History and prognosis of chronic obstructive pulmonary disease
Factors influencing the variable prognostic indicators for COPD need further research
Dr Minesh Kooblall, Respiratory Registrar, Tallaght Hospital, Dublin and Dr Edward Moloney, Consultant Respiratory Physician, Respiratory Department, Tallaght Hospital, Dublin
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory disease characterised by progressive airflow limitation resulting in breathlessness and other associated symptoms. Worldwide, it is a significant cause of morbidity and it is estimated it will be the fourth leading cause of death by 2030. In Ireland, the exact prevalence of COPD is unknown but is estimated to be around 440,000 with significant levels of underdiagnosis.
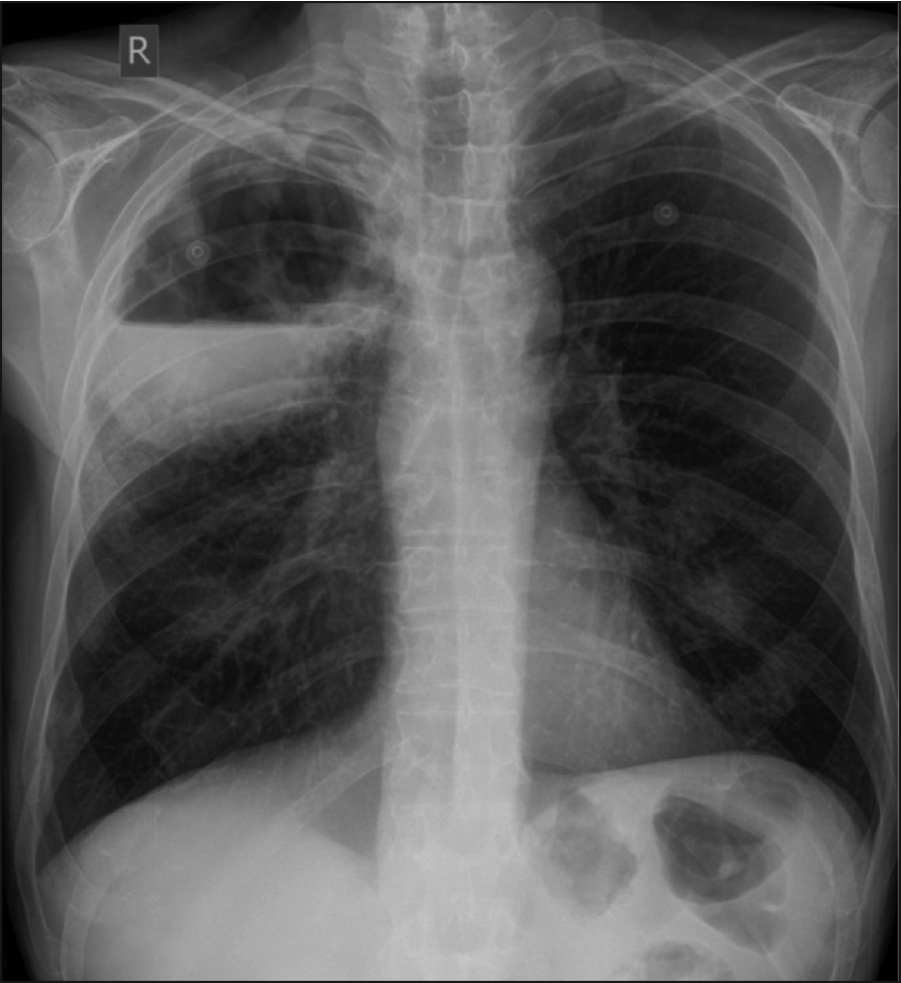
Figure 1. Chest x-ray showing a large cavitating lesion in the right upper lobe(click to enlarge)
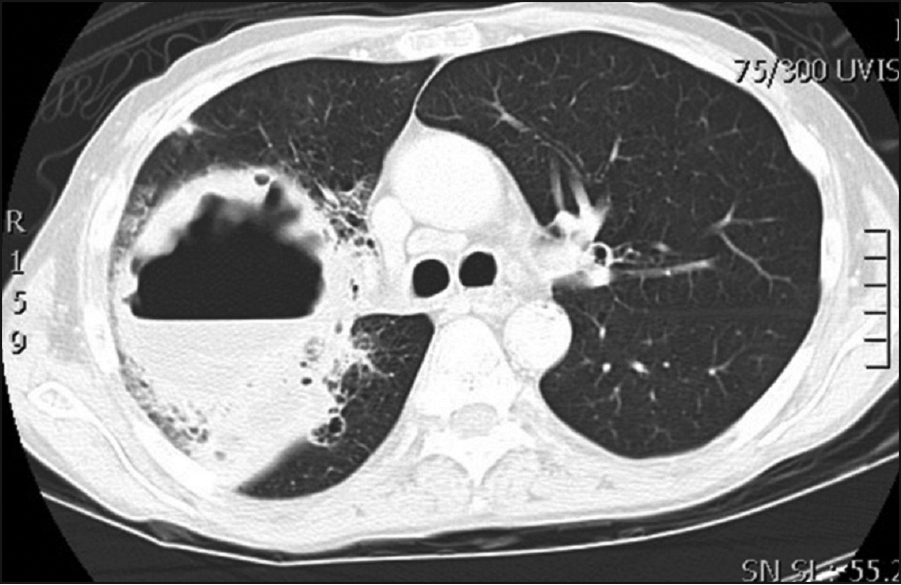
Figure 2. A CT chest with contrast showed a 13x10x12cm cavitating lesion predominantly in the right upper lobe(click to enlarge)
Figure 3. CT scan showing subcutaneous emphysema(click to enlarge)
A number of factors have been identified as prognostic indicators for COPD. In addition to the forced expiratory volume in one second (FEV1), other predictors of accelerated lung function decline, diminished physical function, and/or mortality in patients with COPD include:
Airways responsiveness
Cigarette smoking
Low body mass index (BMI ≤ 21)
HIV infection
Increased airway bacterial load
Decreased exercise capacity
Peak oxygen consumption (VO2), measured by cardiopulmonary exercise testing
Elevated C-reactive protein (>3mg/L)
Male gender
Chest computed tomography showing presence of emphysema.
The following cases illustrate three COPD patients who presented to the emergency department.
Case 1
A 58-year-old gentleman presented with diarrhoea of more than four weeks, with a concern that it was not improving and he was unable to cope at home. He was experiencing loose watery diarrhoea up to nine times a day with occasional faecal incontinence. He stated that he had had chronic diarrhoea in the past but usually it had settled within two to three weeks. He denied any per rectum bleeding, constipation, abdominal pain or cramps. Of note, he denied having any chills, rigors, fevers, productive coughs, dysuria, chest pain or any new dyspnoea. There was no history of tuberculosis exposure.
His medical history included COPD from being a life-long heavy smoker, having osteoporosis, a right hip dynamic hip screw inserted in March 2012 for a fracture sustained following a mechanical fall, hypercholesterolaemia and alcohol-related liver disease. He currently lives with his wife who is the primary carer; he smokes up to 20 cigarettes a day and drinks up to four beers a day in addition to a bottle of wine. His previous exacerbation of COPD was more than one year ago when he was admitted to hospital for three days for a course of intravenous antibiotics, oral corticosteroids and inhalers. His wife is also a heavy smoker. Prior to being diagnosed with COPD, he was a manual tradesman by profession and denied having any exposure to any occupational agents such as asbestos. There was no history of recent overseas travel in the past five years.
On examination, he appeared malnourished but was not tachycardic, tachypnoeic and exhibiting oxygen saturations of 97% on room air. His temperature was 36.2°C and he appeared slightly dehydrated. He had poor dentition with significant decay of many teeth. There was decreased air entry right upper lobe and fine crackles. He had a palpable liver edge but otherwise an unremarkable abdominal examination.
The bedside urinalysis was clear and the ECG was showing a sinus rhythm. His blood tests were predominantly unremarkable with the exception of a C reactive protein of 117 (<10mg/l) and mildly deranged liver function tests. The total white cell count (WCC) was 9 (4-10x109/l). Quantiferon, ACE, ANCA were negative. The chest x-ray showed what appeared to be a large cavitating lesion in the right upper lobe with an air/fluid level (see Figure 1).
A CT chest with contrast was performed which showed a 13x10x12cm cavitating lesion with a large air/fluid level predominantly in the right upper lobe (see Figure 2). Associated with it, there was prominent reactive adenopathy in the superior, anterior mediastinum, as well as in the subcarinal position (see Figure 2).
A CT-guided biopsy confirmed a methicillin-resistant Staphylococcus aureus-positive lung cavitation, most likely secondary to his poor dentition. A full dental clearance was performed, and he was treated with a course of intravenous vancomycin and oral clindamycin with good effect.
Learning points of Case 1
In chronic obstructive pulmonary disease patients presenting with fluid-filled chest cavities, consider an infection of an emphysematous bulla.
Infected emphysematous bullae are common but under-reported.
Strive to obtain previous chest radiography to assist with the diagnosis.
Percutaneous drainage/biopsies provide rapid symptomatic relief and enable titration of antibiotics to the causative microbe.
Treat methicillin-resistant S. aureus-positive infections as a matter of urgency with vancomycin and an appropriate oral stepdown.
Case 2
This is a case of a 75-year-old man with severe smoking related COPD who presented with a secondary pneumothorax. Attempts to treat a persistent air leak using intercoastal (IC) drains of increasing size led to sudden worsening of iatrogenic subcutaneous emphysema. A CT scan performed confirmed the presence of a pneumomediastium and florid subcutaneous emphysema in the face and torso (see Figure 3). Although the patient reported a change in voice with hoarseness there was no evidence of airway compromise. The patient was conservatively managed in the high-dependency unit. He was not considered fit enough to undergo general anaesthesia and surgery; therefore, a pleurodesis using sterile talc was undertaken. The IC drain was successfully removed, following resolution of the air leak and the lung remained re-inflated. His subcutaneous emphysema gradually spontaneously resolved with no further complications.
Learning points of Case 2
COPD patients are at higher risk of developing secondary pneumothorax.
Self-limiting complications have potential to develop rapidly and unexpectedly, emphasising the importance of dealing with the basics and assessing change systematically.
Subcutaneous emphysema can be potentially serious, and patients should be stabilised and managed as appropriate.
Case 3
A 59-year-old man presented to hospital with a two-week history of gradually increasing breathlessness and decreased exercise tolerance. He suffered from grade B COPD and coeliac disease with coexisting dermatitis herpetiformis. Preadmission treatment with oral steroids and antibiotics had failed to improve his symptoms.
Physical examination demonstrated the patient to be peripherally cyanosed (peripheral oxygen saturation, SpO2 85% on 4 l/min of O2) and tachypnoeic (20bpm). His blood pressure and pulse rate were normal. Auscultation of the chest revealed mild bi-basal crackles without wheeze.
Blood profiling: haemoglobin 10.5g/dl, white blood cell count 9.1×109/l, C reactive protein 125.5mg/l.
Plain chest radiograph showed patchy left-sided pneumonic changes consistent with infection on a background of hyper-inflated lungs. Treatment of infective exacerbation of COPD was started with flow-controlled oxygen, intravenous antibiotics, nebulised bronchodilators and corticosteroids. Despite significantly improved inflammatory markers and clinical symptoms, the patient remained cyanosed and persistently hypoxic on pulse oximetry.
Further arterial blood investigations with the patient breathing ambient air revealed a ‘saturation gap’ with a discrepancy between his measured peripheral oxygen saturation (SpO2) and calculated haemoglobin oxygen saturation (SaO2): pH 7.44, PCO2 5.37 kPa, PO2 7.77 kPa, HCO3 27.1mmol/l, SaO2 86.4%, SpO2 79%. Co-oximetry was performed to determine the presence of dyshaemoglobins and revealed a significantly raised fraction of methaemoglobin (FMetHb) level of 13%.
The patient had been taking dapsone for dermatitis herpetiformis since 2006. A baseline FMetHb level of 1.5% at the start of treatment had gradually increased over time. A diagnosis of acquired methaemoglobinaemia secondary to the dapsone therapy was thus considered. The implicated drug was stopped and replaced with topical mometasone furoate with advice from the dermatologist.
Learning points from Case 3
Failure to identify more unusual causes of hypoxia may lead to missed opportunities for earlier intervention.
Causes of methaemoglobinaemia can be either congenital or, more commonly, acquired.
Common causes of acquired methaemoglobinaemia include agents which inflict a significant oxidant stress on cells.
Patients with a coexisting impairment in oxygenation may develop clinical features including cyanosis with only a modest elevation of the fraction of methaemoglobin level.
Conclusion
The natural history and prognosis of COPD are variable and factors influencing this variability are incompletely understood. A number of factors, such as genetic predisposition, severity of disease, environmental exposures, comorbidities, and, to a lesser degree, acute exacerbations, appear to influence prognosis. Short-term (ie. in-hospital) survival for patients with COPD and respiratory failure is determined by the overall severity of acute illness, rather than the degree of respiratory failure. In comparison, long-term survival is primarily influenced by the severity of COPD and the presence of comorbid conditions.
COPD is associated with a number of comorbid conditions, such as cardiovascular diseases (for example, hypertension, coronary heart disease, stroke), diabetes mellitus, renal insufficiency, osteoporosis, psychiatric illness (for example, depression and anxiety), and cognitive dysfunction.
An infected pulmonary bullae, complicated pneumothorax and methaemoglobinaemia is only the tip of the iceberg in this COPD arena. It is almost always a long-term or permanent disability and there is no cure for the condition.
The National Clinical Programme for COPD in Ireland now provides greater awareness of this disease with early detection and early management with greater emphasis made on primary prevention (smoking cessation).
References
Mathers DC, Loncar D. Projections of global mortality and burden of disease from 2002 to 2039. PLoS Med 2006;3:e442
Schirnhofer L, Lamprecht B, Vollmer WM et al. COPD prevalence in Salzburg, Austria: results from the Burden of Obstructive Lung Disease (BOLD) Study. Chest 2007; 131: 29-36
Celli BR, Cote CG, Marin JM et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med 2004; 350:1005
Heffner JE, Mularski RA, Calverley PM. COPD performance measures: missing opportunities for improving care. Chest 2010; 137:1181
Hospers JJ, Postma DS, Rijcken B et al. Histamine airway hyper-responsiveness and mortality from chronic obstructive pulmonary disease: a cohort study. Lancet 2000; 356:1313
Diaz PT, King MA, Pacht ER et al. Increased susceptibility to pulmonary emphysema among HIV-seropositive smokers. Ann Intern Med 2000; 132:369
Wilkinson TM, Patel IS, Wilks M et al. Airway bacterial load and FEV1 decline in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2003; 167:1090
Berry MJ, Adair NE, Rejeski WJ. Use of peak oxygen consumption in predicting physical function and quality of life in COPD patients. Chest 2006; 129:1516
Dahl M, Vestbo J, Lange P et al. C-reactive protein as a predictor of prognosis in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2007; 175:250
Drummond MB, Blackford AL, Benditt JO et al. Continuous oxygen use in nonhypoxemic emphysema patients identifies a high-risk subset of patients: retrospective analysis of the National Emphysema Treatment Trial. Chest 2008; 134:497
de Torres JP, Cote CG, López MV et al. Sex differences in mortality in patients with COPD. Eur Respir J 2009; 33:528
Kohansal R, Martinez-Camblor P, Agustí A et al. The natural history of chronic airflow obstruction revisited: an analysis of the Framingham offspring cohort. Am J Respir Crit Care Med 2009; 180:3
Haruna A, Muro S, Nakano Y et al. CT scan findings of emphysema predict mortality in COPD. Chest 2010; 138:635
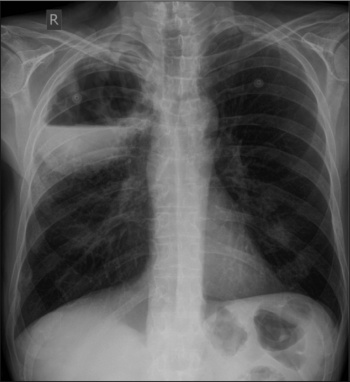 Figure 1. Chest x-ray showing a large cavitating lesion in the right upper lobe(click to enlarge)
Figure 1. Chest x-ray showing a large cavitating lesion in the right upper lobe(click to enlarge)