The majority of patients presenting in general practice with symptoms of headache are suffering from a benign disorder that can be managed and helped with careful monitoring and headache diaries
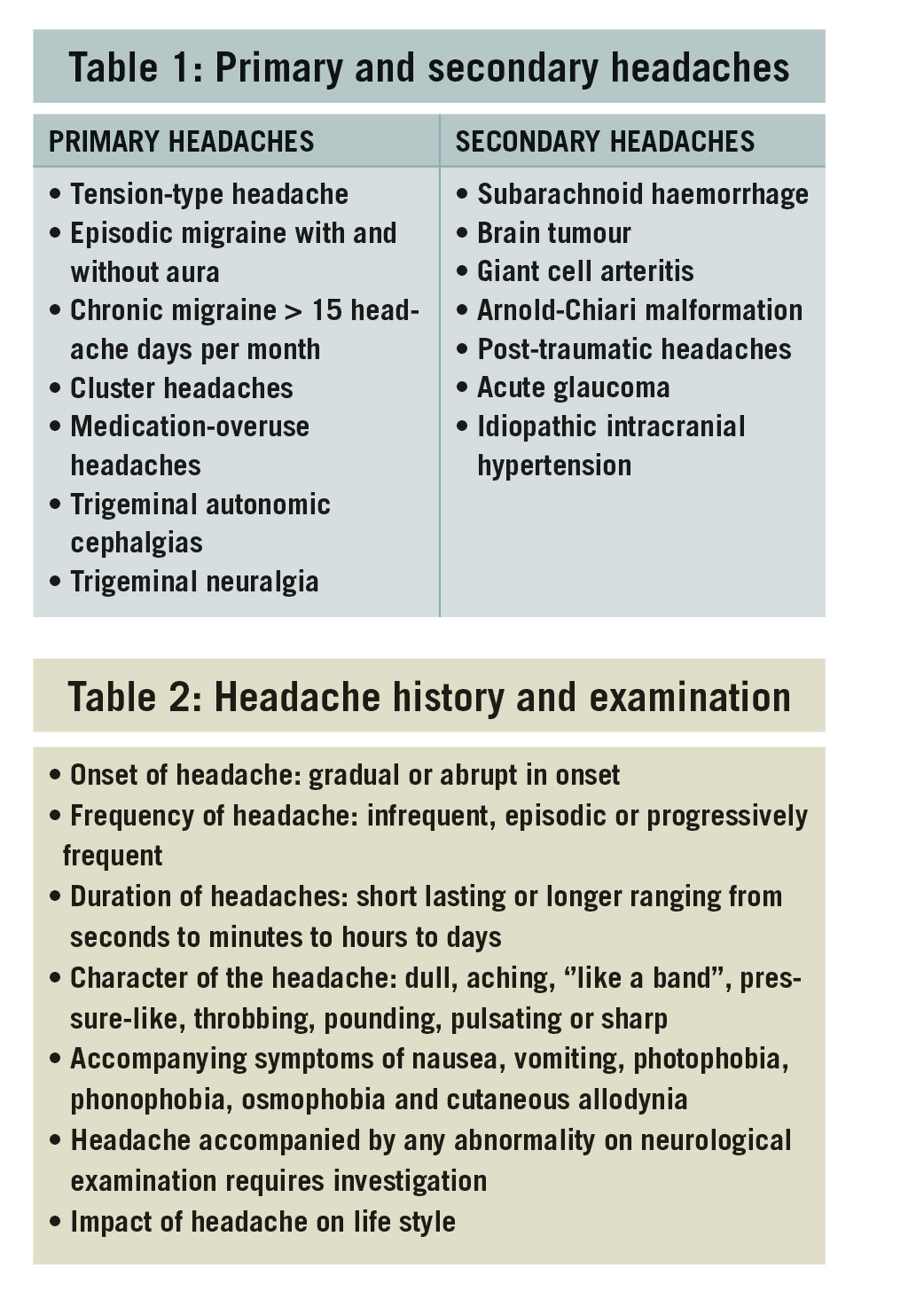
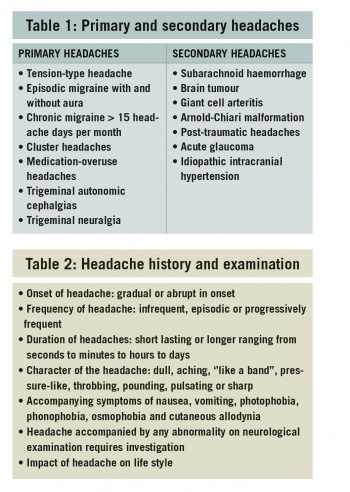
Headache is a common complaint with a lifetime prevalence of greater then 90% of the population. Most acute and recurrent headaches are benign but are frequently disabling, with the differentiation between primary and secondary headache disorders being a diagnostic challenge (see Table 1).
An accurate history and neurological examination will differentiate between those patients that need further investigations, neuroimaging and referral to the emergency or neurology department (see Table 2).
(click to enlarge)
Investigating for secondary causes
No headache symptom is pathonomic of a secondary cause but headache warning symptoms or ‘red flags’ requiring further investigations, neuroimaging and blood tests include:
• First or worst headache: ‘Thunderclap’ headache
• Progressively worsening headache over time
• New onset headache > the age of 50 years
• Headache with alteration in level of consciousness
• Headache with any abnormality on neurological examination
• Headache in the elderly accompanied by tenderness in temporal arteries or blurring of vision
• Headache associated with projectile vomiting
• ‘Side-locked’ headaches.
Investigating headaches:
CT brain scan vs MRI brain scan
In current clinical guidelines the neuroimaging investigation for secondary causes differs between acute headache presentations from those presenting with recurrent, progressive and chronic headache. In patients who present with acute or thunderclap headache, CT brain is the investigation of choice to identify a subarachnoid haemorrhage.
In contrast in patients with recurrent, frequent and progressive headaches, MRI brain is the imaging of choice for brain tumours, metastatic disease, posterior fossa lesion and Arnold Chiari malformations.
Thunderclap headache and subarachnoid haemorrhage
Thunderclap headache is defined as the sudden or abrupt onset of severe headache reaching maximum intensity within one minute. Patients typically describe it as the worst headache of their life, which is ‘explosive’ in character and in clinical practice will often reach its peak in seconds. The most important cause to consider is a subarachnoid haemorrhage caused by a ruptured aneurysm on the circle of Willis. The incidence is 9 per 100,000 per annum with an increased risk of rupture with advancing age, hypertension and cigarette smoking.
Aneurysms may rupture spontaneously but frequently coincide with physical exertion. The headache is often located in the occiput but can be holocranial and best described as pulsating, pounding or throbbing in character. Associated symptoms of neck stiffness, nausea/vomiting, photosensitivity and phonophobia may be absent in up to one-third of cases. Therefore it is the headache history and interpretation that guides and determines your clinical decision.
Thunderclap headache is a diagnostic dilemma and always requires urgent referral to the emergency department for neuroimaging and possible lumbar puncture. In addition, 30% of patients with subarachnoid haemorrhage have ‘warning’ or sentinel headaches in the weeks prior to a major rupture. Other less common causes of thunderclap headache are: cervical artery dissection, reversible cerebral vasoconstriction syndromes, cerebral venous sinus thrombosis, pituitary apoplexy and spontaneous intracranial hypotension (CSF leak).
Brain tumour headache
Brain tumours are rare and are due to primary (benign or malignant tumours) or metastatic disease, with an incidence of 10-12 per 100,000 per annum. Nevertheless both patients and doctors alike frequently ruminate about the headache being potentially caused by a tumour.
Isolated headache on its own without other clinical features such as seizures or neurological deficits is an uncommon presentation for space-occupying lesions and occurs in only 2-16%. Nevertheless brain tumour headache is more likely to occur in younger patients, in tumours that are rapidly growing and lesions located in the posterior fossa. In addition, patients with a past history of benign headache disorders such as migraine or tension-type headache are an at-risk group who may have brain tumour headache as a presenting isolated symptom. This causes diagnostic dilemmas, as a past history of migraine or tension-type headache is not necessarily a reassuring clinical feature.
The classic clinical features of brain tumour headache are that of a new onset, progressively worsening headache over time, occurring in the early morning, particularly with postural change, associated with nausea and or vomiting and is localised or ‘side-locked’ at the site of the tumour. To fulfil diagnostic criteria, brain tumour headache should resolve following neurosurgery.
The headache mechanisms of primary and secondary headache disorders are thought to have many similar pain processing features. Brain tumour headache is considered to be caused by either compression or traction on intracranial structures such as the meninges or intracranial cerebral blood vessels or by raised intracranial pressure leading to dilated ventricles. This leads to activation of sensory afferents with the headache being perpetuated due to peripheral and central sensitisation.
Giant cell arteritis
Giant cell arteritis (GCA), also known as temporal arteritis if the temporal artery is involved, is a systemic vasculitic granulomatous disorder of the medium and larger arteries. It is an important secondary headache disorder to consider in anyone presenting with new onset headache over the age of 50. The incidence rises in the elderly, 70-79 years, to 29.8 per 100,000 per annum and is more common in women.
The headache of giant cell arteritis is usually present for a number of months prior to diagnosis and its presentation may be acute, sub-acute or insidious in onset. The headache tends to become progressively worse and is moderate to severe in intensity with a predilection for involvement of the temporal artery.
In 40% of patients, the headaches are accompanied by systemic symptoms of fever, anorexia, weight loss and polymyalgia rheumatica. Jaw claudication is very pathonomic of GCA and eye symptoms of blurring of vision require immediate urgent referral for IV infusion of methylprednisolone.
Laboratory investigations of an elevated ESR (> 80mm per hour) and/or CRP are elevated in over 85% of patients and are very diagnostic of GCA and should prompt the physician to commence oral steroids of 40-60mg daily while waiting for a temporal artery biopsy.
The guidelines for suspected GCA recommend the commencement of oral steroids (prednisolone or deltacortril) at a dose of 40-60mg daily. The steroid dose can be tapered by 10mg every two weeks to 20mg daily with close monitoring via symptoms, ESR and CRP. The steroid dose is then reduced by 2.5mg weekly to 10mg daily. Further steroid reductions beyond this is by 1mg per month. Due to the commitment to long-term steroid usage patients should also be commenced on calcium, vitamin D and bisphosphonates to reduce the risk of steroid complications.
Migraine aura versus transient ischaemic attack
Migraine aura symptoms are characterised by self-limiting neurological events lasting from 5-60 minutes. These symptoms usually precede but may coincide with the headache. The aura may have both positive and negative phenomena.
The most common aura symptom is visual (90%), followed by sensory symptoms, aphasia/dysphasia and least commonly, motor weakness (hemiplegic migraine). The aura symptoms frequently follow each other during an attack beginning with the visual symptoms.
A typical visual aura consists of a scintillating (positive) scotoma (negative) that begins gradually, expanding and migrating across the visual field lasting on average 20 minutes. This may be followed by a sensory aura, frequently unilateral, beginning in the hand and migrating up the arm to the face, lips and tongue. The sensory aura also has positive (pins and needles) and negative (numbness) phenomena.
Patients who have migraine with aura experience up to 30% of attacks without a headache. Migraine aura is an independent risk factor for stroke. Patients therefore shouldn’t smoke, should be monitored for changing patterns or for prolongation of aura symptoms if on the combined OCP and should have regular blood pressure checks.
In contrast, the symptoms of a transient ischaemic attack (TIA) are abrupt in onset and neurological symptoms may feature hemiparesis, hemisensory loss, aphasia, amaurosis fugax or ataxia. At least one of these symptoms reaches maximal intensity within one minute and more than one symptom occurs at the same time. A TIA completely resolves within 24 hours. TIAs are not usually associated, accompanied or followed by headaches.
Migraine aura is the most frequent mimic for a TIA and differentiating between the two can at times be challenging, even in specialist neurological centres and stroke units. This sometimes results in migraine with aura patients having thrombolysis, although they are unlikely to come to any harm due to the procedure.
Carbon monoxide poisoning and headaches
Headache accompanies most patients with carbon monoxide poisoning. The headaches are non-specific, range in severity, and are most frequently located in the bilateral frontal regions but can vary in locations. The character of the headache ranges from being dull and aching to a throbbing/pounding headache. The severity of the headache does not correlate with the degree of exposure to carbon monoxide.
Diagnosis of carbon monoxide poisoning is based on known or suspected exposure leading to headache and other symptoms of toxicity such as altered level of consciousness, confusion, nausea, unsteadiness and tachycardia. Hyperbaric oxygen is the treatment of choice and provides complete headache relief and resolution of other symptoms.
Acute glaucoma
Acute narrow angle glaucoma is an important diagnosis not to be overlooked in anyone who presents with new-onset headache over the age of 40. Risk factors are: positive family history, women, and hypermetropia (far-sightedness). It is frequently a strictly unilateral headache (‘side-locked’) located in the periorbital region.
The character of the headache is non-specific, is usually non-pulsatile, mild to moderate in severity and commonly occurs at night in dim light. The presence of a red eye, tearing and haloes around light raises awareness. Attacks may begin episodically and become more frequent. Clinically attacks tend to be shorter in duration (~ 2 hours) than migraine attacks, which is an important differentiating pointer. Acute narrow angle glaucoma is an ophthalmic emergency and requires immediate referral for further investigations and management.
Benign headache disorders
The introduction of the International Headache Society’s (IHS) diagnostic guidelines for headache disorders, many decades ago, has greatly facilitated physicians in clinical practice. Their usage is now universally adopted by clinicians and researchers alike. These guidelines enable good clinical practice and epidemiological studies, research and clinical trials to be carried out to the highest of standards. There are over 150 different headache disorders and the common ones are listed in Table 1.
Tension-type headache
In the community, tension-type headache is the most common headache disorder. The symptoms are low grade and non-specific and the features are typically of a dull aching, tightness, ‘like a band’ headache that is either generalised or located in the bilateral frontal regions. Tension-type headaches are usually mild and self-limiting and patients frequently self-medicate with simple over-the-counter analgesics such as paracetamol, aspirin or ibuprofen.
Migraine with and without aura
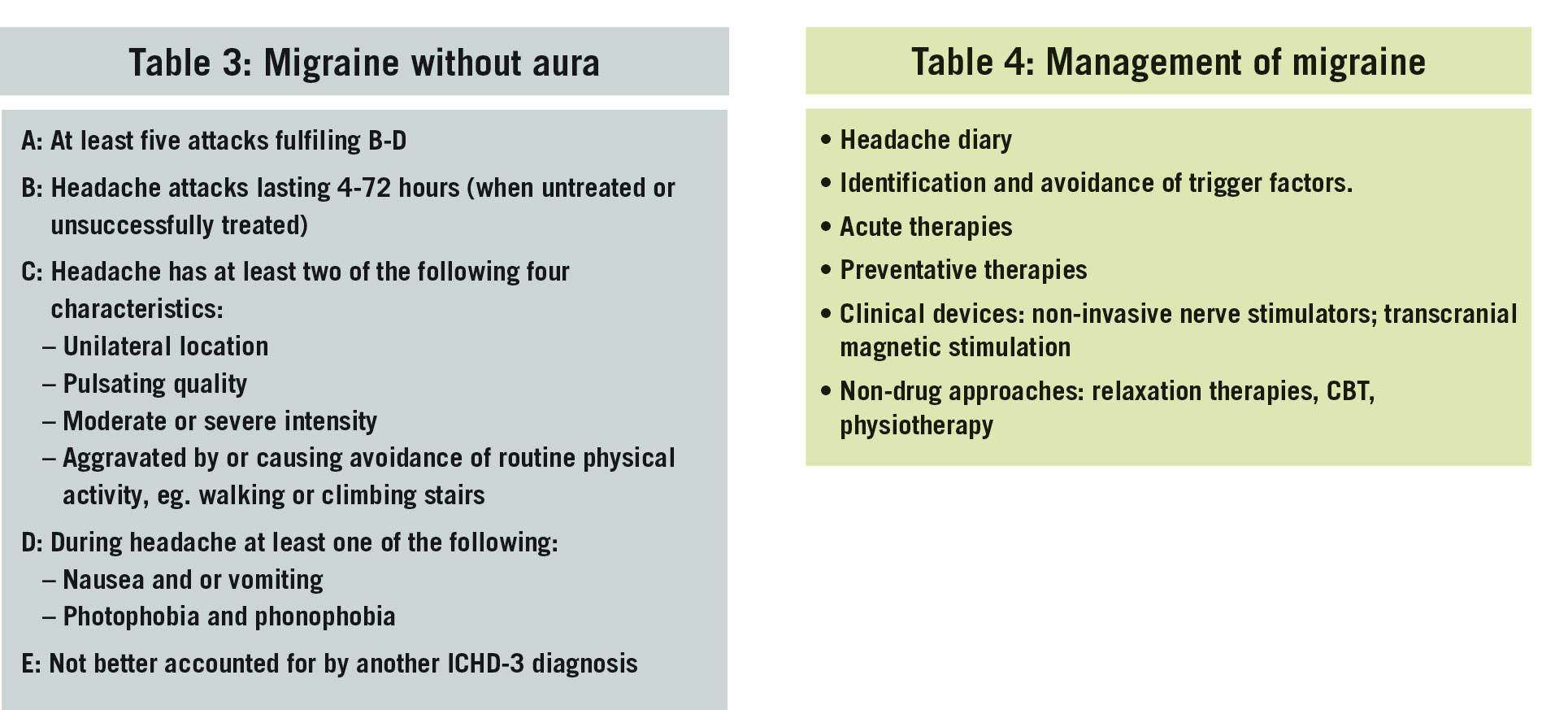
The World Health Organization recognises migraine as the fifth leading cause of years lived with disability for women and the seventh for men. Migraine occurs in 10-12% of the population with a female:male ratio of 3:1. It frequently begins in the late teens or early 20s and can be a life-long disorder. The International Classification of Headaches Disorders diagnostic criteria are outlined in Table 3.
Aura symptoms precede or coincide with the headache in 30% of migraneurs. The aura is defined as a transient focal neurological symptom lasting from 5-60 minutes that is completely reversible. The most common aura is visual, consisting of flashing lights, zig-zag lines, fortification spectra and an expanding scotoma. This may be followed by sensory symptoms of either ‘pins and needles’’ or numbness. Other aura symptoms include dysphasia and motor weakness. Management principles for migraine are outlined in Table 4.
(click to enlarge)
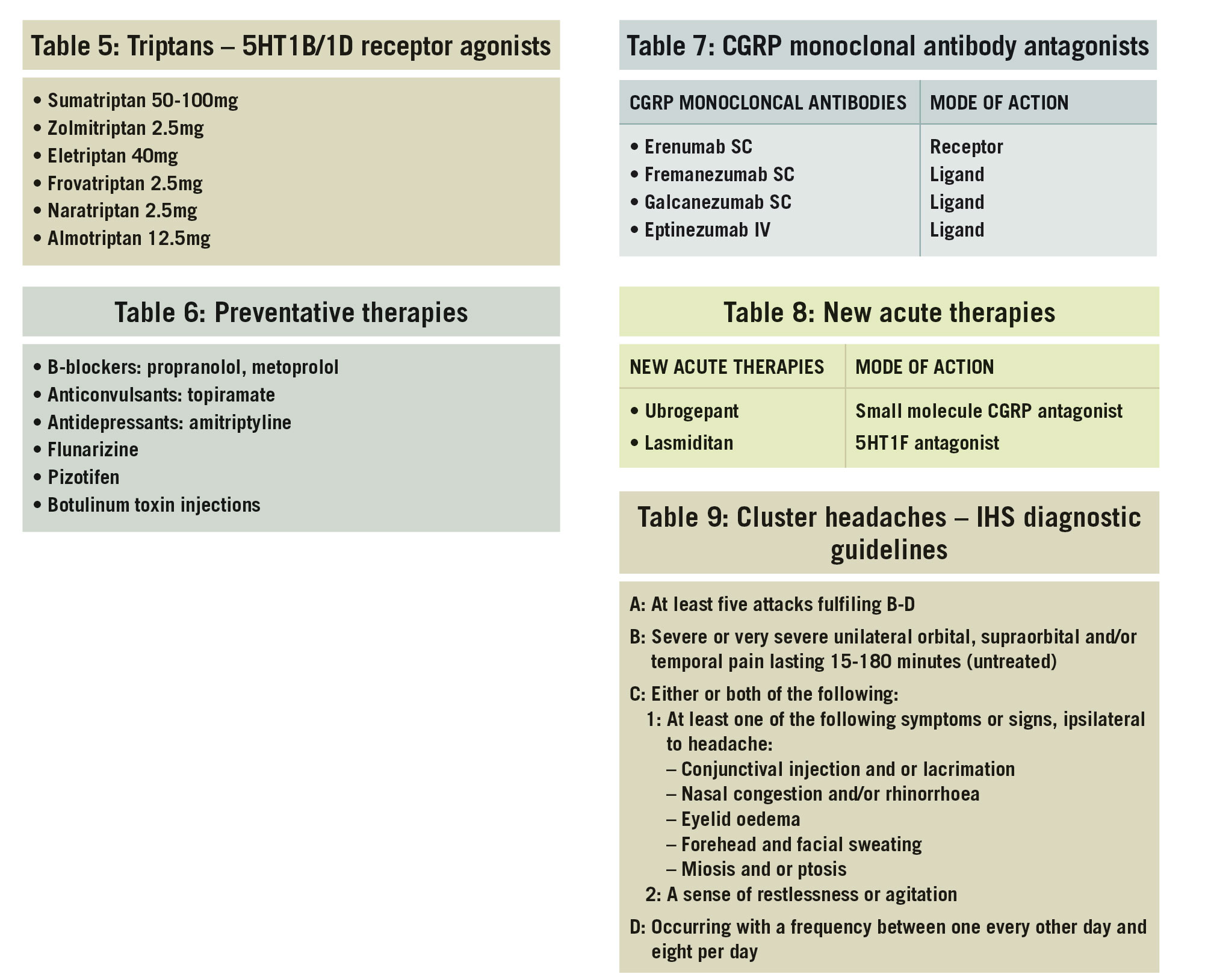
In the treatment of acute attacks up to one-third of patients successfully self-medicate with simple analgesics such as aspirin, paracetamol or ibuprofen. For others however, migraine is a disabling disorder, unresponsive to conventional OTC analgesics and frequently goes undiagnosed and undertreated. In this cohort, the triptans (5HT1B/1D receptor agonists) are first-line recommendations and agents from this class are listed in Table 5.
All acute therapies, analgesics and triptans, should be taken as early as possible during the headache in order to maximise the efficacy. They may also be combined with anti-emetics.
Preventative therapies are indicated in patients who experience two to four attacks per month, particularly if they are unresponsive to acute therapies. All preventative therapies to date were initially licensed for different conditions. Serendipitous observations over time demonstrated their benefits in migraine prevention. The currently recommended preventative therapies are listed in Table 6.
The goals of preventative therapies are to reduce the frequency, severity and duration of attacks and to lower the impact burden of migraine. In responders, good efficacy reduces attacks by 50% in 50% of patients.
Chronic migraine
Migraine is a progressive disorder in 10% of migraneurs with patients at risk of developing chronic migraine. It is defined as a headache occurring on more than 15 days per month of which eight attacks retain the features of debilitating episode migraine. It has peak prevalence in women in their 40s. Many of these patients also overuse medication due to the increasing reliance on simple analgesics, compound analgesics and triptans for pain relief.
The guiding principles of management are to limit the use of acute therapies to two to three days per week and to introduce migraine preventative therapies. Non-drug approaches and accurate headache diaries are important adjunct measures to monitor progress.
New and emerging treatments for migraine
The clinical guidelines in migraine management will soon be overhauled with the imminent arrival of new therapies. The most immediate impact will be in the area of prevention, with the approval of a new class of migraine preventative therapies known as CGRP monoclonal antibody antagonists outlined in Table 7.
The CGRP monoclonal antibodies are likely to be licensed for patients who suffer from four or more migraine days per month. They will be particularly important for patients who suffer from chronic migraine, medication overuse, and in those who have failed to benefit from two or more conventional preventative therapies.
The triptans (eg. sumatriptan, zolmitriptan) have been the gold standard in the treatment of acute migraine attacks for more then two decades. However, they have limitations, as at least 20% of patients are non-responders. They are contraindicated in patients over 65, with ischaemic heart disease and uncontrolled hypertension. These unmet needs may soon be addressed by new acute therapies that are now in late stage clinical development, see Table 8.
Cluster headaches
Cluster headache is a rare very disabling condition (prevalence: 0.1-0.7%) and belongs to a group of benign headache disorders classified as trigeminal autonomic cephalalgias. Cluster headache can occur in episodic or chronic forms. The diagnostic features are outlined in Table 9.
(click to enlarge)
Cluster headaches typically occurs in bouts, with attacks occurring a number of times per day for weeks or months and then goes into remission for months or even years, hence the term ‘cluster’. It is more common in men, with peak prevalence being between the ages of 20-40.
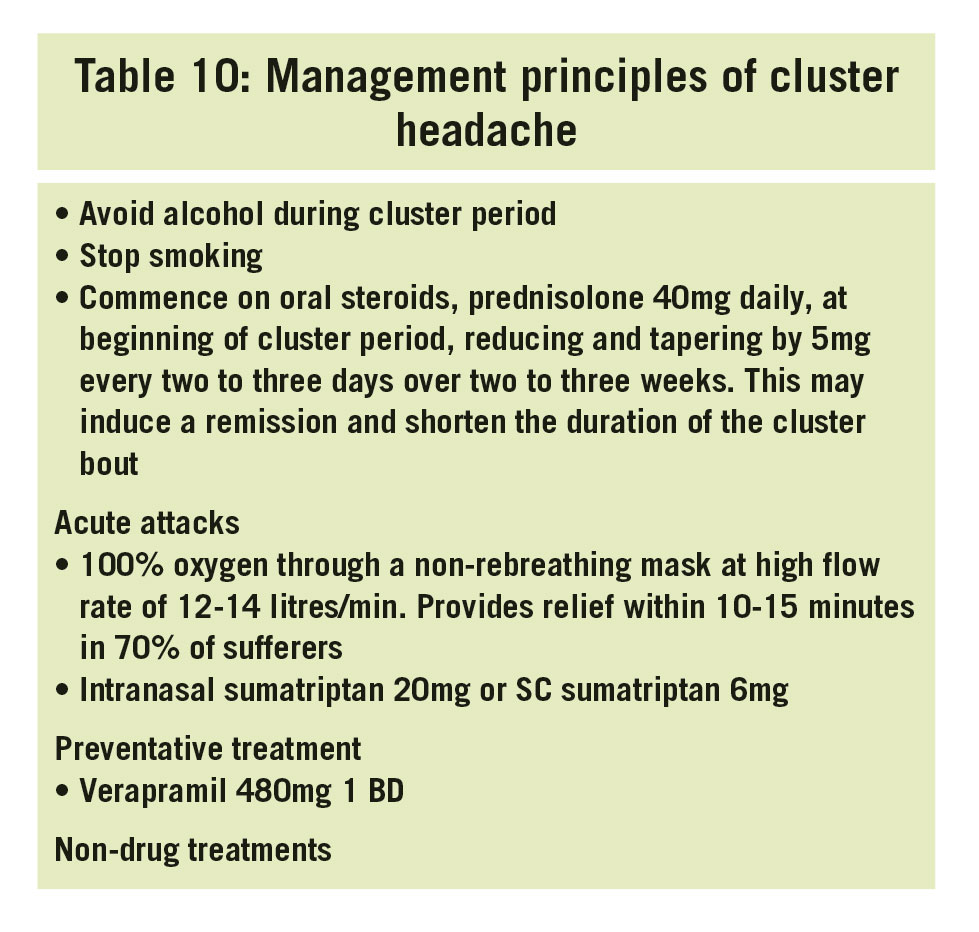
It is important to recognise and distinguish cluster headache from other conditions such as sinus disease, eye problems and migraine, as the management of an attack is very specific for the disorder. Patients are vulnerable to cluster periods in early spring and autumn and both alcohol and cigarettes are triggers during bouts. The management of cluster headache is outlined in Table 10.
(click to enlarge)
Conclusions
There are over 150 different headache disorders whose diagnostic criteria are outlined in the International Headache Society’s classification. An accurate detailed history and examination is the cornerstone to good clinical practice and delineates between benign and secondary disorders.
The ‘red flags’ alert doctors to the potential of secondary causes and the need for urgent referral to emergency departments or for further investigation and referral to neurology departments.
Greater then 95% of patients who present to their GP with the symptom of headache are suffering from a benign headache disorder, which in a general practice setting is most likely to be migraine. The management of migraine and other benign headaches needs careful monitoring with the use of headache diaries. This enables the efficacy of acute and preventative treatments to be evaluated over time and further changes made if necessary.
Management guidelines in migraine are about to change with the anticipated arrival of CGRP monoclonal antibodies for prevention and 5HT1F antagonists and small molecule ‘gpants’ as alternatives to the triptans in the treatment of acute attacks.
(This module was facilitated by Dr Edward O’Sullivan)
Reference
International Headache Society’s (IHS) diagnostic guidelines for headache disorders, 3rd edition, accessible on http://www.ihs-headache.org/ichd-guidelines
 (click to enlarge)
(click to enlarge)