In Ireland it is estimated that 5% of adults have diabetes and the prevalence is rising steadily. It is estimated that 30-91% of diabetes patients experience at least one dermatological complication, which can vary from cosmetic concerns to life-threatening conditions. When discussing skin problems in diabetes patients it is useful to divide them into three categories:
• Specific cutaneous markers of diabetes which may indicate an increased risk of developing the condition. If diagnosed they should prompt us to screen for diabetes
• Non-specific skin problems that are more prevalent in diabetes patients, eg. skin infections
• Diabetic foot ulcers that are a consequence of diabetic neuropathy and vasculopathy.
Specific cutaneous markers of diabetes
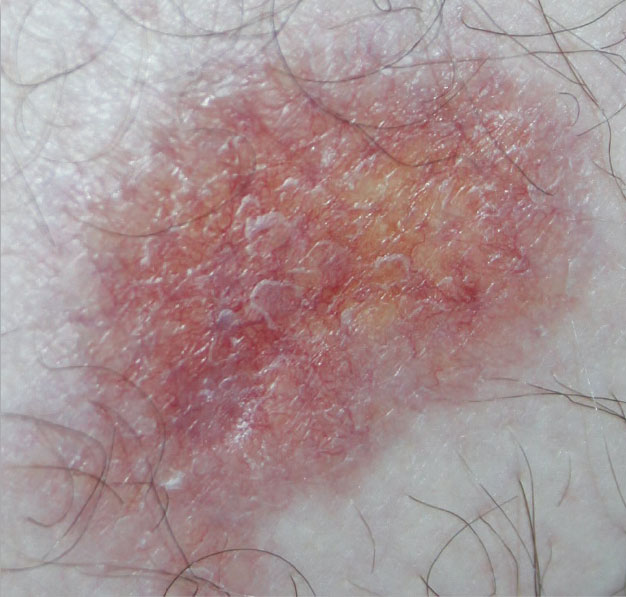
Necrobiosis lipoidica (NL) see Picture 1
Picture 1. Necrobiosis lipoidica. Note the central yellow colour (lipoidica) and the erythematous, advancing edge with prominent telangiectatic vessels(click to enlarge)
NL is a chronic, necrotising, granulomatous skin disease. Although only 0.3-1.6% of people with diabetes develop NL, 75% of patients with NL have or will eventually develop diabetes. NL is also associated with sarcoidosis, inflammatory bowel disease, autoimmune thyroiditis, rheumatoid arthritis and monoclonal gammopathy. It usually presents in the third to fourth decades of life, affecting females more than males in a 4:1 ratio.
Lesions may be solitary or multiple and while usually bilateral in the pretibial areas, they can present unilaterally. Lesions start as small, firm, erythematous papules that gradually grow into well demarcated, indurated, annular plaques. As the lesions develop, a characteristic yellow-brown atrophic centre that is studded with prominent ectatic blood vessels is visible. Over time the central areas become completely atrophic and the lesions are delimited by a narrow, reddish-brown or violaceous margin. Ulceration is common. NL may be asymptomatic, painful or pruritic. It is therefore quite a disfiguring and disabling problem. NL spontaneously resolves in 15% of patients after six to 12 years.
Treatments include the very potent topical corticosteroid ointment clobetasol, which should be applied to active borders of the lesions, aiming to reduce plaque inflammation and halt progression. Applying topical corticosteroid to the atrophic area serves no purpose and risks causing further atrophy.
Intralesional corticosteroids eg. triamcinolone, may be helpful. Again, only active disease at the margins should be injected. The topical calcineurin inhibitor, tacrolimus, may help. There is some evidence that applying compression can be helpful. Unfortunately NL tends to be refractory to treatment.
Granuloma annulare (GA) see Picture 2
Picture 2. Widespread granuloma annulare (GA). This pattern of GA is associated with diabetes. Localised GA is not related(click to enlarge)
GA is a necrobiotic, inflammatory disorder of unknown cause with a prevalence of 0.3% in diabetes patients. It presents as flesh-coloured to erythematous papules that gradually grow to and coalesce to form a discoid plaque. Plaques expand and centrally involute, giving annular configurations with raised borders. These borders are smooth, firm and not scaly. They should not therefore be confused with tinea infection, where the edges will tend to be scaly, less firm and rougher to touch.
GA most often presents with one or a few lesions, localised to the hands and feet. This form is not related to diabetes. Only the generalised form indicates an increased risk of developing diabetes.
Somewhere between 21% and 77% of patients with generalised GA have diabetes, with most of these having type 2 disease. It rarely predates the diabetes. Generalised GA is associated with dyslipidaemia. Therefore, all new cases should be tested for lipids and fasting glucose. Generalised GA runs a more chronic-relapsing course than the localised form, with spontaneous resolution rare.
Treatment tends to be ineffective. Options include clobetasone ointment, intralesional triamcinolone and cryotherapy.
Acanthosis nigricans (AN) see Picture 3
Picture 3. Acanthosis nigricans involving the axilla. Note the dark brown, velvety skin thickening(click to enlarge)
AN usually presents with dark brown, asymptomatic, velvety thickening of the skin. It develops most often in the flexures and on the neck. Papillomas may develop in the lesions of AN, giving a wart-like appearance. It is usually a benign condition, most frequently found in overweight patients with type 2 diabetes. It rarely presents as a paraneoplastic syndrome, most commonly associated with an adenocarcinoma of the stomach. Benign and malignant forms have a similar clinical and histologic presentation.
Many patients with obesity-related AN do not have diabetes and in these patients the condition resolves on weight reduction. Rapid onset of more widespread distribution of AN, with itch and soreness, especially in the non-obese, should prompt consideration of malignant AN. In diabetes patients AN is best managed by weight reduction.
Diabetic bullae (DB)
DB presents as inflammatory, tense, painless, bullae on normal-appearing skin. It is rare, with an incidence of 0.5% in diabetes, usually occurring in long-standing illness. It is often associated with neuropathy, nephropathy and retinopathy. Tense, non-inflamed, asymptomatic bullae, varying in size from a few millimetres to several centimetres in diameter, develop abruptly, mainly on the lower extremity.
They become more flaccid as they enlarge and resolve spontaneously in six weeks, without scarring. They tend to recur. The cause of DB is unknown. They are managed by releasing the fluid, applying an appropriate dressing and compression.
Generalised pruritus
There is an increased incidence of generalised itch in diabetes patients. The cause is not known but it may be due to poor microcirculation and increased dryness of the skin. Moisturisers may help. Amitriptyline, starting at a dose of 10mg at night and titrating upwards, depending on response and tolerability, is a good option for more severe itch.
Eruptive xanthomas (EX)
EX presents with the sudden eruption of groups of multiple red-yellow papules, 1-4mm in diameter and surrounded by erythematous halo. They are most commonly found on the extensor surfaces of the extremities and the buttocks. They are virtually pathognomonic of hypertriglyceridaemia. They tend to resolve with control of carbohydrate and lipid metabolism.
Diabetic dermopathy (DD)
DD presents as multiple, asymptomatic, round, dull red to pink papules or plaques on the pretibial areas, the forearms, the thighs and over the lateral malleoli of the ankles. After one to two weeks of their appearance they evolve into well circumscribed, atrophic, brown macules, often with fine scale.
Up to 40-50% of diabetes patients have DD. It is more common in males, those over 50 years of age, and those with long-standing or poorly controlled diabetes. Patients having DD have an increased incidence of retinopathy, neuropathy and nephropathy.
Non-diabetes patients with greater than four such lesions are thought to be at increased risk of developing diabetes.
Skin infections
There is an increased risk of skin infection in diabetes. Bacterial or fungal infection may be the presenting feature of the condition. Any diagnosis of folliculitis, boils, carbuncles (see Picture 4) or candida should prompt testing for diabetes. Patients with poorly controlled type 2 diabetes are more predisposed as the infections are related to hyperglycaemia. Particular care needs to be taken with candida and tinea infection between the toes (see Picture 5). Skin breaks in these areas may allow entry of bacteria to deeper tissues of the foot. Spreading infection may threaten limb survival.
Picture 4. Carbuncle on the lower chest wall of a patient with diabetes(click to enlarge)
Picture 5. Tinea pedis fungal infection with a very itchy vesicular reaction. Treatment is indicated in this diabetic patient as there is a risk of bacteria penetrating irritated skin to cause foot-threatening deep infection(click to enlarge)
Diabetes patients with dermatophyte foot infection should be treated with oral terbinafine. Topical antifungal treatment will not eradicate dermatophyte infection from the hyperkeratotic skin of the feet.
Diabetic foot ulcers
Diabetes is a clinically significant risk factor for foot ulceration. Foot ulcers are the most costly and preventable complication of diabetes, and while the prevalence of diabetes in the general population is 5%, 46% of patients admitted to hospital with foot ulcers have diabetes, and 50% of patients having lower extremity amputations have diabetes. Therefore, diabetic foot ulceration has major implications for people.
Once ulceration has developed it is very difficult to heal. ‘Diabetic ulceration’ is really a misnomer as diabetes is only one of multiple causes; 50% have neuropathy, 20% have ischaemia and 30% have both (see Picture 6).
Therefore the emphasis in primary care monitoring of diabetes is on the regular checking of all patients for risk factors of ulceration, especially for signs of neuropathy or ischaemia. Early intervention and involvement of vascular surgery and podiatry is essential if any increased risk is identified. It is estimated that 50% of amputations and foot ulcers can be prevented by effective risk identification and patient education.
Vasculopathy
Enquire about any history of intermittent claudication or rest pain. Remember that patients with neuropathy may under appreciate ischaemic pain. Dorsalis pedis or posterior tibial pulses should be palpated but remember that people with diabetes have an increased incidence of arterial wall sclerosis, in which case a palpable pulse does not exclude poor perfusion.
The ankle brachial pressure index (ABPI), measured with a hand-held Doppler, gives a more accurate measure of ischaemia but can be falsely elevated in diabetes patients. Look for signs of ischaemia such as pallor, dependent redness, cool limb, lack of hair and thin, atrophic shiny skin.
Blood glucose control should be optimised as poor control accelerates arterial disease. If ischaemia is detected, refer the patient to vascular surgery for fuller testing and consideration of revascularisation.
Neuropathy (see Picture 6)
Picture 6. A hammer toe deformity has caused excessive wear and pressure on the plantar surface of the big toe, leading to ulceration, cellulitis and osteomyelitis. This diabetic foot ulcer was on an ischaemic, neuropathic limb, did not respond to treatment and subsequently required amputation(click to enlarge)
Neuropathy may be sensory, autonomic, or motor. All three types may play a part in the development of foot ulceration:
• Autonomic neuropathy leads to the development of dry skin which is more prone to breakdown
• Motor neuropathy may cause muscle atrophy and lack of muscle co-ordination leading to ambulation difficulties, toe deformity, and loss of reflexes. The foot may develop ‘hammer toe’ or a ‘claw toe’ deformity which cause abnormal distribution of foot pressure. Over time this pressure leads to the development of callus over pressure points
• Sensory neuropathy leads to loss of protective sensation. This means that the patient does not detect the abnormal pressure outlined above. Repetitive trauma goes undetected, leading to tissue injury, inflammation and eventually tissue necrosis and ulceration. Areas at risk are those that experience pressure while walking or from poorly fitting footwear. During ambulation, direct sagittal force is experienced on two areas of the plantar aspect of the foot – the heel during heel strike and the forefoot during push-off. When examining the foot, particular attention needs to be directed at these areas. Repeated trauma to the foot tends to progress from callus formation, to subcutaneous bleeding, to ulceration, to deeper infection and osteomyelitis.
Testing for neuropathy
A 128-Hz tuning fork is used for vibration testing and a 10g (5.07) Semmes-Weinstein monofilament for sensation. The patient’s eyes should be closed. The monofilament is pressed down on intact skin (non-callus). The monofilament should be allowed to buckle.
Ten sites should be tested, and absent sensation in three sites indicates a positive result. This positive result flags the patient’s increased risk of further diabetes-related foot complications.
Wound dressings
Should ulceration develop, an appropriate dressing regimen needs to be started. Essentially, a dressing should provide a physical, protective barrier that will maintain a moist wound environment over the ulcer surface. This provides the optimum environment to promote wound healing. There is no good evidence that any one dressing is better than another.
Categories used include hydrogels, acrylic film, hydrocolloids, calcium alginates, hydrofibers, and foams. A high exudate wound needs an absorptive dressing (foams, calcium alginates, hydrofiber). A dry wound needs a dressing that will donate moisture (hydrogels) or preserve or bind water (acrylics, hydrocolloids, films).
A diabetic foot ulcer is a chronic wound. Chronic wounds tend to be covered in slough, crust or eschar, all of which impair wound healing. Removing these layers, ie. debriding, converts the chronic wound to an acute wound. Acute wounds heal much better than chronic ones. Debridement is therefore an essential component of managing diabetic foot ulcers.
Hydrogels applied under a secondary dressing may achieve chemical debridement. Surgical debridement, using a scalpel, is best. EMLA topical anaesthetic may be applied one hour before the procedure.
The presence of neuropathy means that the patient may tolerate the procedure without anaesthetic. All tissue down to red, bleeding areas needs to be debrided.
Several studies have concluded that plantar pressure redistribution is the most important component in the management of neuropathic ulcers. Therefore, all patients should be referred to podiatry for plantar pressure redistribution.
Podiatrists may consider shoes with insoles that redistribute high-pressure areas, a total contact cast or a removable cast walker.
Infection in the diabetic foot
Fifty per cent of patients with a diabetic foot ulcer develop skin or soft tissue infection. Infection can vary from superficial cellulitis to deeper infection of the soft tissue and bone. Signs that might suggest infection include erythema, tenderness, discharge, localised increase in temperature or deranged diabetic control. White cell count and inflammatory markers may be normal in patients with an infected foot.
Infection is diagnosed clinically. If judged necessary, a swab should only be taken after debriding from healthy looking tissue. Active infection is treated for at least two weeks if it is mild and superficial, for two to four weeks if moderately severe and for six to 12 weeks if bone is involved.
Co-amoxiclav 375mg eight-hourly is usually effective. If the patient is allergic to penicillin, clindamycin 300mg six-hourly is suitable. Patients who are systemically unwell should be admitted. If prompt improvement does not occur, consider urgent referral for hospital admission.
Monitoring the diabetes patient’s foot
The onset of diabetic foot ulceration is insidious and many patients are unaware of symptoms or signs of progression. Screening to identify the high-risk foot is an essential component of diabetes care. Patients should be graded for risk and all patients need education on how best to look after their feet.
The greater burden of this work will fall on primary care and especially on practice nurses. Ready access to chiropodists, podiatrists, dietitians, public health nurses, and vascular surgeons is essential to support this service. If adequate funding is not provided, the burden of disease will mount for patients as will expense for the health service.
 Picture 1. Necrobiosis lipoidica. Note the central yellow colour (lipoidica) and the erythematous, advancing edge with prominent telangiectatic vessels(click to enlarge)
Picture 1. Necrobiosis lipoidica. Note the central yellow colour (lipoidica) and the erythematous, advancing edge with prominent telangiectatic vessels(click to enlarge)