The National Centre for Inherited Metabolic Disorders is based at the Children’s University Hospital, Temple Street, Dublin and treats both children and adults with inherited metabolic disorders.
Classical galactosaemia, a disorder of carbohydrate metabolism, is an inherited metabolic disorder that occurs due to deficiency of the enzyme, galactose-1-phosphate uridyl transferase (GALT). This deficiency results in a failure of the body to be able to breakdown galactose, one of the two sugars that make up lactose in breast and cow’s milk.
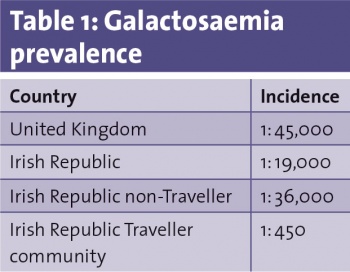
Prevalence and diagnosis
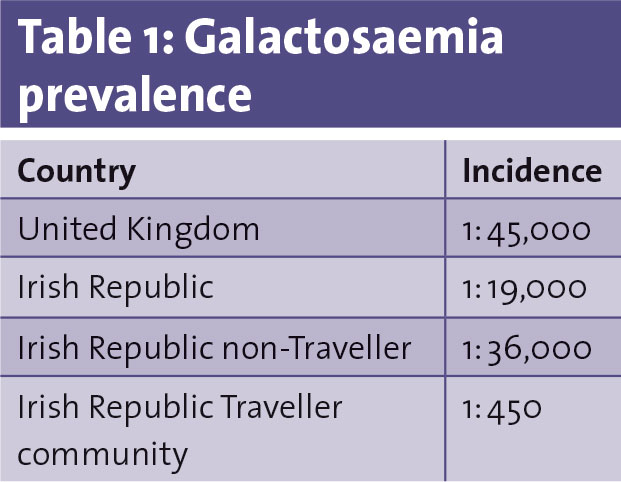
Approximately one in every 19,000 infants born in Ireland has galactosaemia. It is an inherited autosomal recessive disorder ie. both parents are carriers of the mutation, so it is inherited in the same way as PKU. There is an equal prevalence in males and females. There is a higher incidence of galactosaemia in the Irish Traveller community (1:450) vs the non-Traveller community (1:36,000.)
Screening for galactosaemia in Ireland was added on to the national newborn screening programme in 1972. It is one of four metabolic conditions screened for. Commonly referred to as the ‘heel prick test’, blood is taken from the baby’s heel between 72 and 120 hours of life.
As outlined above, galactosaemia is relatively common in infants born to Traveller parents, therefore, a special screening test is offered to babies on the first day of life. The Traveller community is aware that this early screening exists. Travellers are advised not to breastfeed at birth and are offered a galactose-free feed (soya-based) until the result of the test is available. Elemental formula is suitable but not usually indicated. This treatment helps to protect the infant from potentially becoming acutely unwell in the neonatal period. Mothers wishing to breastfeed can do so still once it has been confirmed the baby does not have galatosaemia. They need to express their milk until the result of the test is available. If the result is positive for galactosaemia breastfeeding is unfortunately contraindicated as it contains galactose.
(click to enlarge)
Galactose metabolism
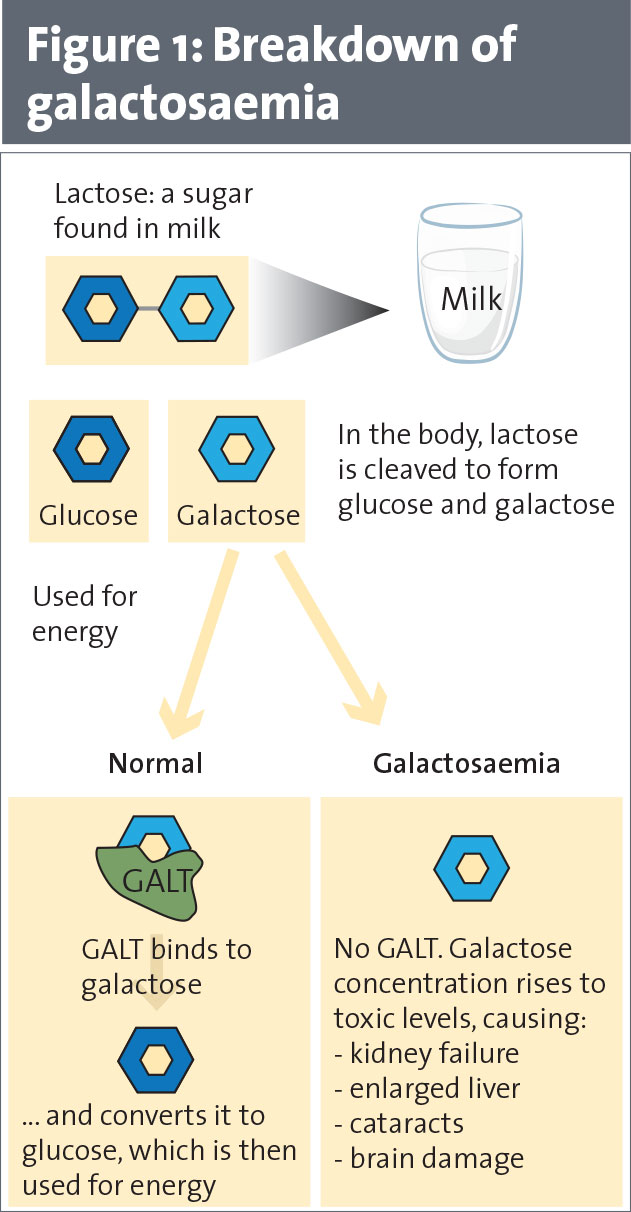
Galactose in the diet mainly comes from lactose, the main sugar in milk. In normal lactose metabolism, lactase breaks down lactose in the human gut to glucose and galactose. Galactose is then broken down to glucose to produce energy using the GALT enzyme. In galactosaemia the breakdown is inhibited (see Figure 1). Galactose then builds up to toxic levels in the body causing issues in the brain, liver, kidneys and ovaries.
(click to enlarge)
If not detected and treated during infancy, the disorder may cause damage to the liver and may occasionally be life-threatening. Early detection and treatment with a galactose-free diet will prevent the early clinical symptoms of the disorder; some of the longer-term complications may still occur in older children and adults despite treatment. Complications which may occur include:
• Neurological dysfunction
• Cognitive impairment
• Verbal dyspraxia
• Infertility in females.
Dietary management
Treatment in the newborn consists of the exclusion of all lactose and galactose from the diet. This is relatively straight forward as lactose-free formulae are available. The baby remains on this exclusively until weaning is commenced at the recommended six months of age as per the rest of the population. Education then centres around label reading, weaning and on avoiding sources of lactose and galactose.
Lactose is found in four main types of food:
• Cow’s milk
• Products made from cow’s milk
• Manufactured foods which contain cow’s milk
• Any mammalian milk including breast milk, goat’s milk or sheep’s milk.
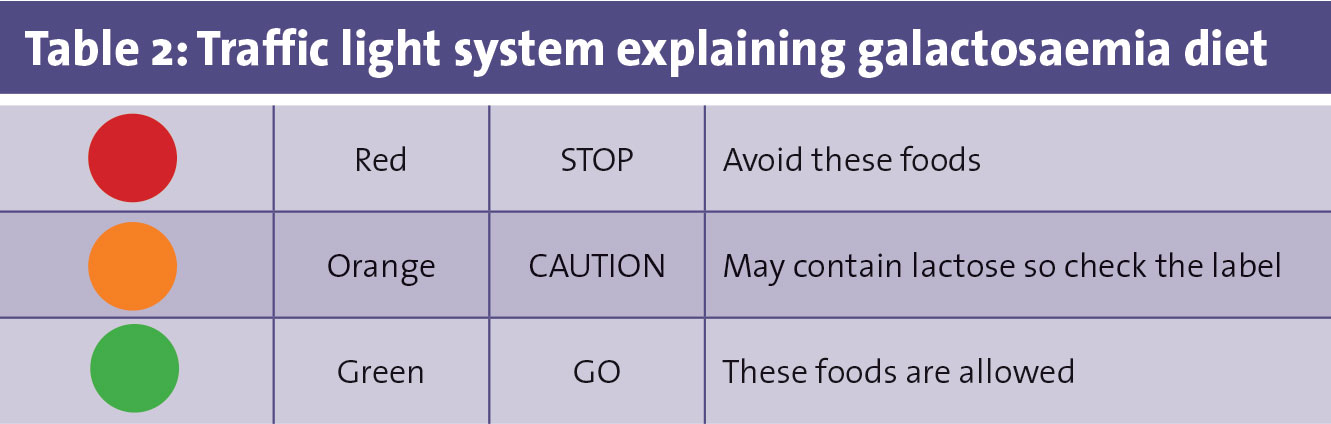
The galactosaemia diet can be split into three main groups. A traffic light system is often used to help explain the diet in more detail (see Table 2). Visit www.metabolic.ie to view more details on the diet.
(click to enlarge)
Lactose-free products
Of particular note has been the evolution of increasingly popular lactose-free products in supermarkets eg. milk and cheese. These foods are not suitable for galactosaemia as they contain galactose.
Lactose in medications
Lactose can be present eg. as a filler. For most, the amount of lactose is unlikely to be significant. Patients are always advised to check with their pharmacist for all over-the-counter medicines and to remind their GP that their prescription should be lactose free.
Other sources of galactose
The following foods are not excluded in Ireland as the amount of galactose in them is minimal:
• Legumes and beans: Galactosides and oligosaccharides – raffinose and stachyose (soya, cocoa, nuts)
• Fruit and vegetables: Free and bound galactose – part of galactolipids, glycoproteins, melibrose
• Offal and eggs: Contain nucleoproteins. Galactose storage organs in animals; eggs.
Bone health
Calcium is necessary to build strong and healthy bones. Milk and milk products usually provide a main source of calcium in the diet. In galactosaemia, milk needs to be replaced with infant soya formula for babies. Soya products fortified with calcium can meet the requirements for older children and adults.
Sources of calcium include:
• Fortified soya products
• Green leafy vegetables
• Tinned salmon and nuts
• Suitable cheeses (discussed below)
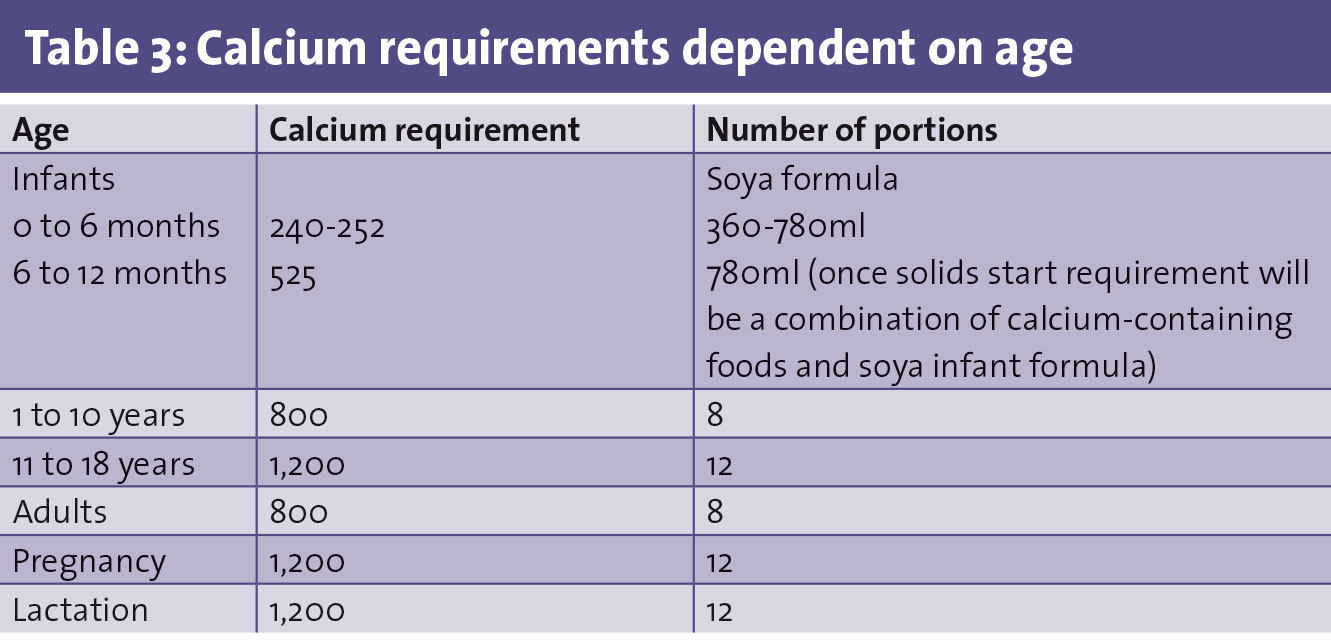
Table 3 outlines calcium requirements for age. Parents/children are encouraged to calculate intake to ensure dietary adequacy. Supplements of calcium and vitamin D are not routinely prescribed. Parents are encouraged to look for both calcium and vitamin D-containing soya products. If nutritional intake is not adequate or deficiency found then supplements will be prescribed. Compliance in particular with calcium supplements can be poor.
Some ordinary cheese can be taken in the diet and is a good source of calcium. This is due to the fact that during the cheese manufacturing process lactose and galactose is lost through two different processes:
• The bacteria added in cheese production will use up the lactose and galactose
• As the cheese ages or matures it dries out and as it dries out it loses lactose and galactose in the whey liquid.
As a result the following cheeses are recommended:
• Emmental (Swiss cheese)
• Gruyere (French cheese)
• Jarlsberg (Norwegian cheese)
• French Comte
• Italian Parmesan (American Parmesan is not suitable)
• Grana Padano (type of Parmesan).
Management of classical galatosaemia
Despite compliance and good metabolic control, long-term complications still occur and are increasingly recognised. There are some unanswered questions, and clinical studies have been performed in Ireland and elsewhere, or are ongoing, to look at, for example, partial diet relaxation as a potential treatment option for certain subgroups of patients (eg. adult patients).
The National Centre for Inherited Metabolic Disorders has close collaboration within the international Galactosemia Network (GalNet). Along these lines, we have also been involved in preparing the ‘international clinical guideline for the management of classical galactosaemia: diagnosis, treatment, and follow-up’ which were published recently in the Journal of Inherited Metabolic Disease.1 Unanswered questions include:
• Exclusion of other foods containing a possible source of galactose
• Significance of endogenous production
• Is the diet too restrictive in the long-term and a cause of some of the complications in susceptible individuals?
However, it is important to emphasise that elimination of dietary galactose/lactose is the only available treatment for patients with classical galactosaemia at present and that it is life-saving, especially in neonates.
(click to enlarge)
Reference
International clinical guidelines for the management of classical galactosaemia; diagnosis, treatment and follow-up. Welling et al. Journal of Inherited Metabolic Disorders 17th November 2016
 (click to enlarge)
(click to enlarge)