Non-steroid anti-inflammatory drugs (NSAIDs) are commonly used in elderly patients to treat pain of a wide range of aetiologies, from muscular pain to arthritic pain to headaches. They are used in the management of both acute and chronic pain. While they are very effective drugs both clinically and economically, they have a number of side-effects, one of the most notable of which is their effect on the mucosa of the upper gastro-intestinal (GI) tract, causing ulceration and bleeding.
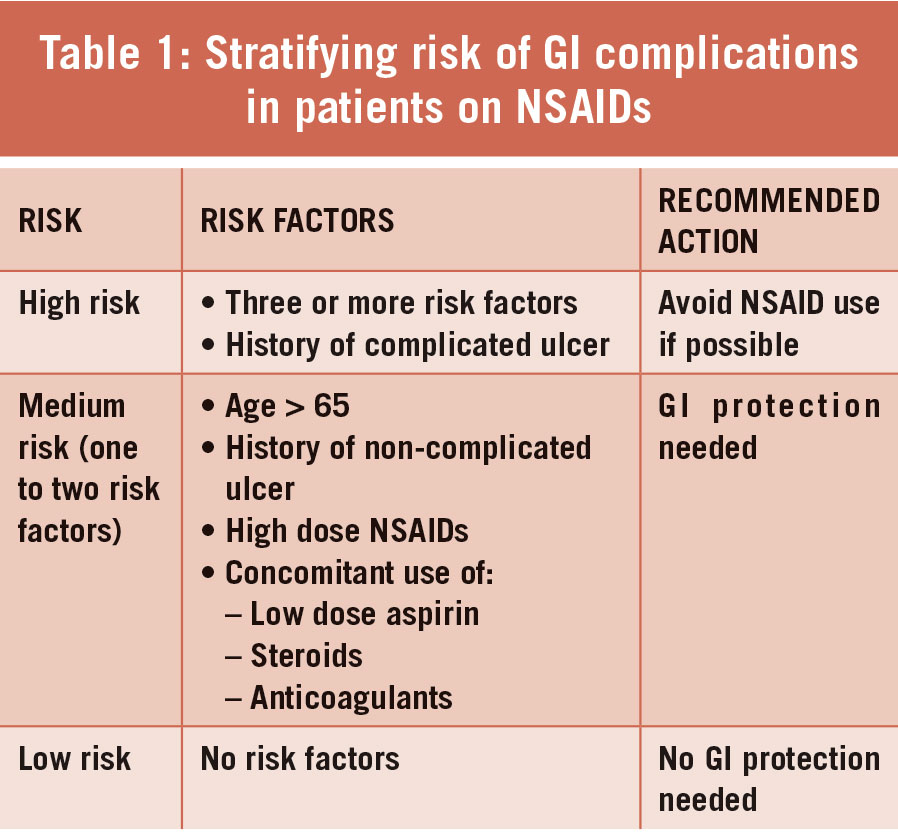
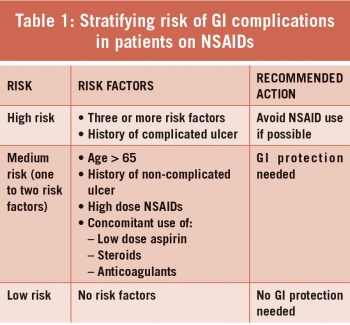
While the mechanism behind this has not been fully elucidated, it is thought to be primarily due to the effect of these drugs on the production of prostaglandins, which are thought to play a role in mucosal protection from acids in the GI tract. Other mechanisms are also thought to play a role, such as topical irritation and disruption to the gastric mucosal blood supply.1 As many as 25% of long-term NSAID users will develop GI ulcers, and the rate of perforation or bleeding can be as high as 4%.2 These figures vary from patient to patient, depending on other risk factors, as outlined in Table 1.3
(click to enlarge)
Interestingly, the concomitant use of low-dose aspirin with another NSAID increases the risk of GI complications. This is important to note, as many patients may be self-medicating with aspirin, and so physicians must be vigilant when prescribing other NSAIDs, particularly in elderly patients. A large scale study based on autopsies of patients who had been using NSAIDs found that the patients at highest risk were those who had been using NSAIDs for less than three months.4 This is not to say, however, that the risk of ulcers is non-existent in those using the drugs for longer periods of time.
One of the most commonly used methods for avoiding GI complications with NSAID use is to co-prescribe a proton pump inhibitor (PPI). Other techniques include using misoprostol, a prostaglandin analogue, H2 receptor antagonists such as ranitidine or famotidine, and COX-2 selective NSAIDs such as celecoxib.
NSAIDs inhibit the enzyme cyclooxygenase (COX) which is involved in prostaglandin production. It is the COX-1 isoenzyme that is most active in the gastric mucosa, where it facilitates production of prostaglandins. Of note, the reduced rate of GI complications with COX-2 selective NSAIDs versus traditional NSAIDs is negated if the patient is also taking low-dose aspirin.2
Current guidelines suggest that in patients who are low risk for GI complications, NSAIDs can be safely used without any form of gastric mucosal protection, but should be used at the lowest effective dose for the shortest effective period.
In patients at medium risk of GI complications, the concomitant use of a PPI or misoprostol is recommended. For those at high risk of GI complications, NSAID use should be avoided. If absolutely necessary, a COX-2 selective inhibitor should be used alongside a PPI or misoprostol.
While there are no current guidelines as to the need for gastric protection in patients taking low dose aspirin without other NSAIDs, a recently published prospective population-based study of more than 3,000 patients 5 suggests that a PPI should be co-prescribed in patients over the age of 75. For the purposes of this audit, this guideline was used.
Results
For the purposes of this audit we looked at one particular risk factor: age, specifically patients over the age of 65. We searched the practice software, Socrates, for all prescriptions issued to patients over the age of 65 over the past six months for aspirin, ibuprofen, diclofenac, naproxen and meloxicam. There were 302 prescriptions for NSAIDs in total, prescribed to a total of 162 different patients. Of the 302 prescriptions, 14 were non-oral routes of administration, to 11 different patients, and so these were excluded.
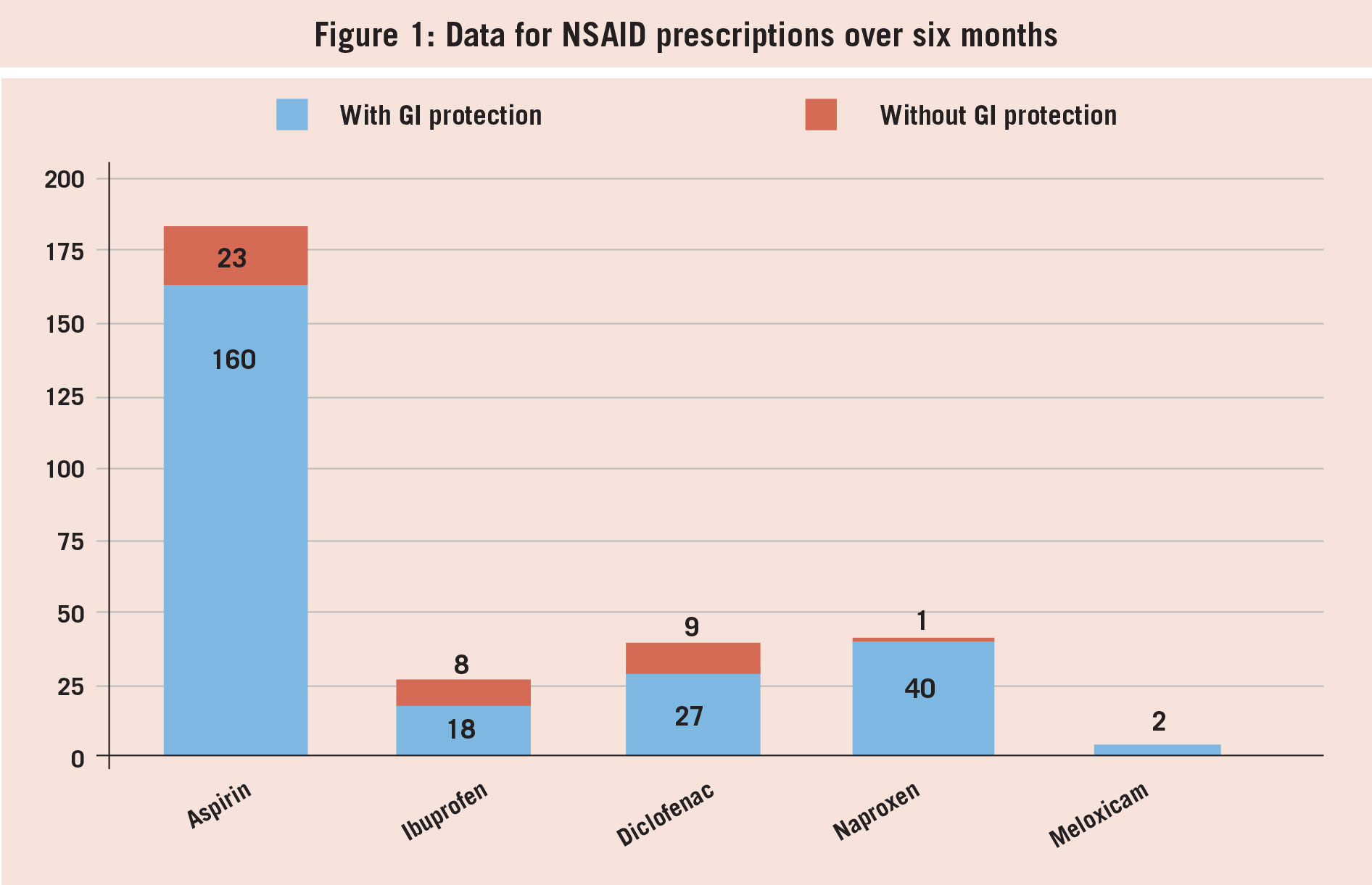
Of the oral NSAID prescriptions, 64% were for aspirin (n = 183), 9% were for ibuprofen (n = 26), 12.5% were for diclofenac (n = 36), 14% were for naproxen (n = 41) and <1% were for meloxicam (n = 2). Of the aspirin prescriptions, 12.5% were given to patients over 75 without gastric protection (n = 23). Of the ibuprofen prescriptions, 11% were given without gastric protection (n = 8). This figure was 25% for diclofenac (n = 9) and 2% for naproxen (n = 1). Both patients who were prescribed meloxicam were co-prescribed a PPI.
It is worth noting that the vast majority of naproxen prescriptions were in the form of a combination drug which includes a PPI; this in part explains why the number of naproxen prescriptions without GI protection was so low (see Figure 1). In all, these figures give a total of 41 times an NSAID was prescribed without gastric protection, against current guidelines. Of these, 20 different patients were on repeat prescriptions for NSAIDs without gastric protection.
(click to enlarge)
Discussion
In light of our findings, a practice meeting was held to discuss our prescribing of gastric protection alongside NSAIDs in patients over the age of 65. The 20 patients on repeat prescriptions for NSAIDs without gastric protection were contacted, and a PPI was added to their regular medications where appropriate.
While most prescriptions for NSAIDs in patients over the age of 65 were appropriately co-prescribed with gastric protection, the results of this audit show that NSAIDs are still commonly prescribed without this protection. While combination drugs are a good way to ensure that all patients are receiving gastric protection, they are associated with higher costs compared to independently prescribing GI protection. As a result of this audit, all patients over the age of 65 currently on repeat NSAIDs, or over the age of 75 and on low dose aspirin, have had a PPI added to their regular medications.
A re-audit is planned to examine the rates of adherence to guidelines on GI protection following the practice meeting, and to complete the audit cycle.
References
Wallace JL. How do NSAIDs cause ulcer disease? Baillieres Best Practice and Research. Clinical Gastroenterology 2000
Silverstein FE. Gastrointestinal toxicity with celecoxib vs. nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. Journal of the American Medical Association 2000
Lanza FL, Chan FK, Quigley EM. Practice Parameters Committee of the American College of Gastroenterology. Guidelines for prevention of NSAID-related ulcer complications. American Journal of Gastroenterology 2009 Mar;104(3):728-38
Allison MC, Howatson AG, Torrance CJ, Lee FD, Russell RI. Gastrointestinal damage associated with the use of nonsteroidal anti-inflammatory drugs. New England Journal of Medicine 1992
Li L, Geraghty OC, Mehta Z, Rothwell PM, Oxford Vascular Study. Age-specific risks, severity, time course, and outcome of bleeding on long-term antiplatelet treatment after vascular events: a population-based cohort study. Lancet 2017
 (click to enlarge)
(click to enlarge)