MENTAL HEALTH
Antipsychotic prescribing for dementia patients
Treating the behavioural and psychological symptoms of dementia is a common example of a difficult prescribing decision
December 1, 2012
-
The NICE guidelines on dementia recommend: “people with Alzheimer’s disease, vascular dementia or mixed dementia with mild to moderate non-cognitive symptoms should not be prescribed antipsychotic drugs because of the possible increased risk of cerebrovascular adverse events and death”.1
The aim of this audit was to measure the number of patients on antipsychotic medication, the indications for initiation, the type of drugs prescribed and how recently the need for the drug had been reviewed. It was hoped to show a reduction in unnecessary prescribing in the second cycle.
Methods
Our practice of three doctors looks after patients in St Mary’s Hospital in Castleblayney, Co Monaghan a nursing home of 115-130 patients. One doctor from the practice attends the nursing home each day. An audit template was designed using the NICE audit support tool from the NICE website.2 This template was completed for each patient by chart and drug kardex review in December 2011.
Dr Feargal Leonard, consultant psychiatrist, who also cares for patients in St Mary’s Hospital, was consulted before and after the first cycle for input from his team. After the first cycle there was a practice meeting to discuss the results, and a policy on antipsychotic prescribing in the nursing home was agreed upon. This included guidelines about starting and discontinuing antipsychotic medication and was based on the NICE guidelines and the best practice guide from the Alzheimer’s Society UK and RCGP.3
There was a meeting with the clinical nurse managers of the nursing home to discuss the results of the first cycle and the new policy document. A laminated copy of the policy was given to each doctor and posted on the wall in each ward. The second cycle was completed in May 2012.
Results
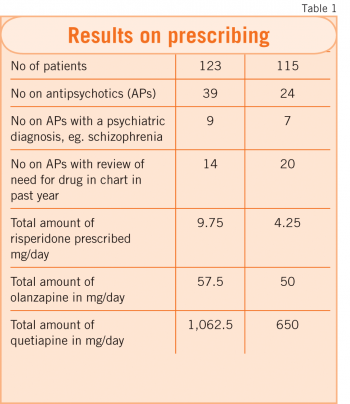
Cycle one (see Table 1)
• Of 123 patients 39 (32%) were on antipsychotic (AP) medication
• Of these patients nine (23%) had a psychiatric diagnosis as an indication for the medication, eg. schizophrenia
• Of the patients on APs, 28% were on risperidone, 33% were on quetiapine and 30% were on olanzapine. The rest of the patients were on haloperidol, amisulpride and chlorpromazine
• 20 (64%) of the patients on APs had a diagnosis of dementia documented in their medical notes
• 26 patients (67%) were on the medication for more than 12 months and in the case of 13 patients (33%) it was unclear how long they had been on the medication
• 27 (69%) had no reason documented in notes for initiation, however, many of these patients seem to have been on the drug when they came to St Mary’s
• 12 patients (31%) had a reason for drug initiation documented. The reasons were agitation, delusions, hallucinations and schizophrenia
• 14 patients (36%) of the patients had a review of drug in past year documented in their medical notes.
Cycle two (see Table 1)
• Of 115 patients 24 (21%) of patients were on AP medication
• 20 (83%) patients had a review of the need for the AP in their chart
• 10 out of 39 patients had had their APs stopped
• Three patients had had their AP stopped and then restarted because of behavioural problems
• Two patients had had their dose reduced and then increased again
• Eight patients had successfully had their dose reduced
• Four patients on APs had died and one had gone home in between the first and second cycle.
Discussion
The rate of antipsychotic prescribing of 32% in the first cycle is comparable to previous studies in the UK and US where it was found 30% of patients in nursing homes were on antipsychotics.4
Risperidone is the only antipsychotic licensed to treat behavioural and psychological symptoms of dementia (BPSD) in Ireland. The European Medicines Agency (EMEA) and UK Medicines and Healthcare products Regulatory Agency (MHRA) have issued warnings about the increased risk of stroke and death and in 2005, the Food and Drug Administration (FDA) issued a ‘black box’ warning.
There is evidence to suggest antipsychotics can help BPSD but the effect is very small. The number needed to treat (NNT) to achieve improvement in one behaviourally disturbed patient range from five to 11. The number needed to harm (NNH) suggests that 100 people with dementia would need to be treated to result in one additional death over 6-12 weeks.5
A recent editorial in the BMJ stated: “Few clinical problems place doctors in as tangled a web of clinical evidence, social policy, and ethical concerns as how to manage behavioural problems in patients with dementia.”6
Indeed, treating the behavioural and psychological symptoms of dementia is a common example of a difficult prescribing decision in general practice. Evidence-based guidelines do not always take into account the complexities of a situation involving patient and carer distress and limited resources and staff numbers in a care setting may limit the non-pharmacological options for treatment.
This audit shows that by implementing a policy on initiation and regular review of antipsychotic medication, prescriptions can be significantly reduced.
Acknowledgements
With thanks to Dr Mary O’Duffy, Dr Michael Clarke and Dr Feargal Leonard. This paper won first prize at the North East GP Scheme audit meeting June 2012.
References
- Dementia NICE guidelines 2006.
- Dementia: the use of medication for non-cognitive symptoms, behaviour that challenges and behaviour control. NICE audit support tool 2009.
- Optimising treatment and care for people with behavioural and psychological symptoms of dementia. A best practice guide for health and social care professionals, Alzheimer’s society UK.
- Time for action, A report for the Minister of State for Care Services by Professor Sube Banerjee.
- Time for action, A report for the Minister of State for Care Services by Professor Sube Banerjee.
- BMJ editorial 2012;344:e1093
 (click to enlarge)
(click to enlarge)

