GPs are the first and ongoing point of contact for patients presenting with mental health difficulties in Ireland.
Many mental illnesses are predominantly managed in primary care in Ireland.1 It is also estimated that 45% of those who die by suicide see their GP in the week prior to death.2
This group of patients poses a particular challenge for GPs. This is highlighted in a recent major study conducted by the HSE National Office for Suicide Prevention (NOSP) and the ICGP,3 which shows, in addition to the obvious traumatic effect on the family and friends of the person who takes their own life, that there is also an effect on the GP. GPs point to feelings of shock, sadness, reduced confidence and frustration at the lack of training provided to them to deal with these cases and the dearth of supports and policies in place to deal with suicidal patients.
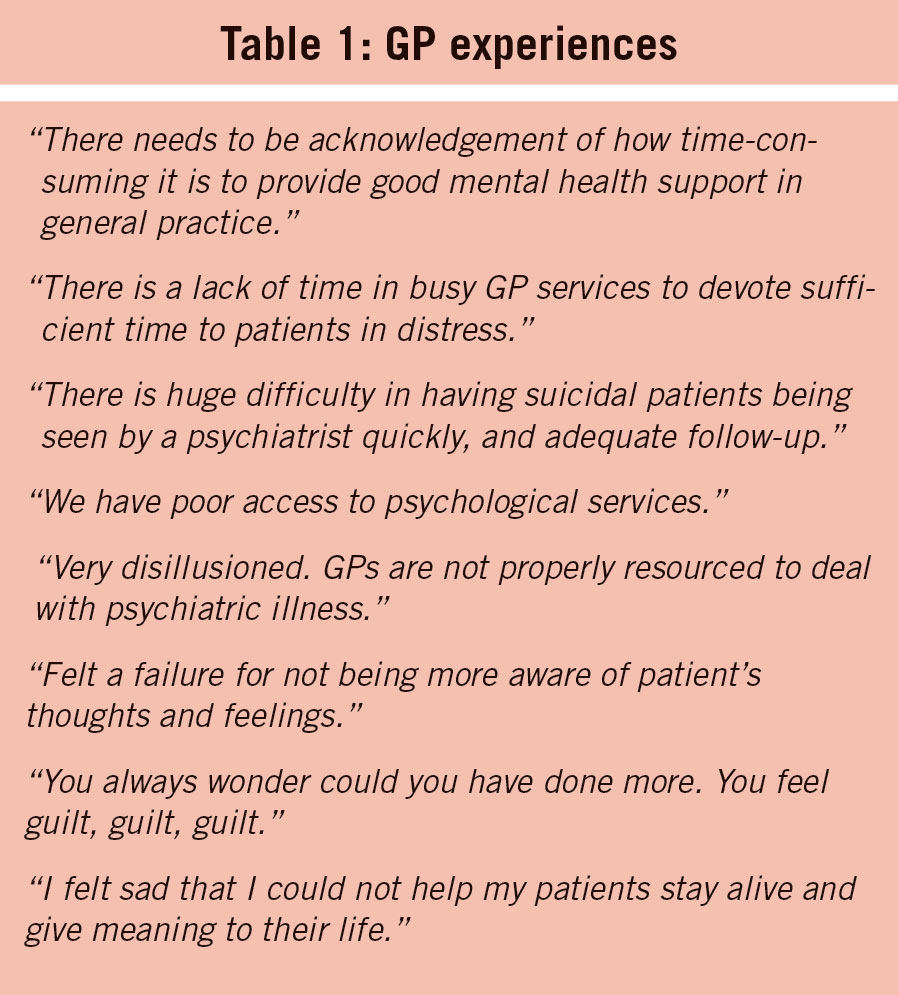
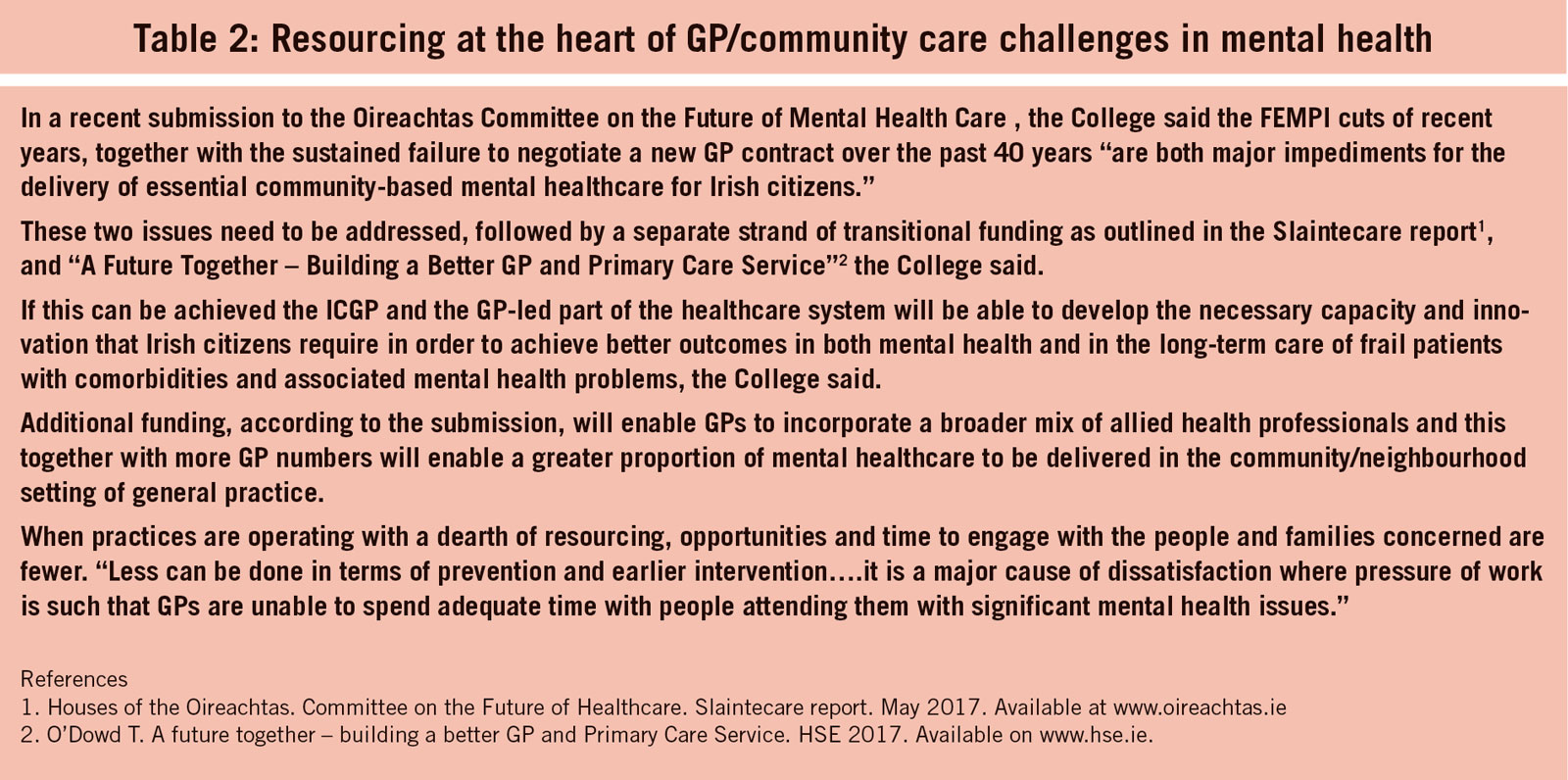
The quotes of individual GPs taken from the report (see Table 1), give a flavour of the views expressed in the NOSP/ICGP survey about service and support deficits in mental healthcare (expressed also in a recent ICGP submission to an Oireachtas committee – seeTable 2). GPs point specifically to deficits in suicide prevention supports and to effects of a patient suicide on the individual GP and practice staff.
(click to enlarge)
(click to enlarge)
The NOSP/HSE study comprised a survey of 469 GPs across nine HSE Community Health Organisations (CHOs). The vast majority of GPs surveyed (77%) reported having experienced a patient suicide. Most of these said patient suicide(s) had had an adverse effect on them. It was also found that:
•The majority of GP respondents had not undertaken any previous suicide prevention training. Those who had undergone training showed more positive attitudes towards suicide prevention, more confidence in dealing with patient needs and in identifying appropriate services for onward referral
•Only a small proportion of GPs had actually received training on formalised assessment of suicide risk. The majority (81%) had not undertaken any previous suicide prevention training
•Two-thirds reported that they did not have adequate preparation for their role in the use of a safety plan
•GPs reported limited access to specialist support services, either within their practice, or in terms of personal liaison with psychiatric services
•The most commonly experienced gaps in services for suicidal persons identified by GPs included: “accessing urgent statutory mental health services, including child and adolescent services”, and “accessing crisis counselling/support services.
The ‘top five’ ranked gaps in services for suicidal patients identified by GPs were:
• Access to crisis counselling
• Access to services (eg. addiction services)
• Access to statutory services for children and adolescents
• Access to psychological support services
• Access to urgent statutory mental health services/triage.
While it is estimated that around 45% of those who die by suicide saw their GP in the month before death,2 only 20% saw a mental health professional.
Another review showed that up to 25% of patients who die by suicide visited their GP in the week before they died.
This does not mean that patients of GPs who died by suicide told their GP of their intention to take their own lives during the last consultation; in fact suicidal ideation is rarely discussed in these circumstances.
The NOSP/ICGP report stresses that with many mental health problems managed in primary care and the high prevalence of mental illness among those who die by suicide, the role of the GP is important in recognising and providing the necessary treatment to individuals who may be at risk of suicide.
There is also evidence that initiatives within primary care, including screening of those felt to be at increased risk, can contribute to suicide prevention.4 The report says there is also evidence to support the benefits of education and training on suicide prevention in primary care.5
However, as the GP findings and comments in the report indicate, the ideal is very far from the reality. For example, only one-third of GP respondents said their practice had a personal liaison with psychiatric services, and only 15% said they had additional practice services to deal with suicidal persons.
While the report pointed to the vast majority of GPs not having had any training in suicide prevention, those who had undertaken such training self-reported more positive attitudes towards suicide prevention.
Connecting for Life (CfL) is a national, coordinated multifaceted strategy to reduce deaths by suicide and self-harm that recognises the important role of primary care and the GP in suicide prevention.
Under this strategy, 17 multi-agency area level suicide prevention action plans have been developed and are aligned with the national strategy on suicide prevention. These plans focus on bringing together a wide range of stakeholders to help lay the foundations for effective implementation of the national strategy at local level.
However, the GP survey found that the vast majority of GPs were not yet familiar with their local area CfL action plan. Moreover, the majority of GPs, it was found, did not know about the local resource officer for suicide prevention. Just over one-in-five said they knew about this local officer, but had had no contact with them in the past.
The report concludes that suicide prevention in primary care is important but very challenging for GPs and that the evidence points to the benefits of GPs having training on the management and recognition of this risk.
“However, in order to facilitate GPs to manage patients with suicidal behaviour, improved connections with and access to mental health services are essential,” it concludes.
ICGP Director of Mental Health Services Dr Brian Osborne said the survey is very welcome. He pointed out that plans are underway to roll out a national programme of further education for GPs on suicide prevention and self-harm, in collaboration with the NOSP.
He pointed out that GP trainees are taught to conduct clinical suicide risk assessments as part of their training. In addition, the college has collaborated with the NOSP since 2014 to develop and continuously offer an e-learning module on suicide prevention in general practice.
Brian added that mental health and suicide prevention updates are also regularly in the programme of continuing education the ICGP offers. “However, we welcome this opportunity to partner with the NOSP again to further strengthen our practices,’ he said.
The NOSP and ICGP will shortly begin a national practice programme and development project to address many of the needs identified in the survey. According to Brian Osborne, the aim of this project is to simplify and support good and safe practice in a way that will have beneficial impact on GPs’ care of suicidal patients.
References
McDaid S. Mental Health in Primary Care in Ireland: A briefing Paper. Mental Health Reform, Dublin, (2013)
Luoma J, Martin C, Pearson J. Contact with mental health and primary care providers before suicide: A review of the evidence. American Journal of Psychiatry 2002; 159 (6):909-16
Suicide prevention: GPs’ professional views and practice experience-NOSP(HSE) and ICGP. 2018. Available on www.hse.ie and www.icgp.ie
Vannoy SD, Robins LS. Suicide related discussions with depressed primary care patients in the USA: gender and quality gaps. British Medical Journal 2011 Open 1(2)
Morriss R, Gask L, Webb R et al. The effects on suicide rates of educational intervention for frontline health professionals with suicidal patients. (The STORM project) Psychological Medicine 2005; 35,957-960
 (click to enlarge)
(click to enlarge)