per week. She seems surprised at the total number of units per week and she asks about the maximum number of drinks she could have per week. Indeed in one study less than one out of ten people knew the correct standard number of drinks that women can safely consume per week (which according to the pre 2010 guidelines was 14 standard drinks). The same survey showed that there is a poor understanding of what a standard drink is; for example less than one in four people were aware that a 200ml glass of wine could contain two standard drinks.12 Furthermore, HSE unit guidelines have since been reduced to 11 units or less (standard drinks) per week for women and 17 units or less for men.13
You go through the 10-item AUDIT and she scores 15, indicating harmful and hazardous drinking, but on further history taking she does not fulfil the ICD-10 criteria for alcohol dependence at this stage. As she is at the contemplation stage, discussing some of the facts around units in a non-judgemental fashion and simple advice as per the FRAMES-style discussed in the introduction is appropriate.
Although women generally drink less alcohol in volume and frequency than men, patterns of drinking in women are beginning to become closer to those of male counterparts. Many women may not be aware of how alcohol affects them differently to men. Women generally develop long-term health consequences earlier than men. For similar doses of alcohol, women are more vulnerable than men to tissue damage and the onset of cirrhosis of the liver. Women generally advance from their first drink to their first alcohol-related problem to the need for treatment more quickly than men, ie. an accelerated course of dependence. Several biological factors make women more vulnerable to the effects of alcohol than men. Women tend to weigh less than men, and a woman’s body contains less water and more fatty tissue than a man’s. Because fat retains alcohol while water dilutes it, alcohol remains at higher concentrations for longer periods of time in a woman’s body, exposing her brain and other organs to more alcohol. Women also have lower activity of the enzyme alcohol dehydrogenase that metabolises alcohol in the stomach. As a result, women absorb more alcohol into their bloodstreams than men. There is also an increase in invasive breast cancer incidence associated with alcohol intake. Consumption of three to six units per day increases the risk of invasive breast cancer by 41% compared to non-drinker.15 Alcohol can also affect normal menstrual cycling in females.16
You note she is back for a contraceptive pill check in two months and flag in your notes this appointment as an opportunity for feedback, monitoring and further brief intervention, if appropriate, regarding her drinking.
Case two
A 55-year-old gentleman presents to your practice complaining of generalised fatigue and ‘feeling out of sorts’ for four to five months. His only past medical issue is that of a duodenal ulcer which was treated successfully 15 years ago. He worries that his symptoms may be related to a recurrence of his ulcer. Physical examination revealed mild epigastric discomfort. He denies any excessive alcohol intake.
You question him about depressive symptoms: He reports he is stressed and acknowledges that his motivation and concentration are ‘not what they were’. He reports initial insomnia on occasion. He says he has lost all interest in playing tennis and attending the local tidy-towns committee. His appetite is normal.
In spite of his psychological state being a possible cause of some of his symptoms you feel further physical investigations are warranted initially. You arrange routine blood testing and a gastroscopy. These tests reveal mild gastritis. No biochemical abnormalities are present apart from a raised GGT.
He returns three weeks later for results. Given the test results, you raise your concerns regarding alcohol misuse and he now admits to drinking up to six units at home most nights. He has begun to wonder if he does have a problem. CAGE questionnaire scores were 2/4 (+ tried to cut down + wife annoyed). He did not fulfil criteria for dependence. Many symptoms of excessive alcohol intake can mimic those of depression. The Epidemiological Catchment Area (ECA) study found that 13% of those with an alcohol use disorder met criteria for a mood disorder.26 In this case his stress was due to his wife expressing her concerns regarding his drinking. His apparent loss of interest in social activities was in fact an attempt to conceal his recent heavy drinking.
The patient was asked specifically about suicidal ideation, given the fact that risk of suicide is increased by 60-120 times in those who are alcohol-dependent.27 This case is that of a non-dependent but harmful drinker who is keen to reduce his drinking (preparation stage). A brief intervention by GP or healthcare professional is the appropriate first step and has the strongest evidence base.19 This should be structured using the FRAMES guidelines (as above). If this initial intervention proved to be unsuccessful, a motivational interviewing (MI) approach may improve his chances of success.3 The patient (as with many substance misusers) is aware he has a problem and appears keen to reduce consumption but as yet has not succeeded (ambivalence). This is precisely where MI targets its efforts.
The patient was informed that it was prudent to first attempt to reduce his alcohol intake prior to considering any specific psychological treatment or medication aimed at addressing his depressive symptoms.29 Depressive symptoms often abate with abstinence30 and a reassessment at one month post cessation is advised. In this case his depressive symptoms did not abate entirely with abstinence.
Patients who take SSRI antidepressants are at a significantly increased risk of upper GI bleeds31 although these risks are reduced with co-administration of a PPI. Given this patient’s medical history he was referred to an alcohol counsellor using a CBT approach, the purpose of which was to help prevent relapse and address his depressive symptoms without medication.
He has made a good recovery with regard to his mood and has maintained abstinence to date.
Conclusion
Tackling the patient who has problem drinking can be difficult and at times disheartening, especially when service provision is often lacking. It is important to remember that it is often a problem we can’t always solve by ourselves.
The primary care solution delivered by GPs is part of a solution that should include public health, legislation, specialist out and inpatient services, family and of course most centrally the patient ready to make a change.
References
Steering group report on a National Substance Misuse Strategy. February 2012.
Barclay GA, Barbour J, Stewart S, Day CP, Gilvarry E. Adverse physical effects of alcohol misuse. Advances in Psychiatric Treatment 2008; 14: 139-151.
Raistrick D, Heather N, Godfrey C. Review of the Effectiveness of Treatment for Alcohol Problems. UK National Treatment Agency for Substance Misuse, 2006.
HealthPromotion.ie
World Health Organization. Global Status Report on Alcohol 2004. Geneva: World Health Organisation, 2004.
F.Babor, John C.Higgins-Biddle et al. The Alcohol Use Disorder Identification Test. Guidelines for Use in Primary Care Thomas World Health Organization. Department of Mental Health and Substance Dependence.
Prochaska JO, DiClimente CC. Towards a comprehensive model of change. Treating addictive behaviours , 2nd ed. Plenum 1996.
Miller WR, Wilbourne PD, Hetema JE. What works? A summary of alcohol treatment outcome research. In Handbook of Alcoholism Treatment Approaches: Effective Alternatives (eds Hester RK, Miller WR): 13–63. Allyn and Bacon, 2003.
Moyer A, Finney JW, Swearingen CE, Vergun P. Brief interventions for alcohol problems. A meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction 2002; 97: 279–92.
Shamil Wainigaratne et al. The effectiveness of psychological therapies on drug misusing clients. NHS, 2005.
Hope A, Gill A et al (2005) Alcohol and injuries in the accident and emergency department – a national perspective. Dublin: Department of Heath and Children.
Alcohol: public knowledge, attitudes and behaviours; Ipsos MRBI. Published by Health Research Board July 2012.
HealthPromotion.ie
Mongan et al 2007 Heath related consequences of alcohol use. Dublin: Health Research Board.
Smith -Warner SA, Spiegelman D et al. Alcohol and Breast Cancer in Women: a pooled analysis of cohort studies. JAMA. 1998; 279(7):535-540.
Emanuele MA et al. Alcohol’s effects on female reproductive function. Alcohol Res Health. 2002; 26 (4): 274-81.
Moos RH, Moos BS. Participation in treatment and Alcoholics Anonymous: a 16-year follow-up of initially untreated individuals. Journal of Clinical Psychology. 2006;62(6):735–750.
Project MATCH Research Group. Matching alcoholism treatment to client heterogeneity: Project MATCH post treatment drinking outcomes. J Stud Alcohol. 1997;58(1):7–29.
Hayashida M et al. Comparative effectiveness and costs of inpatient and outpatient detoxification of patients with mild-to-moderate alcohol withdrawal syndrome. N Engl J Med. 1989;320(6): 358-65.
Thompson et al. The treatment of patients at risk of developing Wernickes encephalopathy in the community. Alcohol and Alcoholism 2006; 41:151-158
The Maudsley Prescribing Guidelines 10th Edition.
Suh, Jesse J. PsyD; Pettinati, Helen M. PhD; Kampman, Kyle M. MD; O’Brien, Charles P. MD, PhD The Status of Disulfiram: A Half of a Century Later. Journal of Clinical Psychopharmacology: June 2006 - Volume 26 - Issue 3 - pp 290-302.
Chick J, Gough K et al. Disulfiram treatment of alcoholism. Br J Psychiatry 1992; 161:84-89.
Chick J et al. United Kingdom Multicentre Acamprosate Study (UKMAS): a 6-month prospective study of acamprosate versus placebo in preventing relapse after withdrawal from alcohol. Alcohol Alcohol 2000 Mar-Apr; 35(2): 176-87
NICE guidance: the NICE guidelines on diagnosis, assessment and management of harmful drinking and alcohol dependence 115. 2011.
Regier DA, Farmer ME et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990 Nov 21;264(19):2511-8.
Berglund M, Ojehagen A. The influence of alcohol drinking and alcohol use disorders on psychiatric disorders and suicidal behaviour. Alcoholism: Clinical and Experimental Research 1998; 22: s333-345.
Stockwell, T., Murphy, D. & Hodgson, R. (1983). The severity of alcohol dependence questionnaire: Its use, reliability and validity. British Journal of Addiction, 78(2), 45-156
Torrens M, Fonseca F, Mateu G, Farré M. Efficacy of antidepressants in substance use disorders with and without comorbid depression. A systematic review and meta-analysis. Drug Alcohol Depend. 2005 Apr 4;78(1):1-22.
Raimo EB, Schuckit MA. Alcohol dependence and mood disorders. Addictive Behaviours 1998; 23: 933-946.
Maudsley guidelines : 10th edition. P197
Edwards,M.E.,& Steinglass,P.(1995).Family therapy treatment outcomes for alcoholism. Journal of Marital and Family Therapy,21(4),475-509.
DSM-IV
Brian L. Burke. The Efficacy of Motivational Interviewing: A Meta-Analysis of Controlled Clinical Trials. Journal of Consulting and Clinical Psychology.2003, Vol. 71, No. 5, 843-861.
 (click to enlarge)
(click to enlarge)
