CHILD HEALTH
Breastfeeding: Breaking down the barriers
The reasons are complex for Ireland's low levels of breastfeeding. However, there are ongoing initiatives which are helping to improve the situation
March 1, 2017
-
Earlier this year, the Lancet published a comprehensive review of breastfeeding. It covered, in detail, the short and long-term health consequences for infants and mothers related to not breastfeeding and the clear evidence supporting these facts.1 Supporting mothers to initiate breastfeeding, breastfeed exclusively and breastfeed for longer durations will help reduce the rates of these illnesses and the associated economic costs. It is important for all healthcare professionals to support the HSE guideline on breastfeeding, which recommends exclusive breastfeeding for six months, followed by the introduction of suitable complementary foods, with continued breastfeeding until two years of age or beyond.
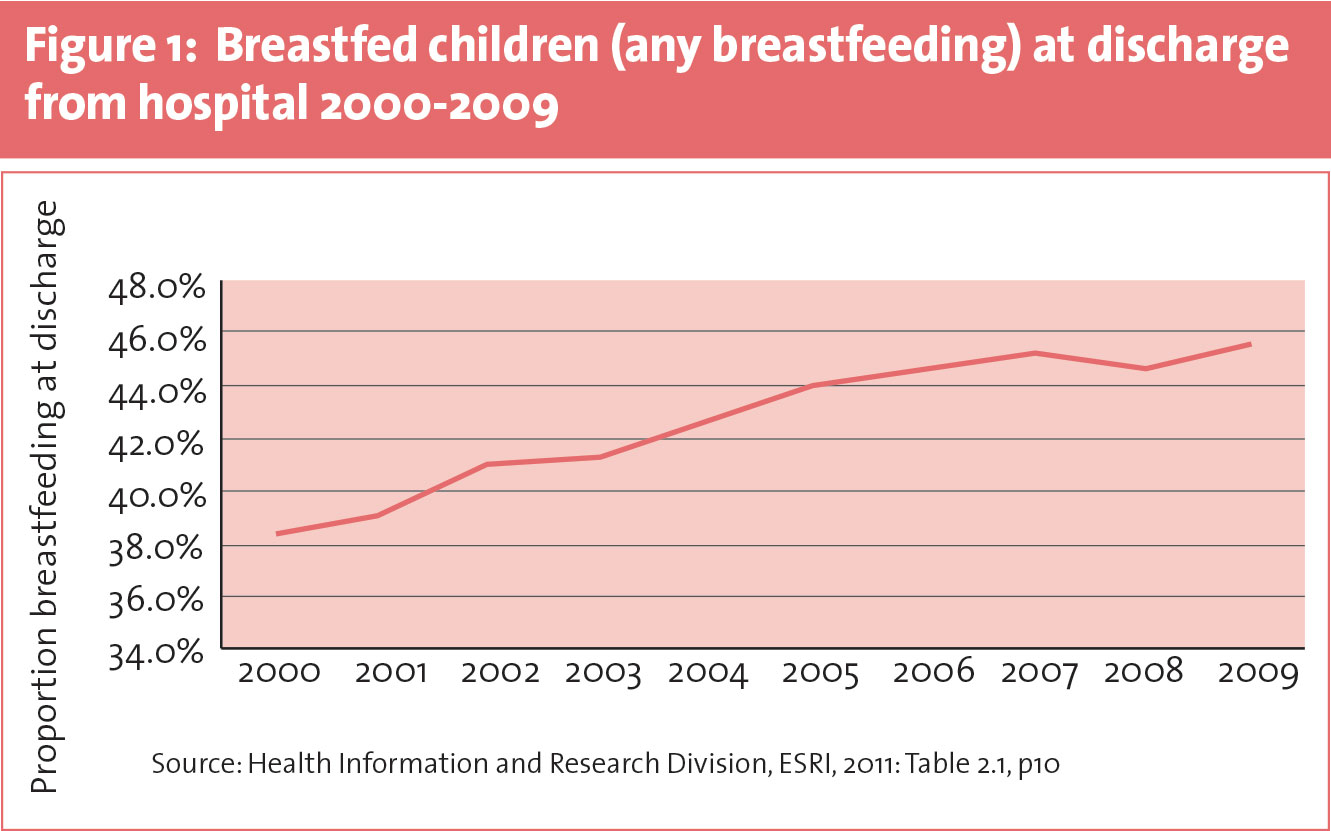
Current breastfeeding rates
The National Perinatal Reporting System has shown that the proportion of infants experiencing any breastfeeding at discharge from Irish maternity hospitals has increased from 38% to 46% over the time period from 2000 to 2009. However, Ireland still has one of the lowest breastfeeding rates in the world with rates much lower than our nearest neighbour the UK (76%), or Sweden (over 90%).2
The data from the Maternal Health Behaviours and Child Growth in Infancy Report from the Growing Up in Ireland (GUI) study3 found that 56% of women breastfed their child to some extent.
Of note, the report found that Irish women were less likely to breastfeed compared to women of all other nationalities who give birth in this country. Another interesting finding on nationality was that the male partner’s nationality was related to the mothers’ decision to breastfeed. The odds of breastfeeding increased by 42% where the male partner was not Irish.
Why women choose not to breastfeed
The main reason found for not breastfeeding in the GUI study was the reported belief that formula feeding was ‘preferable’ for 49% of women. The next two most common reasons were ‘inconvenience/fatigue’ at 17% and ‘difficulty with breastfeeding techniques’ at 8%.
Only 5.6% of mothers in this study reported ‘embarrassment/social stigma’ as the reason why they chose not to breastfed. Women less than 25 years of age were more likely to report this as the reason for not breastfeeding when compared to women aged 35 years or older (9.7% vs 3.4% respectively). This finding is at odds with other Irish studies which have shown much higher rates of women expressing embarrassment around breastfeeding.4
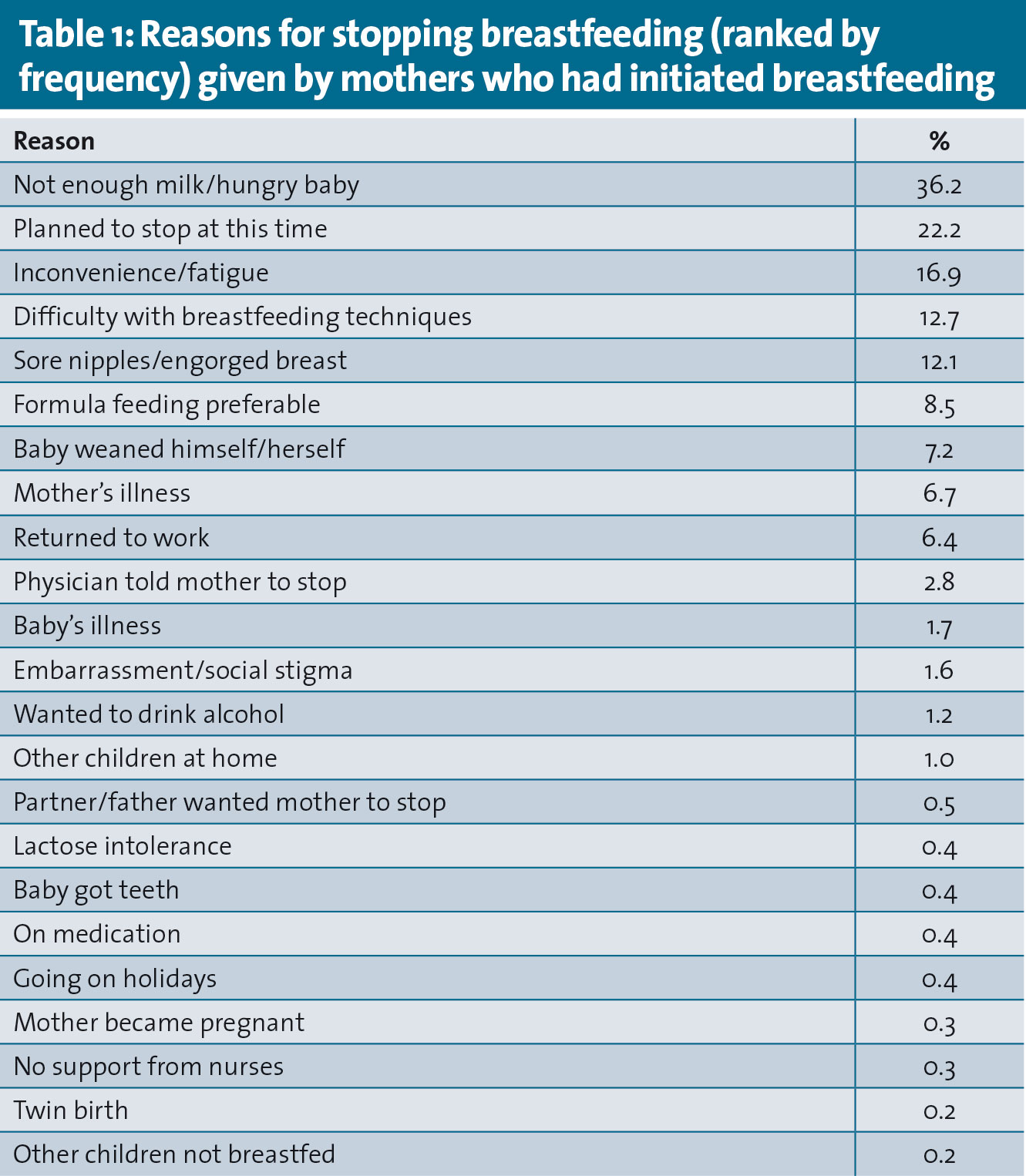
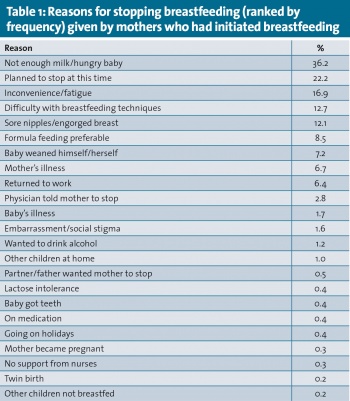
Why women stop breastfeeding
The most common reason for breastfeeding cessation given in the GUI study was the belief that the mother did not produce ‘enough milk’ or that she had a ‘hungry baby’ (36%). The second most common reason was that the mother planned to stop at this point (22%), followed by inconvenience/fatigue (17%).
Many mothers (25%) reported either difficulty with breastfeeding techniques or sore nipples/engorged breasts as other reasons for stopping. The woman’s level of parental stress was also a significant predictor of quitting; each unit increase in stress increased the odds of quitting by 1%.
Women in the GUI study were less likely to stop breastfeeding if they made it through the first month. After this point, the likelihood of stopping falls by around 50% and remains at this level. The likelihood of stopping increases sharply again at six months of age. This change could represent the effect of reaching the end of the standard period of maternity leave. This finding would concur with other research which has found that length of maternity leave is positively associated with duration of breastfeeding and returning to full-time work outside the home is associated with reduced duration of breastfeeding.5
Women of older age, higher income, education and social class were also much more likely to breastfeed and tended to breastfeed for longer. A lower number of previous children was also associated with a higher probability of breastfeeding and a longer duration of breastfeeding. The effect of a number of previous children was confined only to those with three or more previous births.
Supporting breastfeeding
There is extensive evidence to show that children born in hospitals accredited under the WHO’s Baby-Friendly Hospital Initiative are more likely to initiate breastfeeding and to be breastfeeding at discharge from hospital following the birth.5 Only nine of the country’s 19 maternity hospitals are fully accredited at present. The data from the GUI study demonstrated that children born in Baby-Friendly Hospital Initiative-accredited hospitals were 11% more likely to be breastfed than children born in non-accredited hospitals.
A Cochrane review published in 20126 found that a combination of professional and lay/peer supporters is effective in increasing the duration of any breastfeeding and the duration of exclusive breastfeeding. Recent research in Ireland has also shown that first-time mothers depend on healthcare professionals for breastfeeding support.7
Of the top five reasons given for stopping breastfeeding in the GUI study, four were concerns that could be easily addressed by healthcare professionals. The HSE has developed an excellent website, www.breastfeeding.ie, which has factsheets available to download, videos, a list of HSE publications on breastfeeding, which would help guide a breastfeeding mother should she mention any of these issues in a consultation. There is also a list of useful websites where one could direct the mother for further peer support eg. Cuidiú, La Leche League, Friends of Breastfeeding.
Keeping women breastfeeding past the first month helped women breastfeed for longer as identified by the GUI study. Early postnatal checks may be key opportunities for healthcare professionals to offer effective support to mothers to enable them continue to breastfeed.
Conclusion
The Lancet series describe how essential breastfeeding is for building a better world for future generations in all countries, rich and poor alike. Healthcare professionals are well placed to support the breastfeeding mother-infant dyad by offering consistent advice and support that is practical and individualised to their needs.7 There are many resources now available for healthcare professionals to achieve this in a professional capacity or to direct breastfeeding mothers to for peer support.
 (click to enlarge)
(click to enlarge)