Often under-recognised or misdiagnosed, delirium is also known as ‘acute and fluctuating confusional state’. A serious condition, it can cause significant patient, family and healthcare distress. It is associated overall with poorer outcomes leading to increased morbidity, mortality and longer hospitalisations.1,2
Delirium can affect between 28-88% of patients with advanced cancer, with an incidence of 3-45% in specialist palliative care inpatients.1,3 The incidence increases as end of life approaches.4
Delirium can be challenging to recognise and subsequently manage particularly in the palliative care population at end of life. Distinguishing it from dementia, especially when they co-exist, can cause clinical management dilemmas for healthcare professionals. This review article will look at how to assess and manage delirium, principally focusing on the palliative care population.
Diagnosis
Delirium is diagnosed on the basis of the DSM IV diagnostic criteria:
• Inattention
• Disorganised thinking
• At least two of the following:
– reduced level of consciousness
– perceptual disturbance
– disturbance in sleep-wake cycle
– disorientation to time, place or person
– memory impairment.
• Short history and fluctuation.
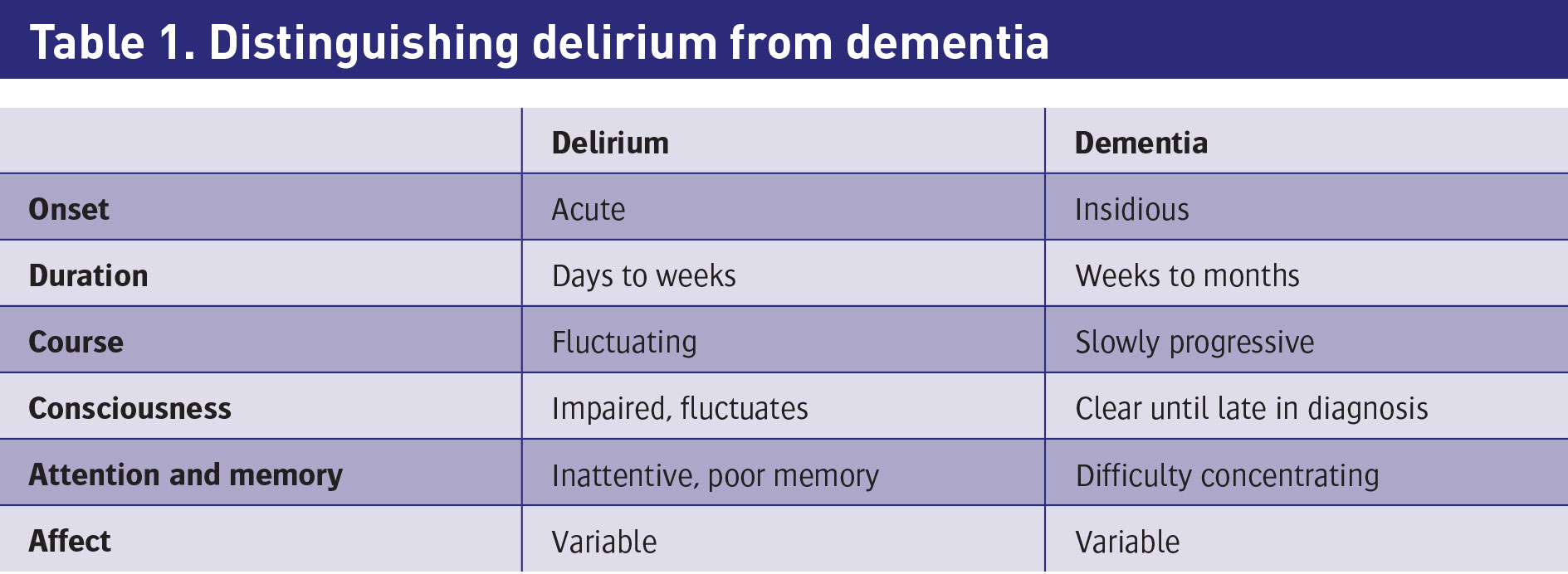
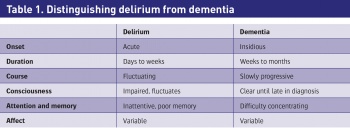
An important step in diagnosing delirium is to distinguish it from dementia. This can be a challenge clinically and certain features can be helpful (see Table 1 below).
There are three clinical subtypes of delirium based on psychomotor features:
Hyperactive
Hypoactive
Mixed.
Hyperactive delirium is associated with heightened arousal, leading to restless, agitated and aggressive behaviours.
Identifying hypoactive and mixed delirium can be more challenging.2 In the palliative care setting, hypoactive delirium is often more common and hence under-recognised.
Hypoactive delirium is denoted by withdrawn, quiet and somnolent features. It is often associated with dehydration and global encephalopathy, and patients are at increased risks of falls, longer hospitalisations and poorer outcomes.2,3
Hyperactive and mixed deliriums are more likely to be associated with medication as a consequence of side-effects, substance intoxication or withdrawal.
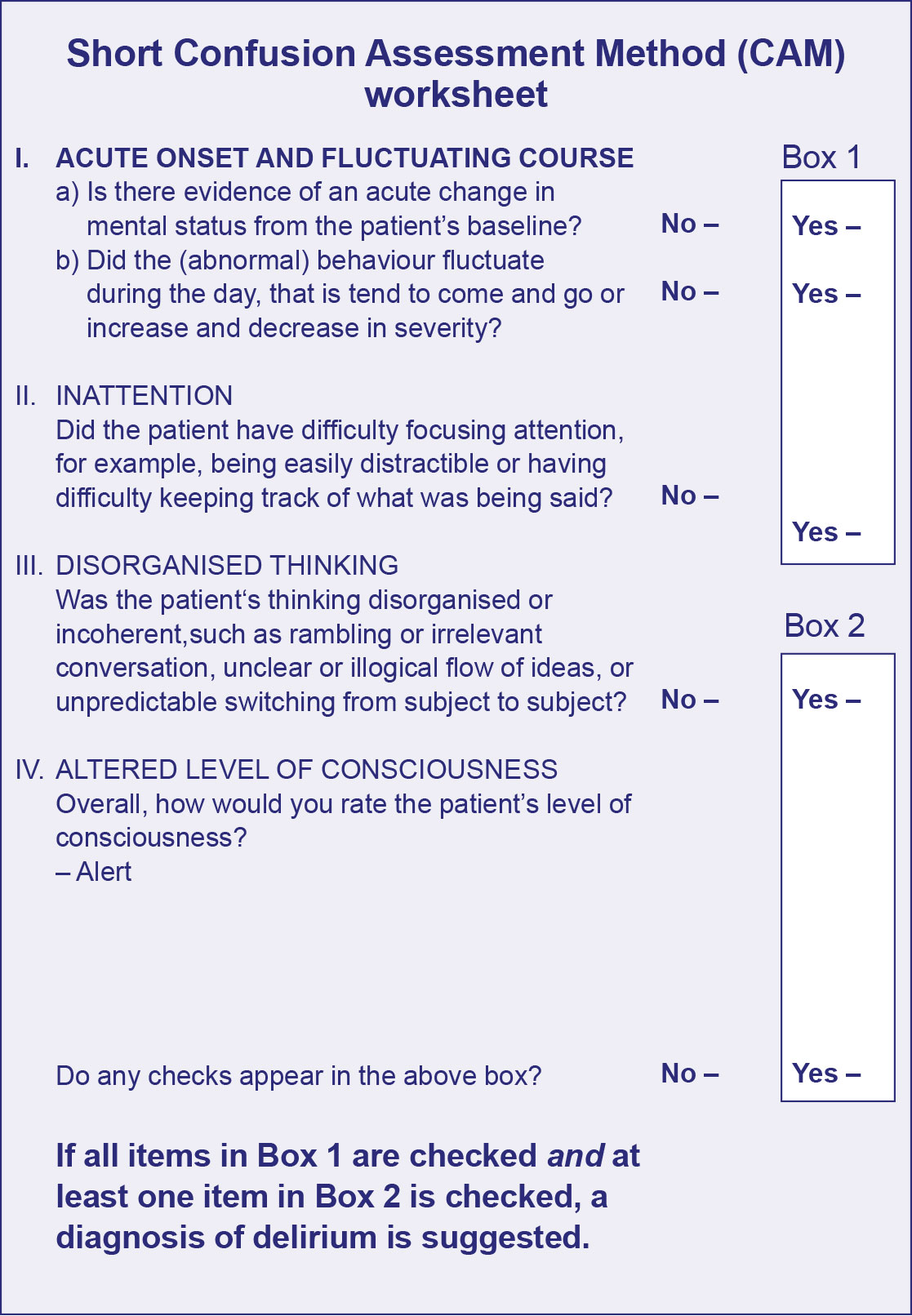
Screening tools have been established to aid in the diagnosis. The CAM (Confusion Assessment Method) is a diagnostic algorithm that is both sensitive (94%) and specific (89%) for the diagnosis of delirium especially when applied by specialists (see Figure 1).5
The algorithm is based on the cardinal features of delirium:
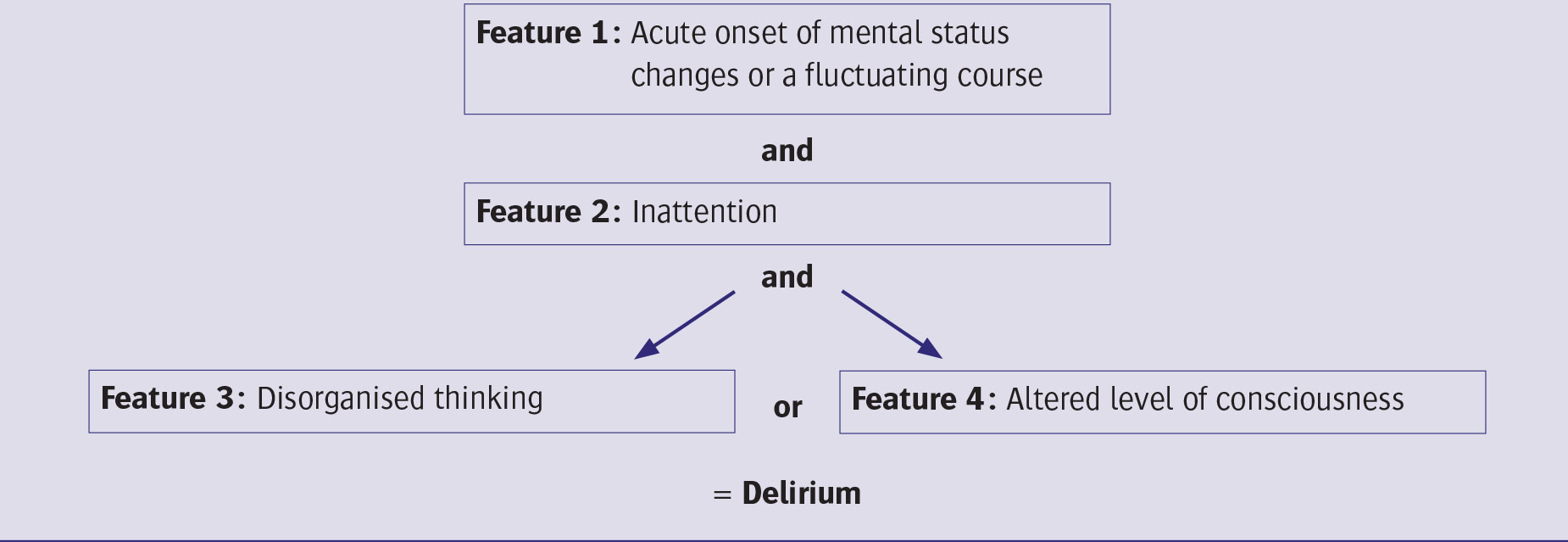
(1) Acute onset with fluctuating course and (2) Impaired ability to focus or sustain attention, ie. distractibility and either (3) Disorganised thinking or (4) Altered cognition (see Figure 2).
Recent research in developing screening tools shows that simple attention tests are useful in delirium screening. The MOTYB (ie. naming the months of the year backwards) is the best individual screening test for delirium especially in the elderly.6
Certain patient groups are more susceptible to developing a delirium. In particular elderly patients, those with cognitive impairment or reduced sensory input (visual impairment/deafness) and exposure to certain medications all increase the risk of delirium.7
(click to enlarge)
Figure 1. Confusion assessment (CAM) shortened version of worksheet (adapted from: Inouye SK et al. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann Intern Med 1990; 113: 941-8)(click to enlarge)
Figure 2. Cardinal features of delirium(click to enlarge)
Aetiology
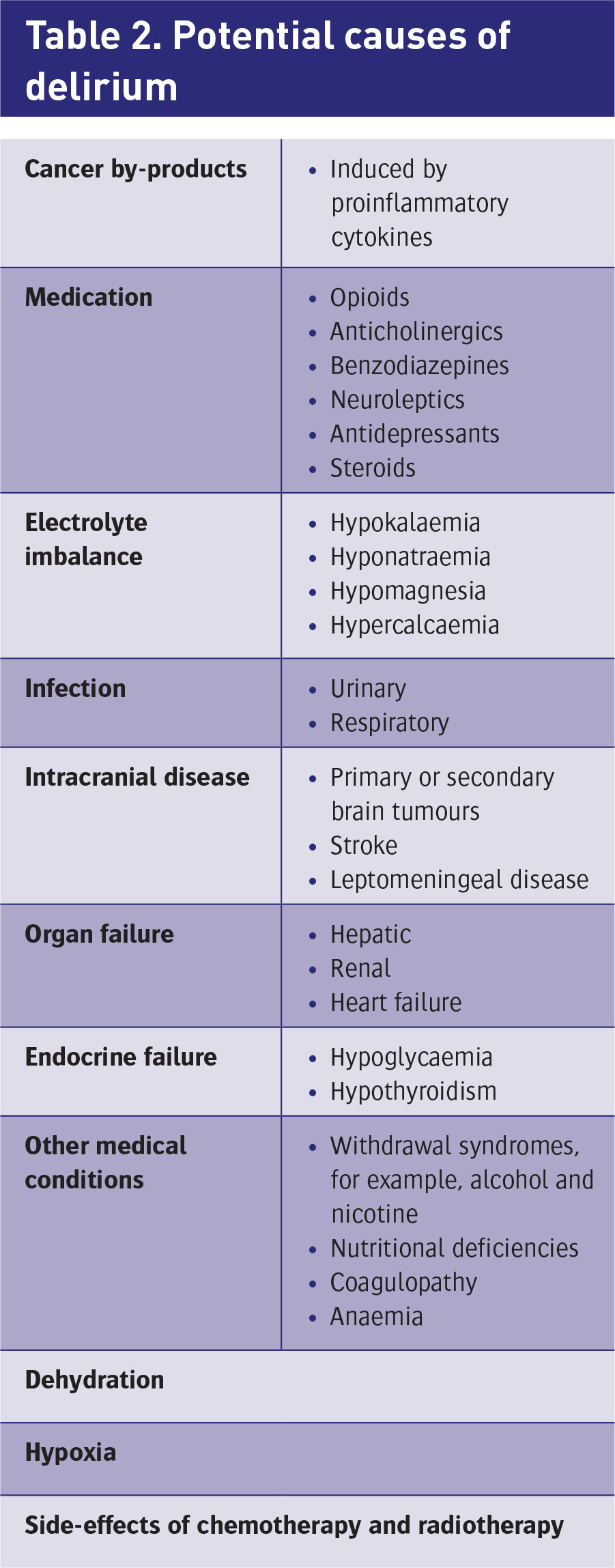
The aetiology of delirium is often multifactorial. A list of potential causes is outlined in Table 2.
The medications used in achieving symptom control in palliative care patients may also be causing or exacerbating the delirium. Anticholinergics in particular can cause a delirium and therefore caution is needed when introducing, combining or titrating these drugs (opioids, steroids, SSRIs, atropine, glycopyrolate and tricyclic antidepressants.8
(click to enlarge)
Management
A multifaceted approach required in the management of delirium. As with all symptoms in palliative care, management is tailored to the individual based on likely causes, potential reversibility, consideration of overall performance status, their recent illness trajectory and goals of treatment.9
The first step in managing a patient with delirium is to identify all potential reversible or contributory factors.2 A thorough history and examination followed by appropriate investigations will help in identifying potential reversible causes. If indicated the following should be arranged: baseline blood tests (to check full blood count, renal function, liver function, corrected calcium), urinanlysis( +/- MSU) and imaging if indicated, eg. chest x-ray, CT brain. Where appropriate any underlying cause should be corrected. Examples include sepsis, dehydration or electrolyte disturbances. Review and consider the role of drugs that may be aggravating or causing delirium, eg. anticholinergics, steroids. Recognition and management of opioid toxicity in particular and opioid induced neurotoxicity is essential in this population.
When reversibility is not possible, then delirium is a relatively reliable predictor of approaching death. It is important to recognise this situation, ie. an end-of-life delirium, so the transition of care can be made for the multidisciplinary team and the family and to enable a change in the focus of care to one of comfort measures. This needs to be discussed and communicated clearly with the family so they are aware of the significance.10
Management of delirium involves both non-pharmacological and pharmacological approaches. Better outcomes are achieved when drug and non-pharmacological interventions are combined.2,11 An interdisciplinary approach to optimising environmental factors so as to promote cognition and safety, and the provision of information to and involvement of family members is key.1
A delirious patient requires:
Simple communication
Reality orientation
Adequate lighting
One-to-one care.
Antipsychotics
Antipsychotics remain the cornerstone of pharmacological treatment of delirium (oral or parenteral). The 2010 NICE guidance on delirium supports the use of antipsychotics, either typical or atypical, in the pharmacological management of delirium, despite the lack of evidence. Ideally, the lowest dose antipsychotic is used for the shortest possible time.2
Guidance from the 2007 Cochrane review on the use of antipsychotics in delirium highlights some areas of note:12
Haloperidol, risperidone and olanzapine all have similar clinical effect in managing delirium. Low-dose haloperidol has no increased incidence of adverse effects when compared to low-dose atypical antipsychotics. Studies support the use of haloperidol at low dose for a short period in delirious patients. Haloperidol at < 3mg/day is effective in reducing severity and duration of delirium. With higher doses of haloperidol, there is increased risk of extrapyramidal side-effects (eg. Parkinsonism, tremor, rigidity, akathisia/restlessness and tardive dyskinesia) and cardiac toxicity (prolonged QT interval). In patients requiring higher doses, use of atypical antipsychotics may lead to fewer adverse effects
The newer atypical antipsychotics, eg. olanzapine and risperidone, have been associated with increased risk of stroke, especially in older people with dementia, when used at high doses
Quetiapine is being used more frequently in managing delirium in palliative care patients. Although it can cause extra-pyramidal side effects, its use in the management of delirium is favoured as studies to date showed no extra-pyramidal side effect in the delirious patients treated. However, these studies were limited by absence of a control group and further research in its use in delirium is needed.12
Levomepromazine is an antipsychotic drug that is widely used in palliative care. In addition to its antipsychotic properties, it also has anxiolytic, antiemetic and sedative effects.13 It is indicated as an adjunct in the relief of pain with accompanying anxiety or distress. As a result of its additional sedative effect, it is often used in the management of hyperactive or mixed delirium at end of life.
Benzodiazepines
Although benzodiazepines are not recommended as first-line in the management of delirium, their role in the management of delirium due to alcohol or acute benzodiazepine withdrawal is acknowledged.2,12 In the palliative care setting, they have the potential to precipitate a paradoxical agitation and therefore should be used with caution.14
In hyperactive delirium, benzodiazepines may be used as an adjunct to antipsychotics, either orally or subcutaneously, eg. midazolam and haloperidol.15
Methylphenidate
Methylphenidate is a psycho-stimulant originally used for the treatment of attention deficit disorder. It inhibits neuronal neurotransmitter transporters involved in the uptake of dopamine and norepinephrine at the level of the synapse. This leads to increased concentrations of dopamine and norepinephrine in the synapse resulting in increased alertness.15 The stimulant effect of methylphenidate has been used for the treatment of major depression, post-stroke depression, fatigue, delirium and sedation associated with opioid use.
Three studies examining the role of methylphenidate in advanced cancer patients with a hypoactive delirium showed improved end-of-life cognitive function and wakefulness.16 It is typically commenced at doses of 2.5mg twice daily or 5mg once daily and may be titrated to 15mg twice daily, once tolerated by blood pressure and heart rate.
Conclusion
Delirium is an increasingly common condition encountered in the palliative care patient population. It can be difficult to recognise and is associated with poorer outcomes for patients, particularly if it is not reversible. It can be distressing for the patient, family member and healthcare workers.
Earlier recognition can be aided by using diagnostic tools. Management requires both non-pharmacological and pharmacological approaches. Potential reversible causes should be first identified and corrected. Antipsychotic medications remain the mainstay of pharmacological treatment and greater understanding of their use and tolerability is emerging.
References
Hey J, Hosker C, Ward J, Kite S, Speechley H. Delirium in palliative care: Detection, documentation and management in three settings. Pall Supp Care 2013; 1-5
Young J, Murthy L. Diagnosis, prevention, and management of delirium: summary of NICE guidance. BMJ 2010; 341(jul28 2):c3704-c3704
Hosie A, Davidson PM, Agar M et al. Delirium: prevalence, incidence and implications for screening in specialist palliative care inpatient setting: a systematic review. Palliative Medicine. 2013;27(6):486-98
Morita T, Akechi T, Ikenaga M et al. Terminal Delirium: Recommendations from Bereaved Families’ Experiences. J Pain and Symptom Management 2007; 34(6):579-589
Ryan K, Leonard M, Guerin S et al. Validation of the confusion assessment method in the palliative care setting. Palliative Medicine 2008; 23(1):40-45
O’Regan NA. Attention! A good bedside test for delirium? J Neurol Neurosurg Psychiatry 2014;85:1122-1131.
Meagher D. Regular review: Delirium: optimising management. BMJ 2001; 322(7279):144-149
Zimmerman K, Salow M, Skarf L et al. Increasing anticholinergic burden and delirium in palliative care inpatients. Palliative Medicine 2014; 28(4):335-341
Bush S, Bruera E, Lawlor P et al. Clinical Practice Guidelines for Delirium Management: Potential Application in Palliative Care. J Pain and Symptom Management 2014; 48(2):249-258
Breitbart W, Alici Y. Agitation and delirium at the end of life: “We couldn’t manage him”. JAMA 2008 (Dec 24); 300(24): 2898-910, E1
Cole M. Systematic detection and multidisciplinary care of depression in older medical inpatients: a randomized trial. Canadian Medical Association Journal. 2006; 174(1):38-44
Lonergan E, Britton AM, Luxenberg J. Antipsychotics for delirium. The Cochrane Library. 2007
Dietz I, Schmitz A, Lampey I, Schulz C. Evidence for the use of levomepromazine for symptom control in the palliative care setting: a systematic review. BMC Palliat Care 2013; 12(1):2
Meagher D, Leonard M. The active management of delirium: improving detection and treatment. Advances in Psychiatric Treatment. 2008; 14(4):292-301
Prommer E. Methylphenidate: Established and Expanding Roles in Symptom Management. Am J Hospice and Palliative Medicine 2011; 29(6):483-490
Elie D, Gagnon P, Gagnon B, Giguère A. Using psychostimulants in end-of-life patients with hypoactive delirium and cognitive disorders: A literature review. Can J Psychiatry 2010 Jun; 2010; 55(6):386-93
 (click to enlarge)
(click to enlarge)