Percutaneous Endoscopic Gastrostomy (PEG) tube is an important means to provide enteral nutrition in a selected subgroup of patients. The decision for PEG insertion is usually made after a clear multidisciplinary discussion with patients and families. There are many medical conditions that would warrant consideration for PEG feeding, but the crucial decision lies on the risks and benefits of each specific situation with full involvement and discussion by physicians with patients and families. Multidisciplinary care and educational programmes have been found to reduce the numbers of patients receiving feeding tubes inappropriately.1
The American Medical Directors Association, American Geriatrics Society and American Academy of Hospice and Palliative Medicine recommend against inserting PEG in individuals with advanced dementia and instead, recommend oral assisted feedings.2,3,4
Aims and methods
This retrospective study aimed to assess the patient cohort in Connolly Hospital, Blanchardstown, Dublin who have had a PEG tube inserted endoscopically between January 2014 and August 2015.
We evaluated the indications, specialty of physicians involved, time frame between presentation of illness to PEG insertion, patient age, sedation used and any immediate complications related to the procedure.
We obtained data from the EndoRAAD database (endoscopy reporting system), medical chart review and phone contact to relatives and general practitioners.
Results
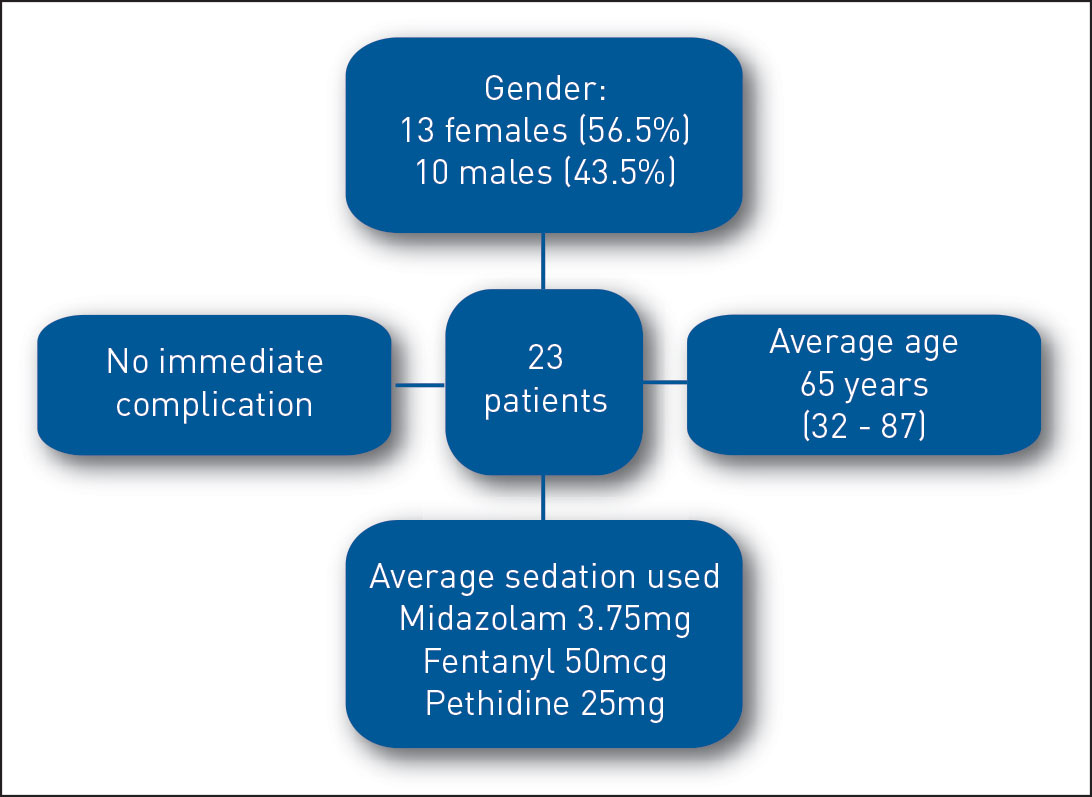
A total of 23 patients had PEG inserted endoscopically, 13 females (56.5%) and 10 males (43.5%) as compared to 27 patients in the previous 20 months. Comparatively, there were six cases of radiologically inserted gastrostomy (RIG) during the corresponding 20 month period. The average age was 65 years (32-87). The average midazolam dose was 3.75mg, fentanyl 50mcg and pethidine 25mg. There were no documented immediate complications (see Figure 1).
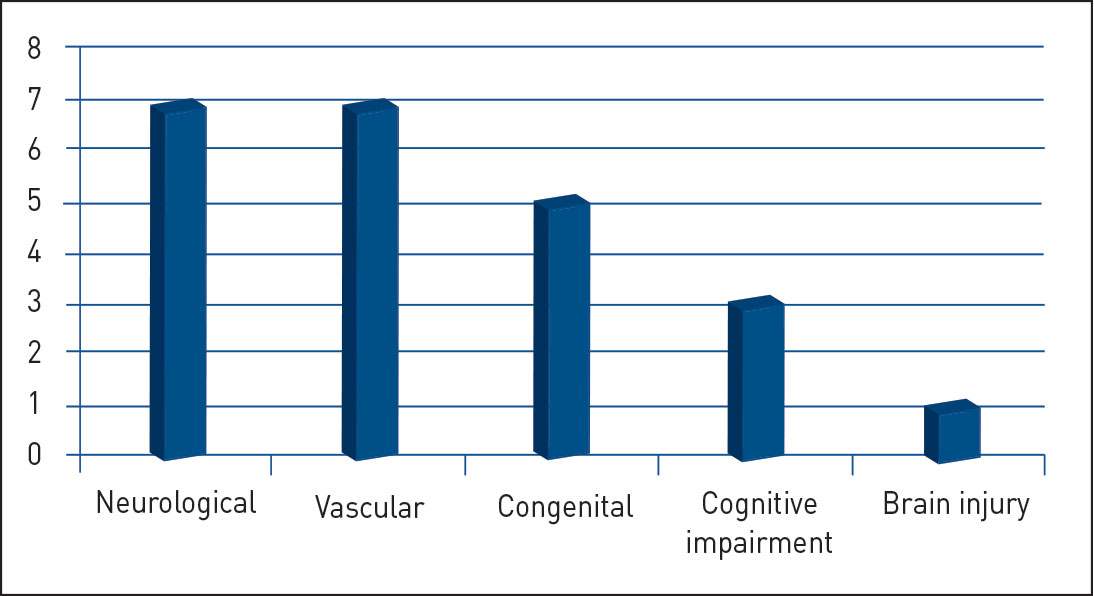
Figure 2. Indications for PEG insertion(click to enlarge)
The decision for PEG insertion was made by stroke physicians (n = 6, 26%) and other medical physicians (n = 17, 74%) (neurologists, gastroenterologists, primary physicians).
Timeframe from diagnosis to PEG insertion was understandably variable. The only definitive timing was for severe stroke patients with average duration of five weeks.
Discussion
Although success rates greater than 95% have been reported for PEG, procedure-related complications are common.5 The risks of PEG insertion include immediate and delayed complications and these are discussed thoroughly with patients and family prior to the decision to go ahead with PEG insertion. Immediate complications (within 72 hours) for PEG include:6
Endoscopy-related:
– Haemorrhage or perforation
– Aspiration
– Oversedation
Procedure-related:
– Ileus
– Pneumoperitoneum
– Wound infection
– Wound bleeding
– Injury to the liver, bowel or spleen
Delayed complications, such as:
– Gastric outlet obstruction
– Buried bumper syndrome (migration of the internal bumper of the PEG tube into the gastric or abdominal wall)
– Dislodged PEG tube
– Peritonitis
– Peristomal leakage or infection
– Skin or gastric ulceration
– Blocked PEG tube
– Tube degradation
– Gastric fistula after removal of the PEG tube
– Granulation around site of insertion of the PEG tube.
PEG used for feeding in conditions associated with swallowing disorders, ie. neurological causes, will reduce the risk of aspiration pneumonia but will not eliminate the risk entirely. PEG insertion should be performed with the aim of an improvement in quality of life rather than just maintaining life.2,3,4
Conclusion
PEG feeding provides an important treatment intervention when used in the right patient cohort. Multidisciplinary involvement is crucial in the decision making process. Our retrospective study showed that our patients were carefully selected and procedures were performed with minimal levels of sedation without immediate complication. We plan to prospectively assess all referrals for PEG tube to ensure clear and appropriate patient selection at all times.
References
Monteleoni C, Clark E. Using rapid-cycle quality improvement methodology to reduce feeding tubes in patients with advanced dementia: before and after study. BMJ 2004(Aug 28); 329(7464):491-494
Feeding tubes for people with Alzheimer’s disease: When you need them – and when you don’t. Retrieved 6 December 2013. White Paper on Surrogate Decision-Making and Advance Care Planning in Long-Term Care. American Medical Directors Association
Daniel K, Rhodes R, Vitale C, Shega J. Feeding Tubes in Advanced Dementia Position Statement. American Geriatrics Society 2013 (May)
Buff D. Against the flow: Tube feeding and survival in patients with dementia. American Academy of Hospice and Palliative Medicine 2006 (Spring); Bulletin 7 (1)
Pender SM, Courtney MG, Rajan E et al. Percutaneous endoscopic gastrostomy; results of an Irish single unit series. Ir J Med Sci 1993; 162:452-455
Kurien M, McAlindon ME, Westaby D et al. Percutaneous endoscopic gastrostomy (PEG) feeding. BMJ 2010 May 7; 340:c2414. doi: 10.1136/bmj.c2414
 Figure 1. PEG study data(click to enlarge)
Figure 1. PEG study data(click to enlarge)