Managing patient expectations is a major component in treating chronic pain. Early introduction of a multidisciplinary approach and the use of non-medical as well as physical therapies are important
Dr Justin Lane, Consultant in Pain Medicine, Beacon Hospital, Dublin
Pain has been described as: “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”
We have all heard this definition at one time or another. Chronic pain and associated conditions require further explanation. This goes part of the way to the explanation to why it is not straightforward to manage. Acute painful episodes usually respond to analgesia. The WHO analgesic ladder is the normal approach taken to this type of pain. Sometimes rapid progression up the ladder is necessary.
In chronic pain patients may already be on a combination of analgesia and adjunctive therapies. They may present with new symptoms as part of a progressive disease process (degenerative disc disease of the spine and acute radiculopathy), or worsening of pre-existing symptoms requiring increases in medication (eg. peripheral neuropathy of any origin).
Pain presentations in general practice constitute a large proportion of the contacts with primary care physicians.1 Cooke et al noted along with hypertension, dyslipidaemia, diabetes, immunisations and respiratory tract issues, osteoarthritis and back complaints were in the top 10. This research looked at consultations with some 2,000 GPs over a 12-month period. These latter two pain-related conditions ranked 8th and 9th.
Types of pain presenting in general practice
Osteoarthritis (inflammatory) and back complaints represent a large proportion of consultations in primary care. However, these terms are extremely non-specific and have to be looked at in detail to give a more detailed picture of the types of pain presenting to the surgery in everyday practice.
Pain presentations here refer to those outside of other conditions, (pregnancy, ischaemic heart disease, acute visceral-type pain), which are present in areas of daily practice.
Masters et el looked at 133 consecutive musculoskeletal patients over five weeks.2 These were categorised as; somatic, somatic referred, neuropathic or a combination of all of these. The history in what was a predominantly female group included age, gender, length of attendance, mode of referral, current pain.
Somatic lower back pain was most common (50%), neuropathic (25%) and pure somatic referred in one-in-seven cases (13%).
The two main categories of pain are:
Acute (nociceptive) pain
Chronic (neuropathic) pain.
Nociceptive pain is caused by damage to body tissue and usually described as a sharp, aching, or throbbing pain. Often there is an obvious cause or trigger (injury, fall, associated illness).
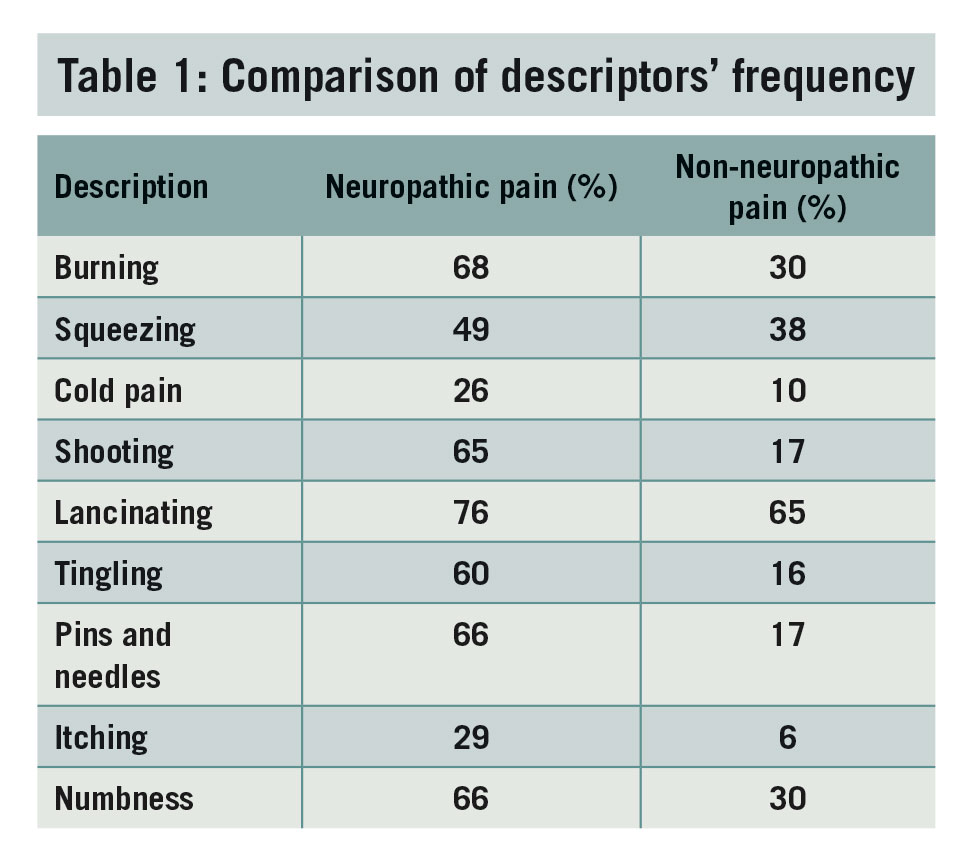
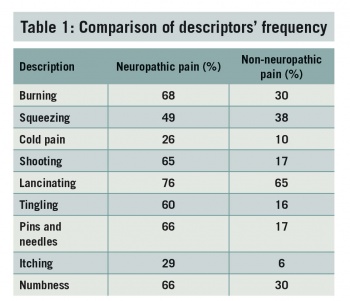
Neuropathic pain occurs when there is actual nerve damage. The clue in this type of pain usually comes from the patient description. The words used usually are quite different from those which are used to describe acute or nociceptive pain. Often words such as burning , itching, tingling, crawling, numb, electric shock, shooting and pressure-like are used to try and describe the sensation.
There can be an overlap of nociceptive and neuropathic symptoms. The identification in diagnosis of neuropathic pain warrants the use of neuropathic medications. Unfortunately the isolation of neuropathic pain diagnosis is difficult, and the treatment options are relatively limited. Commonly mixed agents are used or pure analgesics (eg. opioids), are introduced on an escalating scale.
(click to enlarge)
Essential definitions in pain management3
Nociception: The neural process of encoding noxious stimuli
Nociceptive pain: Pain that arises from actual or threatened damage to non-neural tissue and is due to the activation of nociceptors
Neuralgia: Pain in the distribution of a nerve or nerves
Neuritis: Inflammation of a nerve or nerves
Neuropathic pain: Pain caused by a lesion or disease of the somatosensory nervous system
Neuropathy: A disturbance of function or pathological change in a nerve
Allodynia: Pain due to a stimulus that does not normally provoke pain.
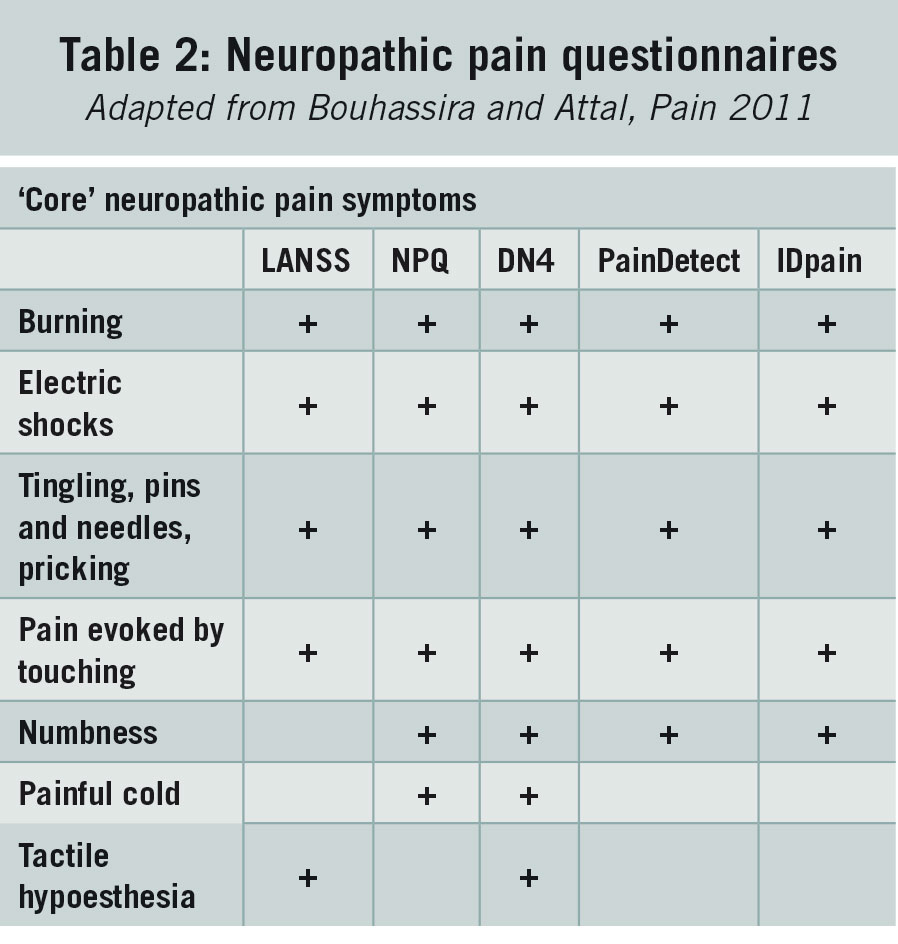
Many questionnaires have been developed in an attempt to simplify and make diagnosing and distinguishing neuropathic pain. Commonly used neuropathic pain questionnaires (see Table 2) attempt to identify the condition with some certainty. This can be helpful in guiding treatment. Two examples are:
The Leeds Assessment of Neuropathic Symptoms and Signs (LANSS)4
Douleur Neuropathique 4 (DN4).5
As with most conditions or clinical situations where there are multiple scoring systems and diagnostic criteria, no one system is without its weakness.
LANSS
This was developed by Bennett in Leeds. It comprises seven items with grouped sensory items and sensory examination, with a straightforward scoring system. The first five questions ask about unpleasant skin sensations (tingling, prickling, pins and needles etc), skin colour and appearance (red, pink, mottled), and increased sensitivity of the skin as well as descriptions of attacks of sudden burning skin sensation or electric-shock like sensation. The last two parts ask about increased sensitivity of the skin when examined, ie. allodynia and altered pin prick sensation threshold.
Maximum score is 24. Scores less than 12 make a diagnosis of neuropathic pain unlikely. Scores greater than 12 make involvement of neuropathic elements in the patient’s pain likely.
The sensitivity is rated at 85% with specificity at 80% and predictive value of 82%. (Sensitivity: how many patients with neuropathic pain test positive? Specificity: a measure of the false positive rate from the test. Positive predictive value: probability that a patient in the population with a positive score has neuropathic pain).6
DN4
This questionnaire was developed by the French Neuropathic Pain Group. Like LANSS, it is an attempt to distinguish neuropathic from non-neuropathic pain. There are 10 questions with sensory descriptors and also signs related to examination.
This questionnaire may be more patient- and time-friendly. There are four sections, each with different components. The final two sections (three questions involved), rely on physical examination to elicit symptoms. A score of 1 is given to each positive, and a score of 0 to each negative. A cut off value of 4/10 is positive for a diagnosis of neuropathic pain. Sensitivity is quoted as 82.9% and specificity at 89.9% by the original group in validation.
Both these tools are useful and well validated in terms of diagnosis .The correct diagnosis or possibly outruling incorrect diagnoses is very valuable in directing possible future treatment.
(click to enlarge)
Stepwise pharmacologic management of NP7
Step 1
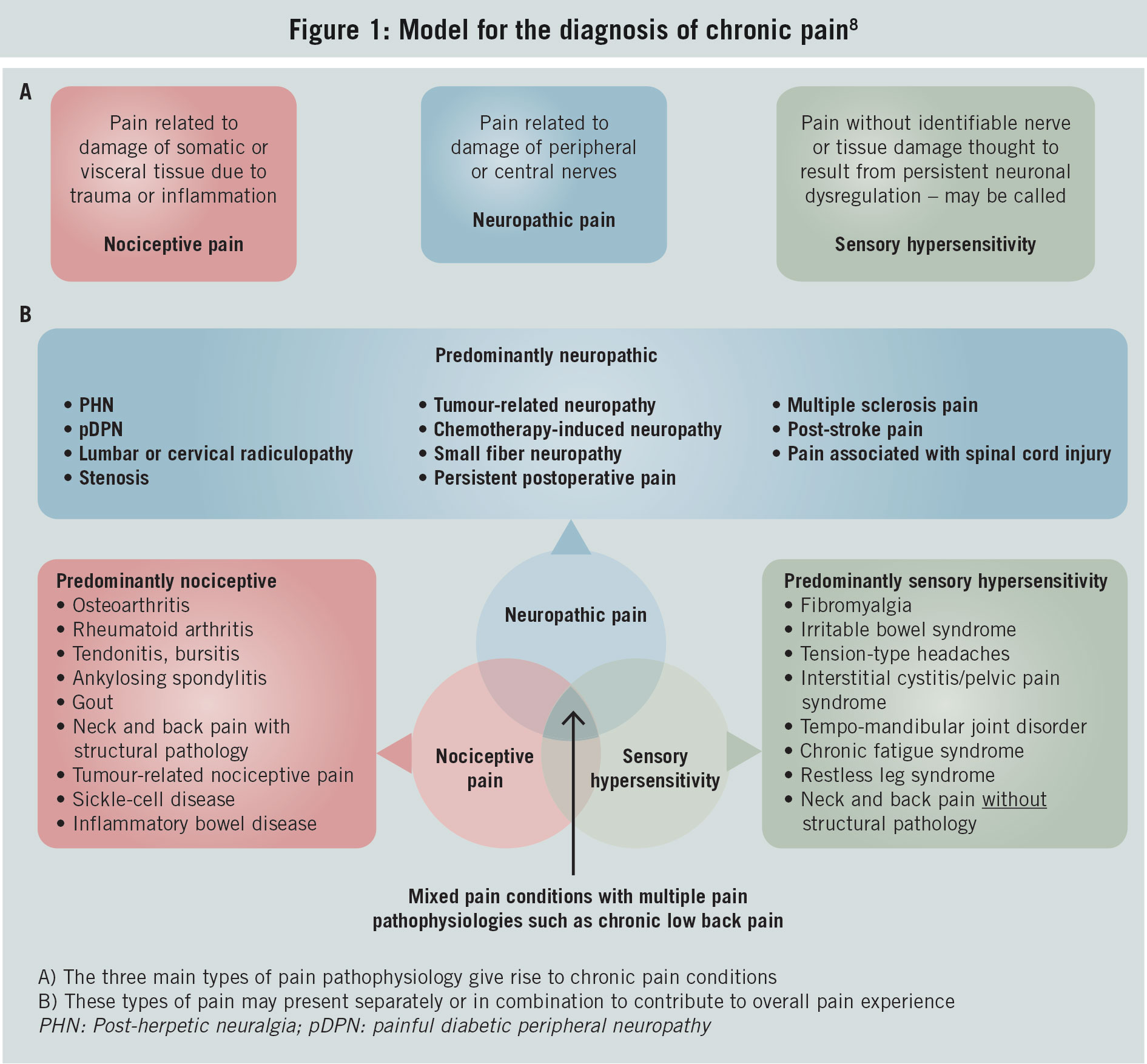
Assess pain and establish the diagnosis of neuropathic pain (NP) through use of questionnaire, eg. DN4 or LANSS. If uncertain about the diagnosis, consider referral to a pain specialist or neurologist. See ‘Model for the diagnosis of chronic pain’ in Figure 1.
(click to enlarge)
Look to rule out ‘red flag’ conditions eg. new onset low back pain in male (PSA?), malignancy, unexplained weight loss, steroid use, fever, incontinence, urinary retention, pain that is increased or unrelieved by rest, intravenous drug abuse (IVDA), immunosuppression.9
Identify relevant comorbidities (eg. cardiac, renal, or hepatic disease, depression, gait instability) that might be relieved or exacerbated by NP treatment, or that might require dosage adjustment or additional monitoring of therapy (eg. BPH, glaucoma and tricyclic antidepressant [TCA] drugs). Explain the diagnosis and treatment plan to the patient, and establish realistic expectations.
It is essential when commencing NP agents to counsel the patient about expected side-effects and the ‘lag’ phase to effect. A prime example is the use of TCA medication. Start at the lowest dose, eg. amitryptyline 10mg. Advise about sedative and anticholinergic effects (dry mouth, blurred vision and urinary retention). The patient is advised to take the dose two hours before bed and to bring a bottle of water to bed, as dry mouth is a common complaint.
A useful strategy is to commence treatment when possible side-effects will be less inconvenient, eg. Friday nights and weekends for people working or doing lots of school runs. The lack of choice in NP agents means that if the patients are not aware of the most common side-effects and the lag to effect (up to six weeks for some agents), you can rapidly run out of options.
Step 2
Initiate therapy of the disease causing NP, and if applicable initiate symptom treatment with one or more of the following:
A secondary amine TCA (amitryptyline, nortriptyline, desipramine) or a selective serotonin and norepinephrine reuptake inhibitor (SSNRI: duloxetine, venlafaxine)
A calcium channel a2-d ligand, either gabapentin or pregabalin
For patients with localised peripheral NP, topical lidocaine used alone or in combination with one of the other first-line therapies
For patients with acute neuropathic pain, neuropathic cancer pain, or episodic exacerbations of severe pain, and when prompt pain relief during titration of a first-line
medication to an efficacious dosage is required, opioid analgesics may be used alone or in combination with one of the first-line therapies. Explain risks of dependence issues with driving, mobility and co-prescribe laxative/stool softeners. It is wise to limit duration of opiate prescriptions to a minimum required to allow the NP agent to work.•
Evaluate patient for non-pharmacologic treatments, and initiate if appropriate.
Step 3
Reassess pain and health-related quality of life. If there is substantial pain relief and tolerable side-effects, continue treatment. If there is only partial pain relief (eg. average pain remains 4/10) after an adequate trial, add one of the other first-line medications. If there is no or inadequate pain relief (eg. < 30% reduction) at target dosage after an adequate trial, switch to an alternative first-line medication.
Step 4
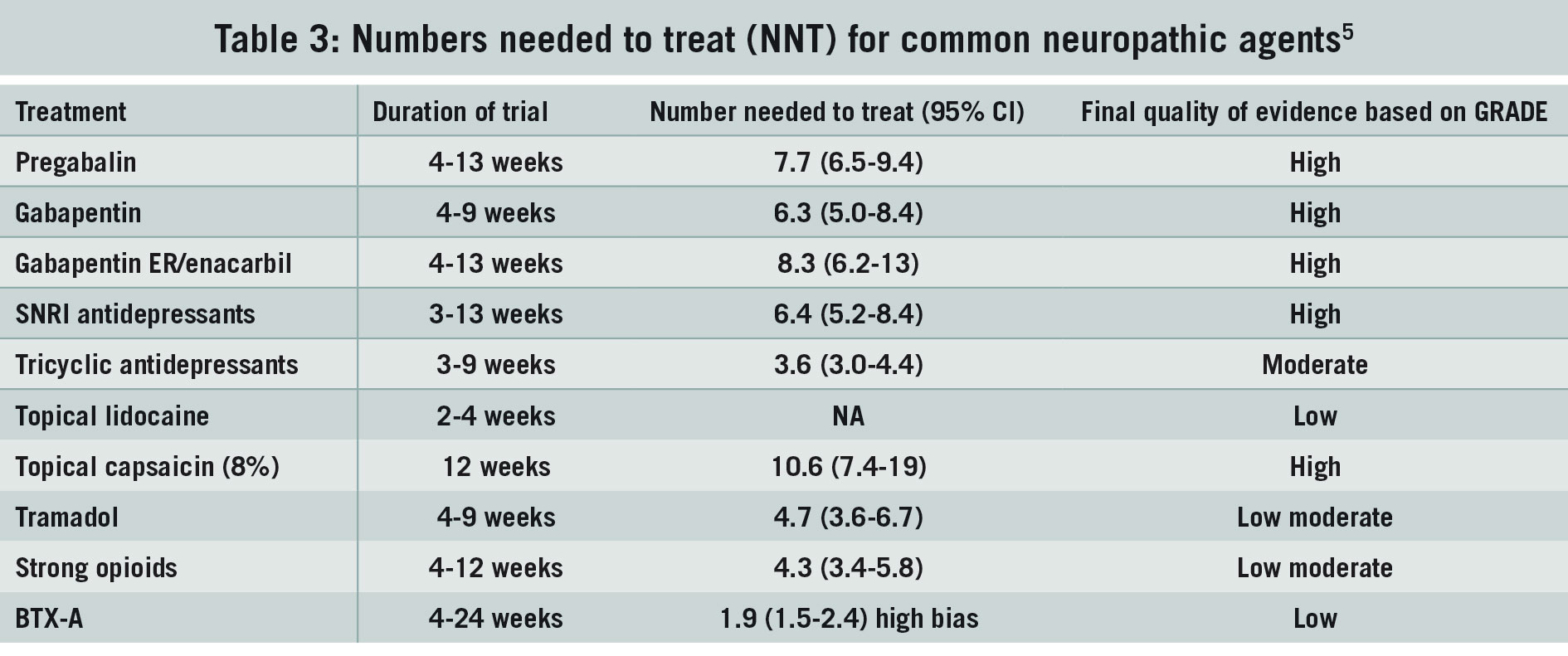
If trials of first-line medications alone and in combination fail, consider second- and third-line medications or referral to a pain specialist (see Table 3).
(click to enlarge)
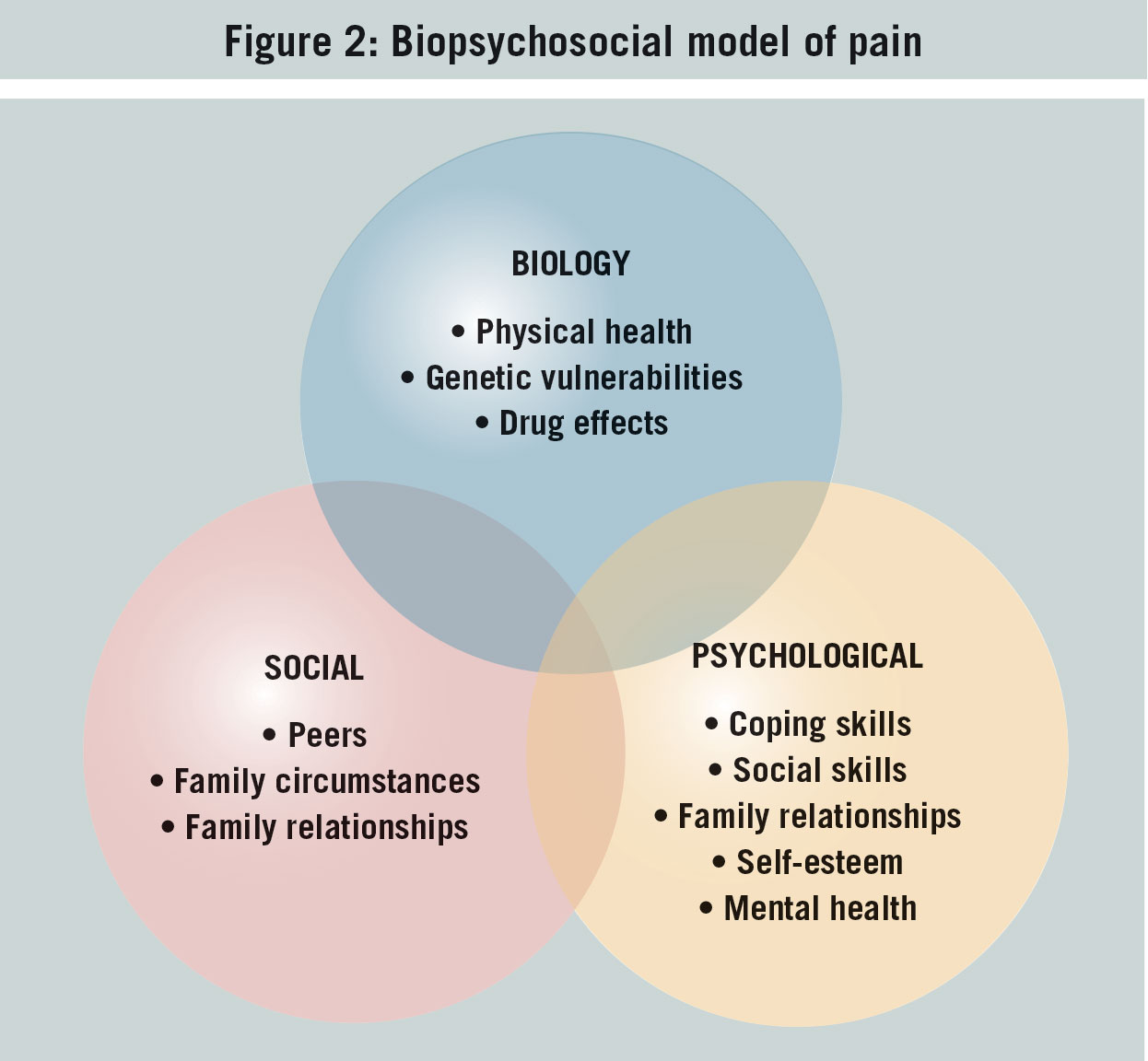
Biopsychosocial model of health applied to pain
This model was first described by Engel in 1977.11 Originally it was perceived as being about the causation and the biological, psychological and social contributions to illness and disease (see Figure 2). Later discussions identified the three components in how disease is manifest in patients.
(click to enlarge)
The biological component may cause the physical manifestation, however the psychological make-up of the patient may determine his or her reaction to the condition.
The social component reflects how the social circumstances of the patient may in turn determine the progress and engagement of the patient in therapy. This will ultimately determine the outcome for the patient.
This can be the same in many chronic illnesses. Patient, family and societal perception of conditions and diagnoses can alter the way the individual interacts with healthcare providers and treatment. This then affects outcome.
This can form the basis for the famed ‘multidisciplinary’ team approach to chronic pain. The concept of psychological involvement in treating and assessing pain is still an unwelcome conversation with patients. Like the physical and pharmacological treatments, it is an essential part of chronic pain and most chronic conditions.
Using coping strategies, CBT or mindfulness is a part of treatment. Once a diagnosis is made, early discussion of this area is a good idea. This allows the patient to absorb the idea that their problem is a little more than a pill or injection away from cure.
Evidence-based management
A large part of the management of any chronic disease is in managing expectations. The patient’s hope is often complete pain relief and unfortunately this is rare. This results in a change in our role from aiming for a ‘cure’ to optimising pain relief as far as possible.
The emphasis is also on improved function within the boundaries of the pain relief achieved. In a busy practice this may not always be possible.
The time resource required may not be realistic for one individual practitioner. The multidisciplinary approach including roles for psychology, physiotherapy, occupational therapy and mindfulness is important. Early introduction of these concepts and treatment arms is essential.
Other difficult realities need to be addressed. The management of chronic back pain in overweight, sedentary smokers without addressing lifestyle issues is unlikely to succeed. In my experience the realisation of ‘ownership’ of the pain problem is important in order to get the patient involved in their pain management.
SIGN guidelines13 emphasise the need for a multidisciplinary team approach to improve outcomes, and highlights five broad categories of care:
Supported self-management
Drug treatment
Psychological based interventions
Physical therapies
Complementary therapies.
Exercise, regardless of its type and the source of pain, is recommended for the management of chronic pain. In chronic low back pain, exercise therapy can improve strength and range of motion across joints, cardio-respiratory fitness and sense of wellbeing.
Conclusions
Pain consultations represent a large proportion of primary care interactions. Accurate identification and classification of pain diagnoses in combination with setting realistic expectations provides confidence to the doctor and their patient about planned treatment. Early identification of ‘red flags’ is essential, as any of these should trigger urgent assessment and investigation at secondary care level.
Unfortunately the ‘ideal’, example of multidisciplinary pain units and programmes, alluded to in peer reviewed journal content, is not too common in Irish hospitals. This often means more complex cases must commence treatment in general practice. The use of LANSS and DN4 is useful in this scenario. They are concise and are therefore suited to clinic consultation.
In practice, using a stepwise approach to medical therapy allows planning and may help in confirming diagnosis. The importance of counselling the patient about the time to treatment effect and common side effects cannot be stressed enough.
Rapid progression through the neuropathic agents will leave the practitioner with limited options and possibly maintenance opioids. Some newer agents have evidence of efficacy in mixed neuropathic and nociceptive pain without, as yet, reports of addiction or dependance. These may be a better option in the primary care setting when moderate to strong analgesics are needed.14
Managing patient expectations is still a major component in treating chronic pain. The early introduction of the multidisciplinary approach and the use of non-medical as well as physical therapies are important as they can be approaches the patients may take time to appreciate.
References
Cooke et al. Common general practice presentations and publication frequency. Australian Family Physician. 2013; 42(1): 65-68
Masters S., Lind R. Musculoskeletal pain. Presentations to general practice. Australian Family Physician. 2010: 39(6): 425-428
www.iasp-pain.org/Taxonomy
Bennett et al. The LANNS pain scale. Pain. 2001; 92(1-2): 147-57
Bouhassira D et al. Comparision of pain syndromes assoicated with nervous or somatic lesions and develoment of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005; 114(1-2): 29-36
www.getthediagnosis.org
R.H. Dworkin et al. Pharmacologic management of neuropathic pain. Pain. 2007; 132: 237-251 Adapted.
Stanos et al. Rethinking chronic pain in a primary care setting. Postgraduate Medicine. 2016; 128(5): 502-515
Bratton, RL. Assessment and management of acute low back pain. Am Fam Physician. 1999; 60(8): 2299-308).
Engel, George L. The need for a new medical model: A challenge for biomedicine. Science. 1977; 196(4286): 129-136
Engel, George. The need for a new medical model: A challenge for biomedicine. Science. 196: 129-136
Govenden DI, Serpell M. Improving outcomes for chronic pain in primary care. Practitioner. 2014; 258(1774): 13-7
Colvin, LA et al. Managing chronic pain: a clinical challenge. New SIGN guidelines provide a practical evidence-based approach and identify research gaps. British Journal of Anaesthesia. 2014; 112 (1): 9-12. On behalf of the SIGN Chronic Pain guideline development group
Dart et al. Assessment of the abuse of tapentadol immeidate release: the first 24 months. J Opioid Management. 2012; 8(6): 395-402
 (click to enlarge)
(click to enlarge)