Current treatment advances in traumatic brain injury
Significant positive developments in relation to traumatic brain injury (TBI), often referred to as a silent epidemic, are forthcoming with the publication of the Major Trauma Audit in Ireland currently underway
Dr Áine Carroll, National Director Clinical Strategy and Programmes, HSE Consultant in Rehabilitation Medicine, National Rehabilitation Hospital, Dun Laoghaire, Co Dublin and Dr Amanda Carty, Programme Manager, Brain Injury and Stroke, National Rehabilitation Hospital, Dun Laoghaire, Co Dublin
Traumatic brain injury (TBI) is defined by the US Centre for Disease Control and Prevention (CDC) as an occurrence of an injury to the head with one or more of the following attributable to the head injury:
Decreased level of consciousness
Amnesia
Skull fracture
A neurological, neurophysiological or intracranial
lesion
OR
An occurrence of death from trauma with head injury listed in the sequence of conditions leading to death.1
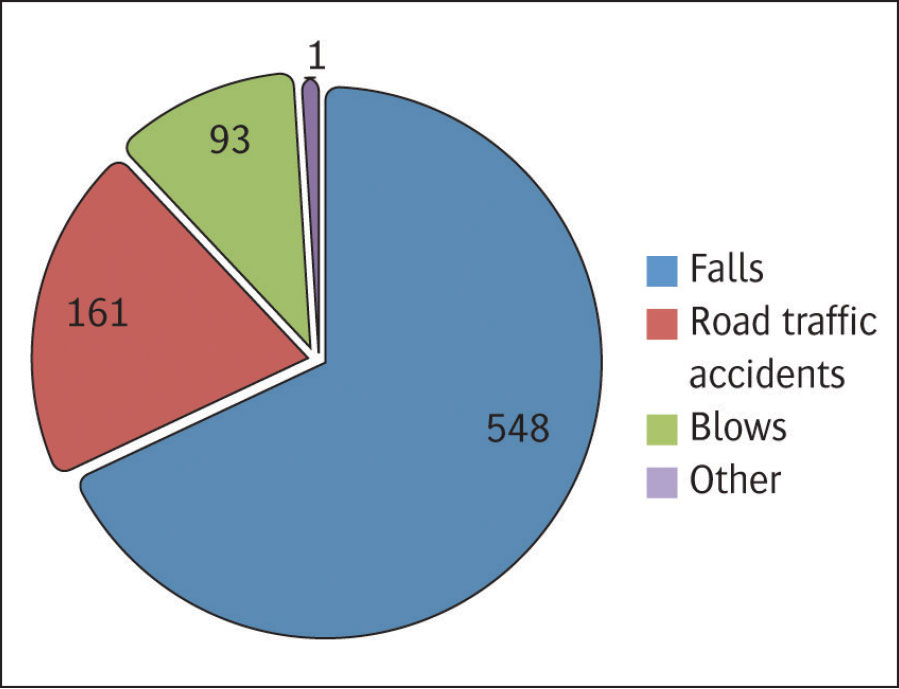
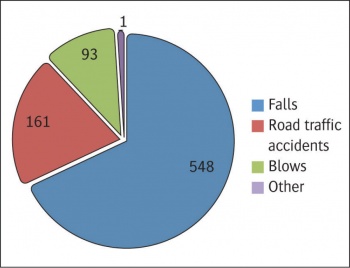
Complete figures on the incidence of traumatic brain injury are lacking in Ireland but several reports have acknowledged that traumatic brain injury is a major cause of premature death and disability in the Republic of Ireland.2 The National Office of Clinical Audit (NOCA) is now collecting trauma data, through the major trauma audit (MTA) that aims to deliver accurate data for Ireland for the first time. The MTA will help inform and develop strategy, measure the impact of changes and will be a vital quality assurance, quality improvement and research tool. TBI figures obtained through the MTA for 2014 show 813 recorded TBIs. The causes of these are illustrated in Figure 1.3
Incidence and causes of TBI in Ireland 2014. Data from the National Office of Clinical Audit, Major Trauma Audit 2016(click to enlarge)
It is estimated that across Europe there is an average incidence of TBI of approximately 235 per 100,000 with most countries experiencing an incidence in the range of 150-300 / 100,000 per year.4 This international incidence would suggest that the Irish figures given above appear to be low and therefore incomplete. TBI is acknowledged to be the main cause of death and disability in the population under the age of 455 and accounts for a significant proportion of emergency department (ED) and pre-hospital workload. It is generally accepted that 10% of ED attendances are because of head injury, of which 10% are admitted and of which 10% need neurosurgical care.6,7
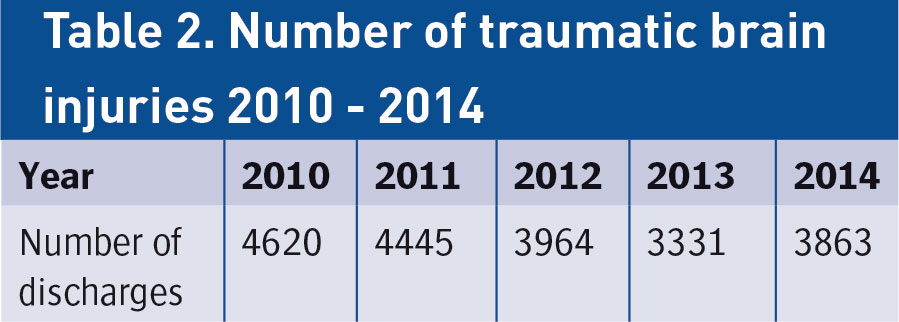
The hospital inpatient enquiry scheme (HIPE) data, provided by the Hospital Pricing Office (HPO), is the best source of Irish data. The figures include data from all publicly funded hospitals which were included on the HIPE system from 2010-2014.8 To date 2015 figures are not yet available. It is important to note that this data is based on hospital discharges only. Furthermore, the data is based on hospitalisations which may include multiple admissions for the same patient. Therefore, the data presented here cannot be construed as the absolute prevalence of tbi in Ireland but may represent a reasonable estimate.
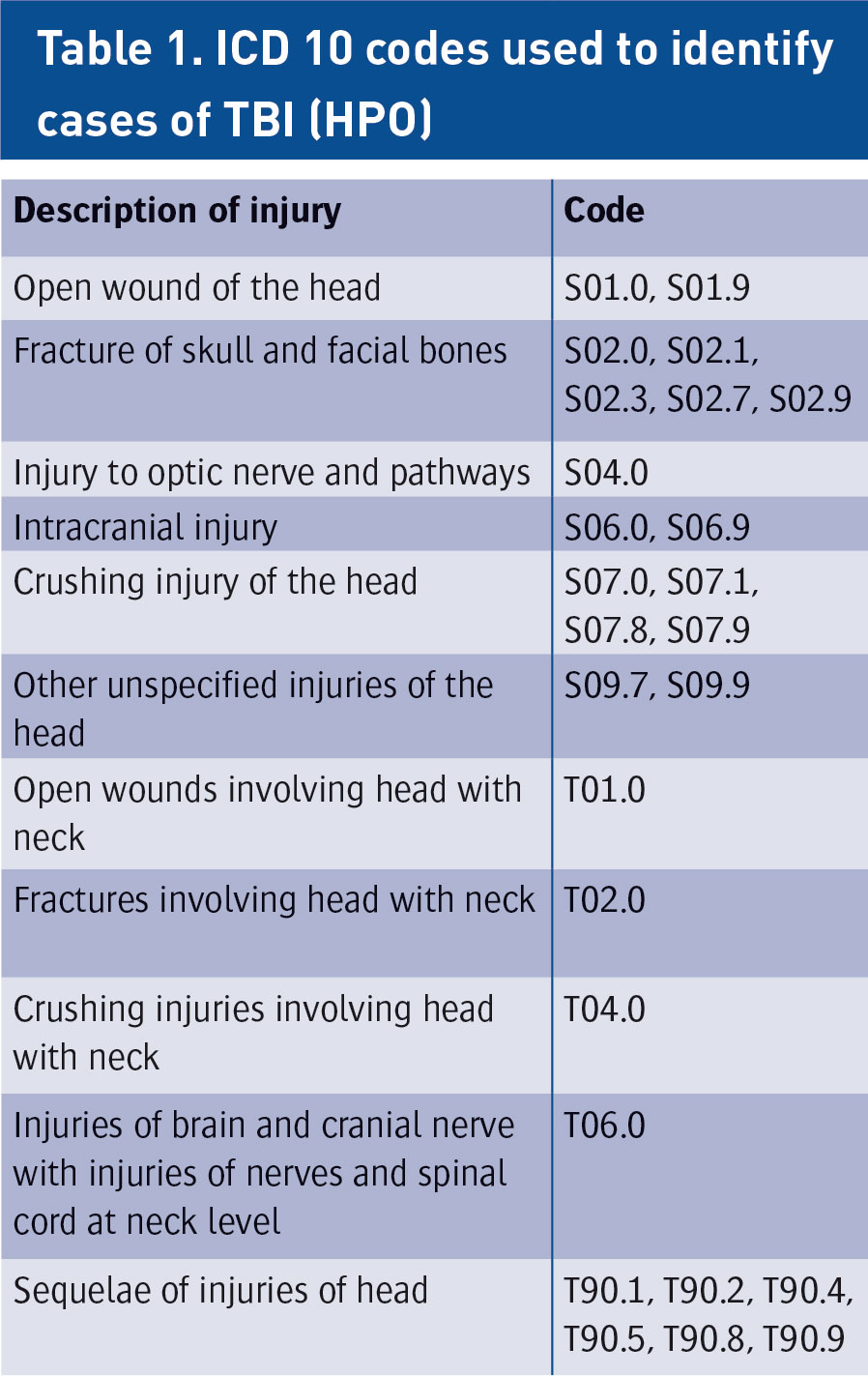
Table 1 shows the codes that were used to identify cases of TBI. Table 2 shows the number of traumatic brain injuries for the period 2010-2014.7
(click to enlarge)
(click to enlarge)
Although case fatality is low, trauma is the leading cause of death under the age of 45 and up to 50% of these are due to a head injury.9 Up to half of all inpatient adults with a head injury experience long term psychological and/or physical disability, especially if definitive therapy is delayed.10,11,12,13
Classification of TBI
TBI can be classified in numerous ways, including type, severity, location, mechanism of injury and physiological response to injury. This heterogeneity is considered to be one of the most significant barriers to establishing effective therapeutic interventions in TBI.14
Efforts in the US and the UK to standardise the naming, definitions and classification of TBI subgroups have the potential to reduce the variability in data coding and improve the quality of data gathering in TBI research. However, it is generally accepted that biomechanical and neuropathological methods of classifying TBI are helpful in determining therapeutic intervention.
The principal mechanisms of TBI are classified as:
(a) Focal – due to contact injury types resulting in contusion, laceration and intracranial haemorrhage or
(b) Diffuse – due to acceleration/deceleration injury types resulting in diffuse axonal injury or brain swelling.15,16,17
The outcome from TBI
The outcome from TBI is determined by two different stages:
The primary insult that occurs at the moment of impact. This type of injury is sensitive to preventive but not therapeutic measures
The secondary insult, which represents consequent pathological processes, which although initiated at the moment of injury, may have delayed clinical presentation.
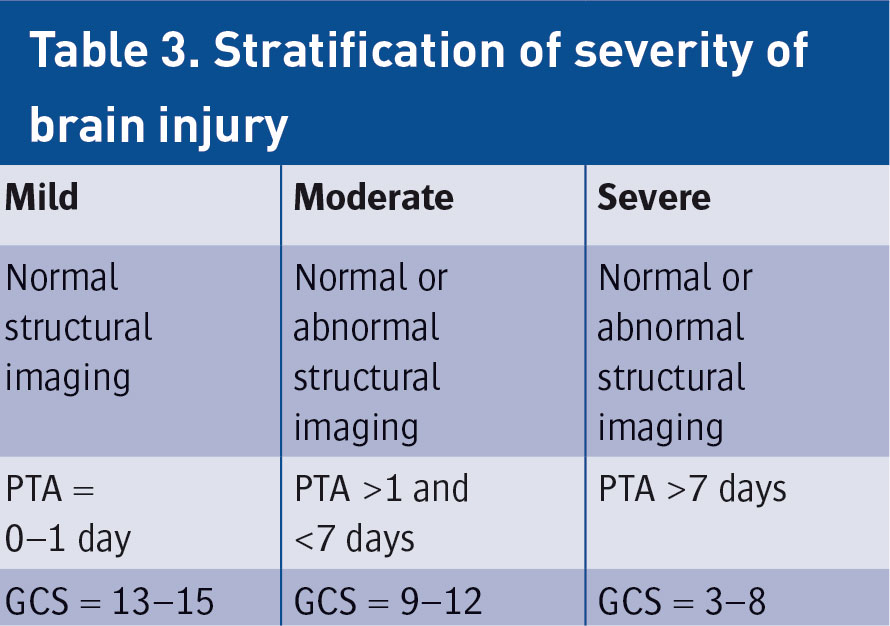
This results from delayed biochemical, metabolic and cellular changes that are initiated by the primary event. There is therefore a therapeutic window for pharmacological or other treatments to prevent progressive tissue damage and improve outcome. The Glasgow Coma Scale (GCS) and duration of post-traumatic amnesia (PTA) are often used to stratify injury severity as shown in Table 3. It should be noted, however, that GCS and PTA are only weakly related to long-term outcome in individual patients.18,19
(click to enlarge)
Causes
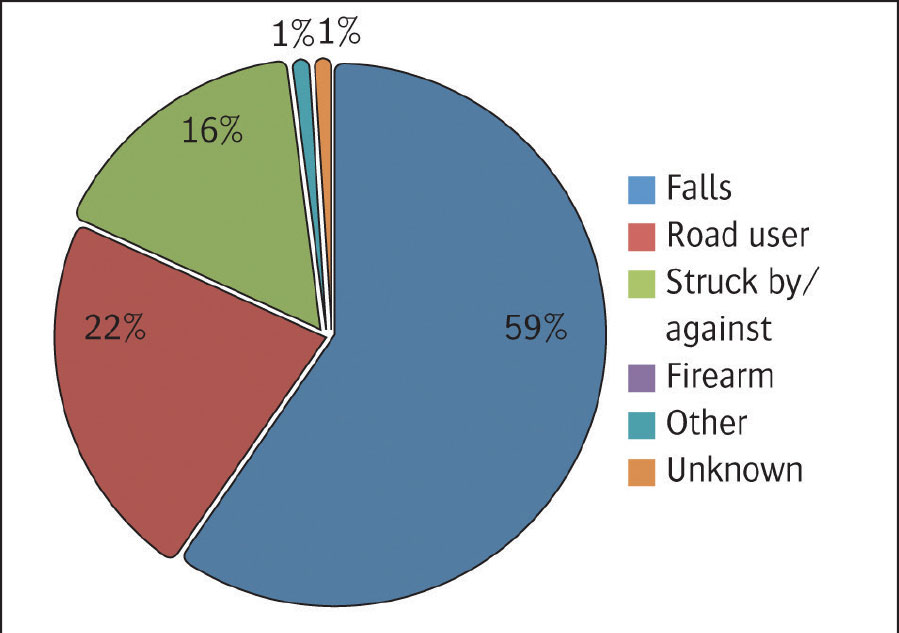
Unfortunately, as indicated above, there are currently no traumatic brain injury databases in Ireland. The Phillips report in 2008 demonstrated that falls were responsible for the majority of injuries for both male and female patients at 59% of all TBI occurrences, thus far outweighing road users (22%) and all other causes (Figure 2).
Cause of TBI – Philips report 2008(click to enlarge)
According to Shivaji et al, in Scotland in 2014, with respect to the causes of TBI admission, by far the leading cause was falls (47%). Next were assaults (18%) however in the age group 15-34, violent causes are the predominant cause of injury, accounting for 40% of hospitalisations.20
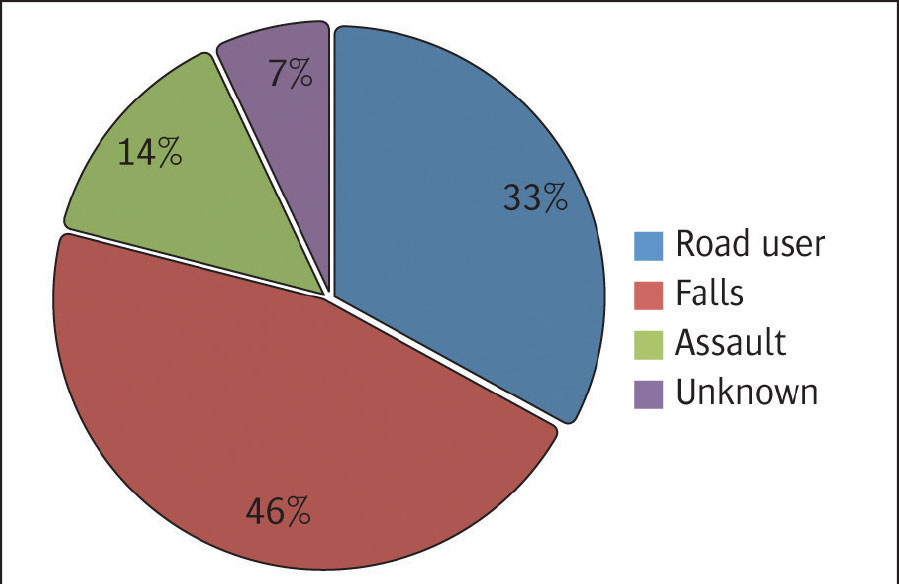
While there is no Irish TBI database, the causes of TBI in patients discharged from the National Rehabilitation Hospital (NRH), the national tertiary brain injury rehabilitation provider, in 2015 are illustrated in Figure 3. The figures reflect the above findings with falls accounting for the highest number of TBIs at 46%. Road accidents accounted for the next largest cause, accounting for one third of all TBIs. Assault figures are close to the Scottish findings at 14% (NRH unpublished data 2015). It should be considered however, that this only addresses TBI patients who were discharged from NRH over two years rather than all traumatic brain injury cases for these years.21
Figure 3. Cause of TBI- NRH discharges 2014-2015(click to enlarge)
Sequelae
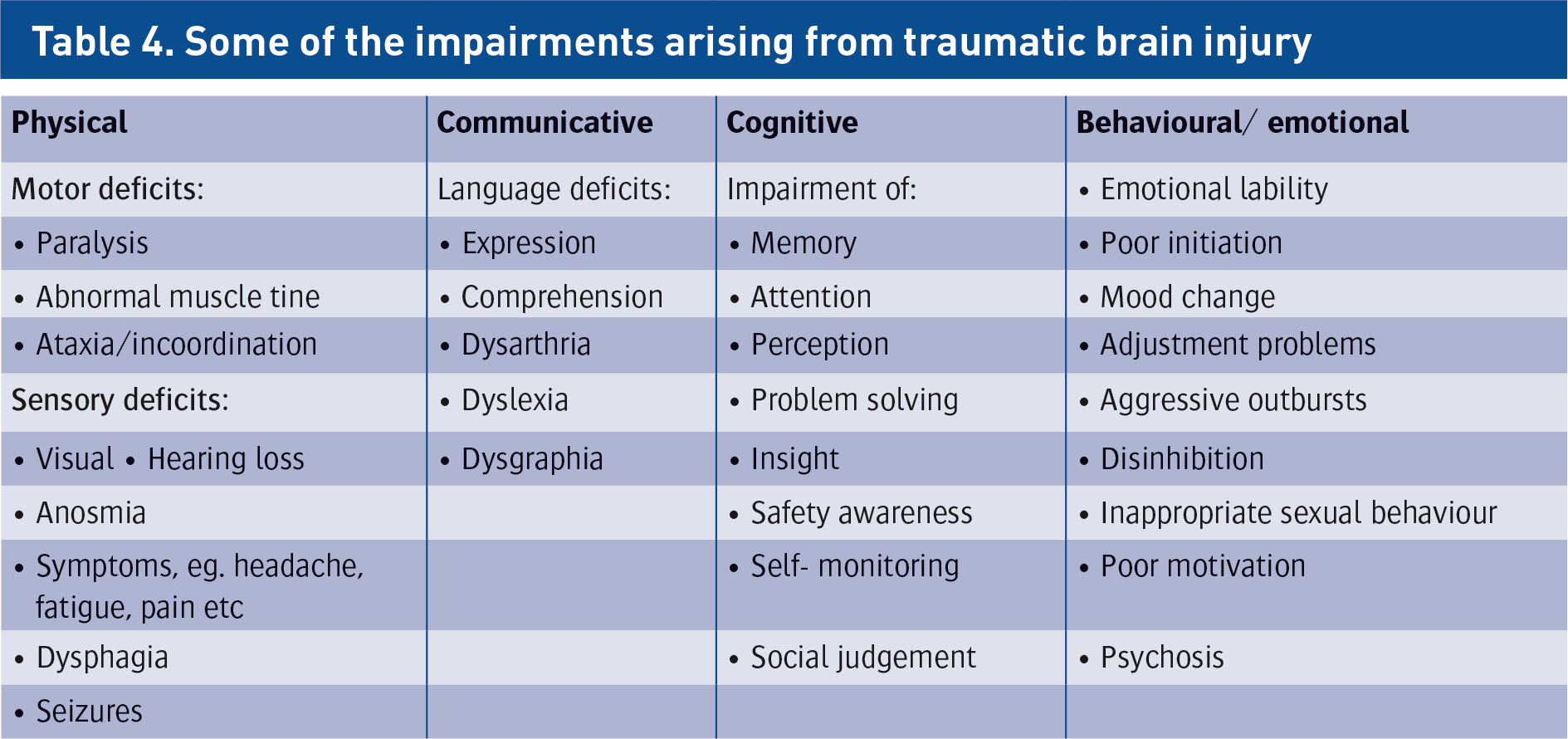
Depending on the nature and location of injury, patients with TBI can present with a wide range of problems.22 These can be broadly divided into the categories listed in Table 4.
(click to enlarge)
Management of traumatic brain injury
Basic science research has greatly advanced knowledge of the mechanisms involved in secondary damage, creating opportunities for medical intervention and targeted therapies; however, translating this research into patient benefit remains a challenge. Clinical management has become much more structured and evidence based since the publication of guidelines covering many aspects of care. It is clear that evidence based guidelines can help to achieve optimal care.
Unfortunately, there are currently no Irish guidelines on the management of TBI nor is there a nationally accepted or adopted guideline. The emergency medicine programme (HSE/RCSI) is developing a national care pathway in collaboration with other specialties and programmes. There are currently no centres in Ireland that meet the criteria to be a level 1 trauma centre (access to acute specialist rehabilitation being absent currently). Since the first Guidelines for Management of TBI were published in 1995, there have been several studies clearly demonstrating that management of TBI in accordance with the guidelines can achieve substantially better outcomes, such as improved functional outcome scores and reduced mortality rate, length of hospital stay and costs. Patel et al unequivocally showed a 2.15 times increase in the odds of death (adjusted for case mix) for patients with severe head injury treated in non-neurosurgical centres versus neurosurgical centres.23
Their report makes a strong case for transferring and treating all patients with severe head injury in a setting with 24-hour neurosurgical facilities. Most neurosurgical centres in the UK and Ireland are not equipped to receive all patients with TBI because of shortages in human and technical resources24 and patients with TBI are referred only for selected surgical indications. In light of this it could be suggested that all treatable patients with TBI should be centralised in large neurotrauma centres that offer surgical therapy and access to specialised neurocritical care.25,26 However, this cannot be achieved without significant reconfiguration of services and reallocation of resources.27
Prehospital care
The main goals of prehospital management are to prevent secondary insult and therefore appropriate advanced life support approaches are advised. No benefits have yet been shown for hypertonic solutions, albumin or hypothermia.27,28,29
Admission care
The primary aims of admission care are stabilisation and diagnostic assessment with prioritisation according to advanced trauma life support standards. The essential aims of neuroimaging after TBI are to assist in prevention of secondary damage, to emphasise favourable biomarkers with potential for neurodegenerative disease detection, and to obtain prognostic information about long-term outcome.
The American Journal of Radiology in 2015 advised that advanced neuroimaging techniques show promising results in group comparison analyses; however, there is still a lack of evidence supporting the routine clinical use of advanced neuroimaging for diagnosis and/or prognostication at the individual patient level.30
Intensive care management
The main object of intensive care management is to optimise cerebral perfusion and oxygenation to prevent secondary insult and create the optimum conditions for recovery. Monitoring of ICP, optimum oxygenation, perfusion, nutrition, glycaemic control and temperature control are all required, as is good glycaemic control.
Decompressive craniectomy
Despite having been used for over a century, decompressive craniectomy (DC) remains a controversial procedure with many complications. Two trials are currently ongoing: the RESCUEicp (randomised evaluation of surgery in craniectomy for uncontrollable elevation of intracranial pressure) study in Europe and the DECRA (decompressive craniectomy) study in Australia, which should hopefully end the controversy.31,32
Monitoring of the severely injured brain
There has been considerable debate about the effectiveness of ICP monitoring in TBI. The consensus, however, is that regardless of technique (of which there are many) no monitoring technique can improve outcome unless it triggers an appropriate response when an abnormality is detected. A good review in the International Journal of Molecular Sciences in 2015 provides a comprehensive review on the current literature and advises that the future in monitoring seeks for non-invasive methods with equal accuracy as invasive techniques.32
Neuroprotection
Despite being heralded as the ‘next big thing’ in TBI, and although preclinical studies have suggested many promising pharmacological agents to prevent secondary injury, unfortunately nearly all phase II/III clinical trials in neuroprotection have failed to show any consistent improvement in outcome for TBI patients.33,34,35,36
There are a large number of exciting translational research developments in this area. Promising drug or cell-based therapeutic approaches include erythropoietin and its carbamylated form, statins, bone marrow stromal cells, stem cells singularly or in combination with biomaterials to reduce brain injury via neuroprotection and promote brain remodelling via angiogenesis, neurogenesis and synaptogenesis with a final goal to improve functional outcome of TBI patients.37
Steroids should not be routinely used and have actually been shown to increase mortality.38
Rehabilitation
There is now a substantial body of high quality research evidence for the effectiveness, and indeed the cost-effectiveness of rehabilitation. Access to appropriate and timely specialist assessment and rehabilitation has a positive impact on outcome. Studies suggest that patients with moderate to severe brain injury who receive more intensive rehabilitation showed earlier improvement and that earlier rehabilitation was better than delayed treatment.39,40
Strong evidence supports the provision of cognitive rehabilitation in a therapeutic ‘milieu’, that is, an environment in which patients receive predominantly group-based rehabilitation alongside a peer group of others who are facing similar challenges. Rehabilitation for brain injury is such an individualised and long-term process that research studies do not necessarily facilitate general conclusions.41
In addition to the above, enriched environment and voluntary physical exercise show promise in promoting functional outcome after TBI, and should be evaluated alone or in combination with other treatments as therapeutic approaches for TBI.42,43
Non-invasive brain stimulation (NBS)
Current evidence from animal and human studies reveals the potential benefit of non-invasive brain stimulation (NBS) in reducing the extent of injury and enhancing neuroplastic changes to facilitate learning and recovery of function post TBI. However, the evidence is mainly theoretical at this point. Given safety constraints, studies in TBI patients are necessary to address the role of NBS in this condition, as well as to further elucidate its therapeutic effects and define optimal stimulation parameters.44
Conclusion
There is a considerable amount of TBI-related research published every year. Systematic reviews consistently identify the need for well-constructed methodologically robust studies to elucidate appropriate treatment modalities, which can only be done if there is standardisation of the naming, definitions and classification of TBI subgroups.
Animal models of TBI are necessary to clarify injury mechanisms, to assess the safety and efficacy of new treatments prior to clinical trials and to better understand the injury mechanisms that drive injury progression. There is a need to explore optimal combinations of preventive and therapeutic measurements for TBI.
TBI is a complex and heterogeneous disease that requires recognition, monitoring and treatment in clinical practice according to the severity, course, age, gender and co-morbidities associated with injury. There are a number of significant positive developments forthcoming in Ireland with the work on head injury guidance led by the EMP, the imminent publication of the major trauma strategy, the major trauma audit in Ireland currently underway and the imminent national rehabilitation model of care from the rehabilitation medicine programme.
TBI is common and is often referred to as a silent epidemic. As healthcare professionals, both clinical and academic, and as decision makers for resource distribution, we have a duty to the patients we serve to optimise treatment pathways to get the best possible outcome for our patients.
References
Faul M, Xu L, Wald M et al. Traumatic brain injury in the United States: emergency department visits, hospitalisations and deaths 2002–2006. Atlanta, Georgia: Center for Disease Control and Prevention, National Center for Injury Prevention and Control. 2010
Phillips J. National report on traumatic brain injury in the Republic of Ireland. Traumatic Brain Injury Research Group, 2008
National Office of Clinical Audit Data: Major trauma audit 2014. Accessed January 1, 2016
Whitfield PC, Elfyn TO, Summers F et al. Editors. Head injury: A multidisciplinary approach. Cambridge University Press, 2009
Corrigan JD, Selassie AW, Oman JA. The epidemiology of traumatic brain injury. J Head Trauma Rehabil 2010; 25:72-80
Early management of patients with a head injury. A national clinical guideline. Scottish Intercollegiate Guidelines Network. 2009
Swann IJ, Walker A. Who cares for the patient with head injury now? Emerg Med J. 2001; 18(5):352-7
HIPE data provided by Hospital Purchasing Office, 2015. (unpublished)
Advanced trauma life support for doctors. American College of Surgeons committee on trauma. Student course manual (ATLS). Seventh ed. Chicago. The College. 2004
Roy CW, Pentland B, Miller JD. The causes and consequences of minor head injury in the elderly. Injury. 1986; 17(4):220-3
Thornhill S et al. Disability in young people and adults one year after head injury: Prospective cohort study. Brit Med J 2000; 320(7250):1631-5
Whitnall L, McMillan TM, Murray GD et al. Disability in young people and adults after head injury: 5-7 year follow up of a prospective cohort study. J Neurol, Neurosurg Psychiat. 2006; 77(5):640-5
Bennett B, Snoek J, Bond MR, Brooks N. Disability after severe head injury: observations on the use of the Glasgow outcome scale. J Neurol Neurosurg Psychiat 1981; 44: 285-93
Saatman KE, Duhaime AC, Bullock R et al. Classification of traumatic brain injury for targeted therapies. J Neurotrauma 2008; 25(7): 719-38
Werner C, Engelhard K. Pathophysiology of traumatic brain injury. BJA. 2007; 99(1): 4-9
Prins M, Greco T, Alexander D et al. The pathophysiology of traumatic brain injury at a glance. Dis Model Mech 2013; Nov 6(6): 1307-1315
Teasdale G, Jennet B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974; ii: 81-84
Shores EA et al. Preliminary validation of a clinical scale for measuring duration of post traumatic amnesia. Med J Aust 1986; 144: 569-72
Shivaji T et al. The epidemiology of hospital treated traumatic brain injury in Scotland. BMC Neurol 2014; 14:2 doi: 10.1186/1471-2377-14-2
National Rehabilitation Hospital, Dublin, Ireland unpublished data 2014-2015
Turner Stokes, L editor. Royal College of Physicians and British Society of Rehabilitation Medicine. Rehabilitation following acquired brain injury: national clinical guidelines. London: RCP, BSRM, 2003
Patel HC et al. Trends in head injury outcome from 1989 to 2003 and the effect of neurosurgical care: an observational study [published erratum in Lancet 2006; 367: 816]. Lancet. 2005; 366: 1538-44
Thillai M. Neurosurgical units working beyond safe capacity. BMJ 2000; 320-99
Maas AI, Stocchetti N, Bullock R. Moderate and severe traumatic brain injury in adults. Lancet Neurol 2008; 7: 728-35
Seeley HM, Maimaris C, Carroll G et al. Implementing the Galasko Report on the management of head injuries: the Eastern Region approach. Emerg Med J 2001; 18: 358-65
Cooper DJ, Myles PS, McDermott FT et al. Prehospital hypertonic saline resuscitation of patients with hypotension and severe traumatic brain injury: a randomized controlled trial. JAMA 2004; 291: 1350-7
The SAFE study investigators. Saline or albumin for fluid resuscitation in patients with traumatic brain injury. N Engl J Med 2007; 357: 874-84
Urbano LA, Oddo M. Therapeutic hypothermia for traumatic brain injury. Curr Neurol Neurosci Rep 2012; Oct 12(5):580-91
Wintermark M, Sanelli PC, Anzai Y et al. CT Imaging evidence and recommendations for traumatic brain injury: Advanced neuro and neurovascular imaging techniques. Am J Neuroradiol 2015; 36: E1-E11
Hutchinson PJ, Kolias AG, Timofeev I et al. Update on the RESCUEicp decompressive craniectomy trial. Crit Care 2011; 15(Suppl 1): P312
National Trauma Research Institute. Clinical research projects. Decompressive craniectomy (DECRA) study. Available from: www.ntri.com.au/research/clinical/projects/ (Accessed June 13, 2008)
Reis C et al. What’s New in Traumatic Brain Injury: Update on Tracking, Monitoring and Treatment. J Mol Sci 2015; 16: 11903-65
Loane D, Faden A. Neuroprotection for traumatic brain injury: translational challenges and emerging therapeutic strategies. Trends Pharmacol Sci 2010 December 1; 31(12):596-604
Maas AI, Roozenbeek B, Manley GT. Clinical trials in traumatic brain injury: past experience and current developments. Neurotherapeutics 2010; 7(1):115-126
Narayan RK, et al. Clinical trials in head injury. J Neurotrauma 2002; 19(5):503-57
Schouten JW. Neuroprotection in traumatic brain injury: a complex struggle against the biology of nature. Curr Opin Crit Care 2007; 13(2):134-42
Xiong Y, Mahmood A, Chopp M. Emerging treatments for traumatic brain injury. Expert Opin Emerg Drugs. 2009 Mar; 14(1):67-84
Alderson P, Roberts I. Corticosteroids for acute traumatic brain injury. Cochrane Database Syst Rev 2005; 15: CD000196
Turner-Stokes L. Evidence for the effectiveness of multi-disciplinary rehabilitation following acquired brain injury: a synthesis of two systematic approaches. J Rehabil Med 2008 Oct; 40(9):691-701. doi: 10.2340/16501977-0265
Turner-Stokes L, Pick A, Nair A et al. Multi-disciplinary rehabilitation for acquired brain injury in adults of working age. Cochrane Database of Systematic Reviews 2015; 12. Art No: CD004170. doi: 10.1002/14651858.CD004170.pub3
Bondi C, Klitsch K, Leary J et al. Environmental Enrichment as a Viable Neurorehabilitation Strategy for Experimental Traumatic Brain Injury. J Neurotrauma. 2014; 31(10): 873-88. doi: 10.1089/NEU.2014.3328
Van Praag H. Neurogenesis and exercise: past and future directions. Neuromolecular Med 2008; 10: 128-40
Wise EK, Hoffman JM, Powell JM et al. Benefits of exercise maintenance after traumatic brain injury. Arch Phys Med Rehabil 2012; 93:1319-23
Villamar M, Santos P, Fregni F et al. Noninvasive brain stimulation to modulate neuroplasticity in traumatic brain injury. Neuromodulation 2012 Jul; 15(4): 326-38. doi: 10.1111/j.1525-1403.2012.00474.x
 Incidence and causes of TBI in Ireland 2014. Data from the National Office of Clinical Audit, Major Trauma Audit 2016(click to enlarge)
Incidence and causes of TBI in Ireland 2014. Data from the National Office of Clinical Audit, Major Trauma Audit 2016(click to enlarge)