Current thinking on urinary tract infections in children
An update on the management of urinary tract infections in children, incorporating the latest national and international guidelines
Prof Alf Nicholson, Consultant Paediatrician, RCSI Department of Paediatrics, Children’s University Hospital, Dublin, Dr Michael Riordan, Paediatric Nephrologist, Children’s University Hospital, Temple Street and Our Lady’s Children’s Hospital Crumlin, Dublin, Dublin and Dr Robert Cunney, Consultant Microbiologist, Children’s University Hospital, Temple Street, Dublin
Urinary tract infections (UTIs) are relatively common in childhood and are more frequently seen in girls. UTIs may be difficult to diagnose in infants as symptoms are often non-specific, such as fever, irritability and poor feeding, with consequent poor weight gain. One in 10 girls and one in 30 boys will have a UTI before their 16th birthday. Common bacterial causes are Escherichia coli, Proteus, Klebsiella and Enterococcus.
New revised NICE guidelines were published in August 2017,1 the American Academy of Paediatrics reaffirmed their 2011 guidelines in 20162 and national guidelines have recently been agreed in Ireland. This article reflects these recent developments.
Presenting symptoms
Presenting symptoms are age-related. In infants under six months of age, presenting symptoms may be relatively non-specific with fever, vomiting, lethargy, irritability and poor feeding with consequent failure to thrive. Occasionally, young infants may have jaundice or offensive urine or a poor urinary flow.
Infants and children over six months up to the age of two may present with poor feeding, vomiting, loin tenderness and abdominal pain and occasionally they may also have offensive urine with obvious macroscopic haematuria.
In children who have been toilet trained, the most common symptoms are frequency, dysuria, dysfunctional voiding, day time enuresis, abdominal pain and loin tenderness. Depending on whether they have acute pyelonephritis or not, they may have fever and constitutional symptoms. They may also present with an offensive-smelling urine or cloudy urine.
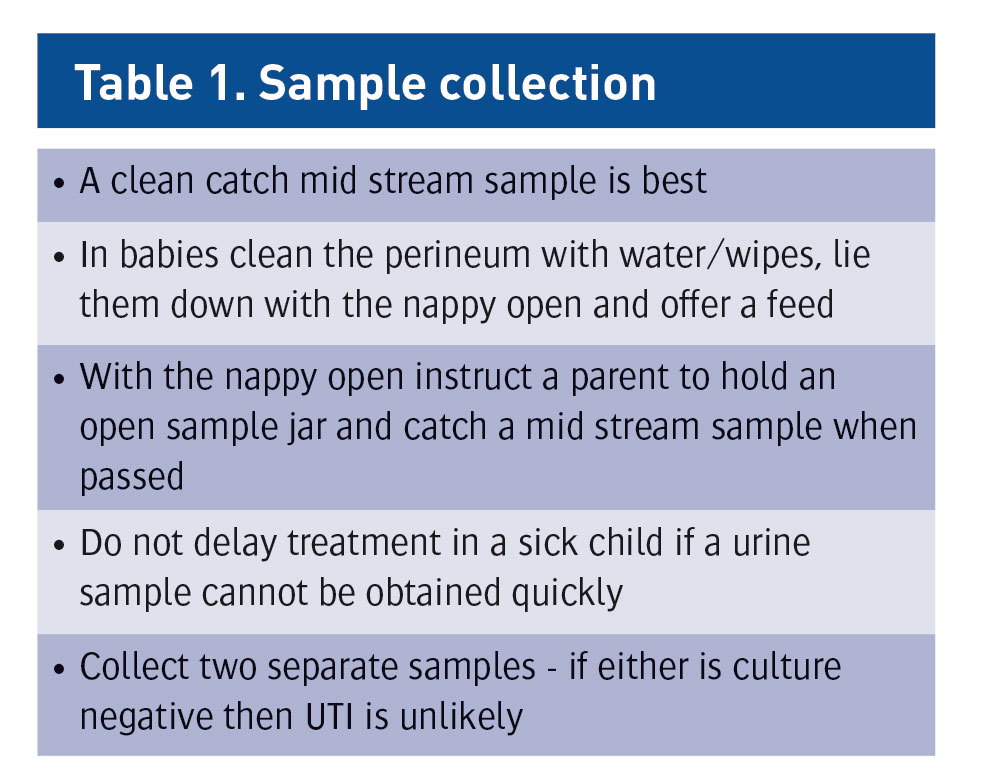
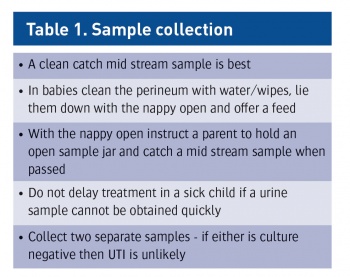
Urine collection
Urine collection is challenging in young children. It is of great importance as a clean catch urine specimen is the recommended method for urine collection. If a clean catch urine is not obtainable, other non-invasive measures such as urine collection bags can be used but are associated with frequent false positive cultures. It is important to follow the manufacturer’s instructions when using urine collection bags. Cotton wool balls, gauze or sanitary towels should not be used to collect urine in infants and children. It is not possible or practical to collect urine by invasive methods, such as a catheter sample or suprapubic aspirate in general practice. In an emergency department setting, if a suprapubic aspirate is being attempted, ultrasound guidance should be used to demonstrate the presence of urine within the bladder.
It is not necessary to send ‘test of cure’ urine samples in children who have had a good clinical response to antibiotic treatment of UTI. Urine preservation is equally challenging. Often a urine sample may be collected out of hours and will not go to the laboratory for some time. In this situation, the sample should be refrigerated immediately.
(click to enlarge)
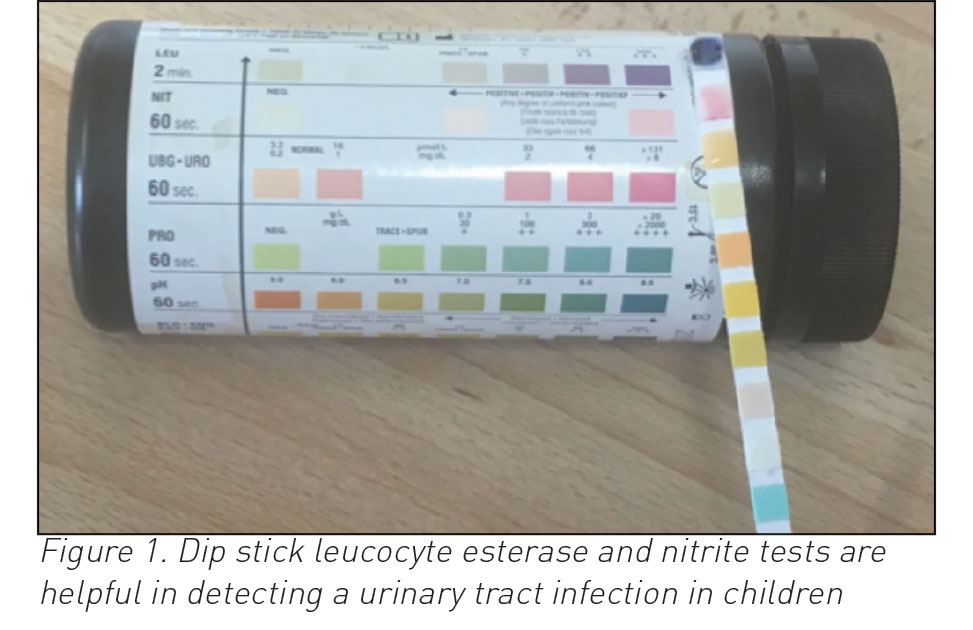
Dip stick testing
Dip stick testing is very helpful and can be used in infants and children with a suspected UTI:
If leucocyte esterase and nitrite tests are both positive, a UTI is highly likely and antibiotic treatment should be started and urine sent for culture.
If the leucocyte esterase is positive and nitrite negative, check that the sample is fresh and if so send a culture and treat with antibiotics
If the leucocyte esterase is positive and the nitrite is negative, examine for vulvitis or balanitis and only treat if obvious urinary symptoms
If leucocyte esterase and nitrite tests are both negative, the child should not be considered to have a UTI. There is no need to start antibiotic therapy or indeed to send a urine sample for culture and sensitivity
Infants under three months of age have relatively dilute urine and therefore a negative dipstick test does not exclude UTI in this age group.
In summary, a urine sample should be sent from primary care for culture in infants and children:
Who are suspected of having acute pyelonephritis
If at higher risk of serious illness, ie. in all infants under three months of age
If a positive test for leucocyte esterase or nitrite test on dipstick testing.
Key points in the history
The following key questions should be asked in relation to a young child with UTI. Firstly, enquire about urinary flow. Ask about a history suggestive of previous UTIs, recurrent fevers or previously picked up renal anomalies. Ask regarding a family history of vesico-ureteric reflux (VUR) or renal disease. Enquire regarding co-incident constipation or dysfunctional voiding, especially in girls post toilet training.
(click to enlarge)
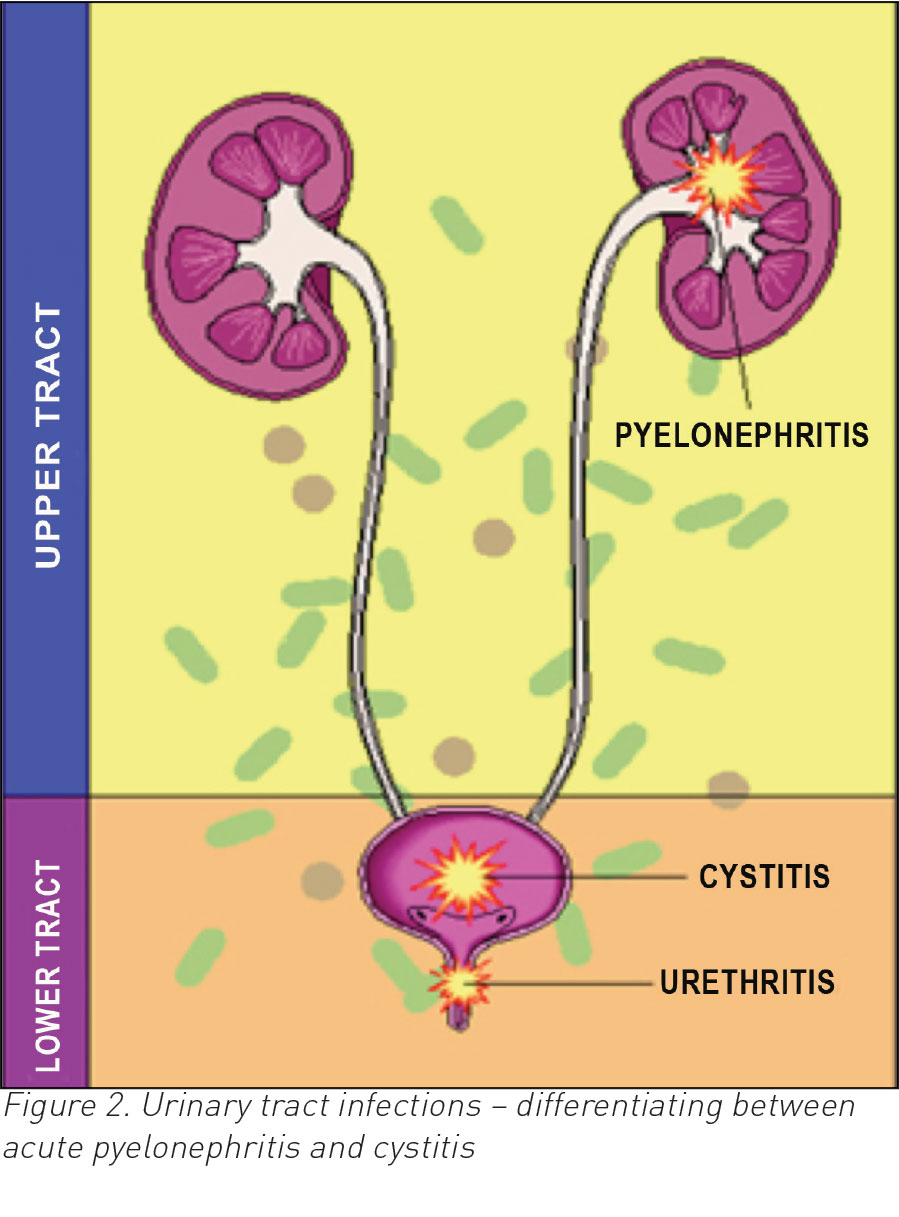
Acute pyelonephritis and cystitis
It is important to differentiate between acute pyelonephritis and cystitis. Infants and children with significant bacteriuria, loin tenderness and fever above 38°C, should be considered as having acute pyelonephritis or upper urinary tract infection. Children with bacteriuria, who have symptoms or signs suggestive of UTI but none of the above systemic features, should be considered as having cystitis or a low urinary tract infection (see Figure 2).
(click to enlarge)
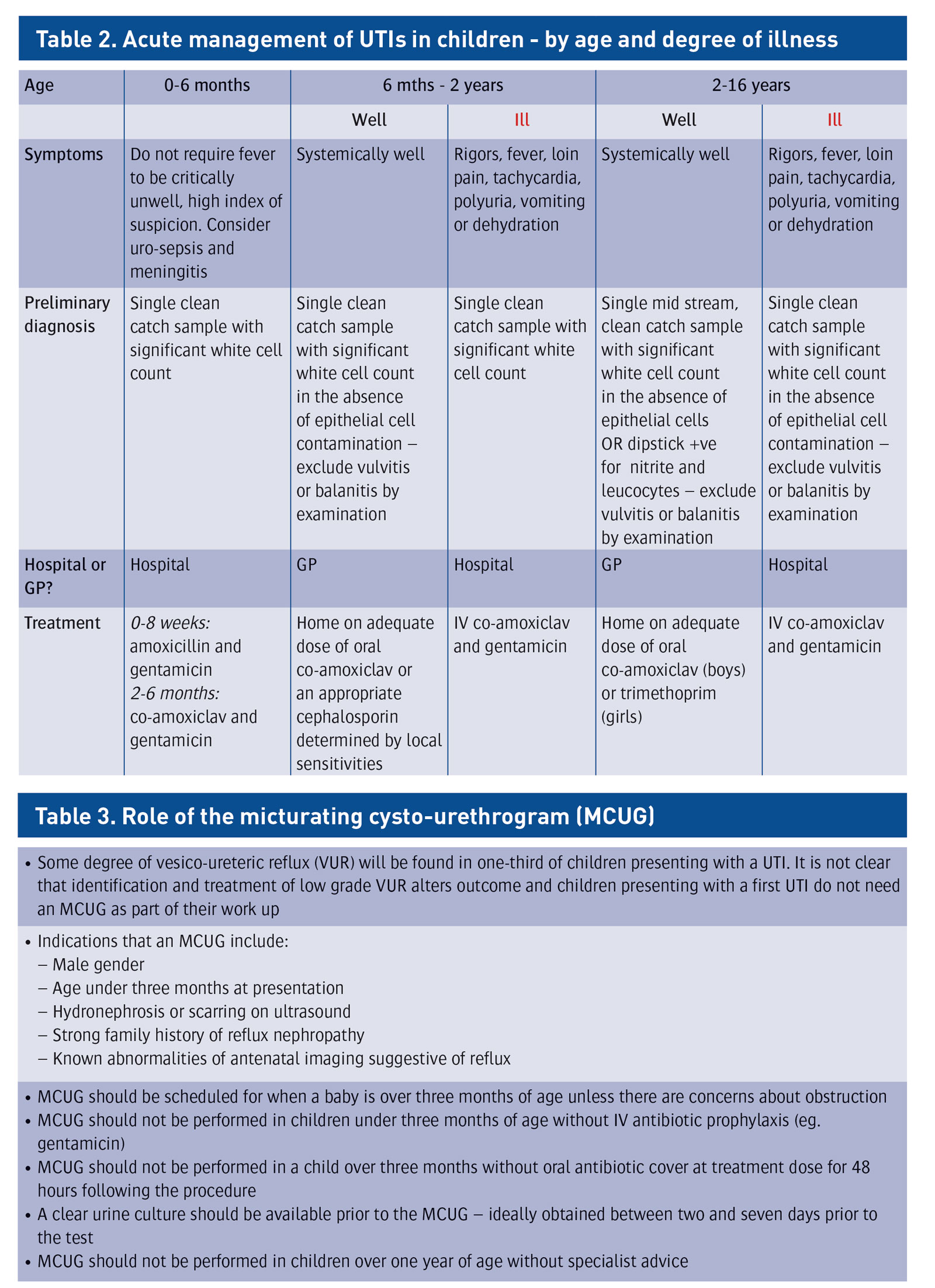
Acute management
Acute management relates to age and whether ill or not (see Table 2). Febrile infants under six months of age with a possible UTI should be referred immediately to the emergency department with a view to admission. Treatment should be with intravenous antibiotics. For infants over six months, treatment should be with oral antibiotics for seven to 10 days. The use of oral antibiotics with low resistance patterns is recommended.
The www.antibioticprescribing.ie website5 recommends trimethoprim, cephalexin or nitrofurantoin for lower UTI or co-amoxiclav for upper UTI. If oral antibiotics cannot be used, treat with intravenous amoxicillin and gentamycin or co-amoxiclav and gentamycin.
For infants and children six months or older with cystitis or lower urinary tract infection, treat with oral antibiotics for three days. Trimethoprim, nutrofurantoin and cephalosporin may be suitable and the parents should be advised to bring the infant/child for re-assessment if the child is unwell after 24-48 hours. Dysfunctional voiding and constipation should be treated to ensure reduction in occurrences.
Consider antibiotic prophylaxis post-UTI only in cases of documented recurrent UTI or high grade vesico-ureteric reflux and, if prophylaxis considered necessary, use narrow spectrum antibiotics (trimethoprim or nitrofurantoin) for a limited time period (maximum three to six months).4
(click to enlarge)
Imaging investigations
For infants under the age of six months with a urinary tract infection an ultrasound should be carried out. For those over six months with a first time UTI that responds well to treatment, routine ultrasound scan is not recommended. Some degree of vesico-ureteric reflux will be found in up to one-third of children presenting with UTI, but it is not clear that identification and management of mild reflux (grades 1 and 2 ) improves outcomes.
Micturating cystogram should not be performed routinely but should be considered if the following features are present:
Dilatation on ultrasound scan (hydronephrosis and hydroureter) suggestive of reflux
Renal scarring
Poor urine flow
Recurrent infection
Under three months at first presentation
Strong family history of reflux nephropathy.
Ultrasound scanning in a toilet trained child should be performed with a full bladder with an estimated bladder volume before and after micturition.
Significance of vesicoureteric reflux3
In a recent major review, micturating cysto-urethrogram (MCUG) is the diagnostic test for vesico-ureteric reflux (VUR) but is now almost exclusively reserved for infants under six months of age. Longterm complications of VUR include endstage renal failure (ESRF) (1 in 10,000), but not high BP or PET in pregnancy. There is a high rate of spontaneous resolution of VUR and no benefits from surgery or longterm antibiotic prophylaxis.
When is specialist or hospital referral indicated ?
Referral to general paediatrics is indicated if either recurrent infections or atypical infections. Recurrent infections are defined as more than one proven urinary tract infection with symptoms based on two separate episodes at which urine culture demonstrates a pure growth of a single organism from an appropriately collected sample.
Atypical infections are defined as those with a significant systemic illness, poor urine flow, abnormal renal function, abdominal or bladder mass, septicaemia or bacteraemia with a positive blood culture, infection with a non-E. coli organism, a strong family history of kidney problems or abnormal antenatal renal imaging.
Discuss with nephro-urology if:
Children under two years of age with recurrent UTI
Imaging suggests urinary obstruction, significant hydronephrosis, single kidney, significant unilateral scarring/dysplasia, calculi or bilateral renal abnormality
Poor urine output or/raised serum creatinine
Palpable bladder or abdominal mass.
What can we offer as advice based on latest guidelines?
A positive urine dip stick test for leucocyte esterase and nitrate in children over three months of age greatly increases the likelihood of finding a positive urine culture. Sending only positive dipstick samples for culture offers a better balance of benefits and cost for these children than prescribing antibiotics and sending a urine culture for all children. All children under six months of age should be referred for specialist paediatric care if urinary tract infection is suspected.
In those infants and children three months or older but younger than three years, symptoms are easier to identify and antibiotics should only be started if a dip stick test is positive for either or both leucocyte esterase or nitrites. Children in this age group with a positive dip stick, should have a urine sample sent for culture.
New UTI guidelines in Ireland are consistent with NICE guidelines and reflect a reduced emphasis on MCUG, which effectively is now restricted to infants under six month olds with a documented UTI.
References
NICE clinical guideline 2017 (nice.org.uk/guidance/cg54 ). Urinary tract infection in under 16 year olds : diagnosis and management
Reaffirmation of AAP Clinical Practice Guideline: The diagnosis and management of the initial urinary tract infection in febrile infants and young children 2-24 months of age. Subcommittee on Urinary Tract Infection 2016 ; 138(6)e20163026;DOI : 10.1542/peds 2016-3026
Tullus K. Vesico-ureteric reflux. Lancet 2015; 385:371-378
Urinary Tract Infections in infants and children : diagnosis and management. Robinson JC, et al. Paediatr Child Health 2014; 19(6) : 315-319
www.antibioticprescribing.ie. Management of urinary tract infections in children
 (click to enlarge)
(click to enlarge)