The American Heart Association (AHA) and American College of Cardiology (ACC) have considerably lowered hypertension treatment thresholds in recently-published guidelines.1 The new guidelines have generated much debate about the pros and cons of ‘going so low’ with these thresholds.
The new guidance has met with a generally positive reception in terms of the proven benefits shown to date from more aggressive treatment of hypertension, but there have been caveats on the widening of the criteria, particularly in view of the fact that this would lead to a far greater number of people being classified as hypertensive and treated accordingly.
It has been pointed out that under the new guidelines, around half the US population would be designated as having high blood pressure, thereby creating issues around potentially generating a huge cohort of ‘worried well’.
(click to enlarge)
(click to enlarge)
Health service resource concerns
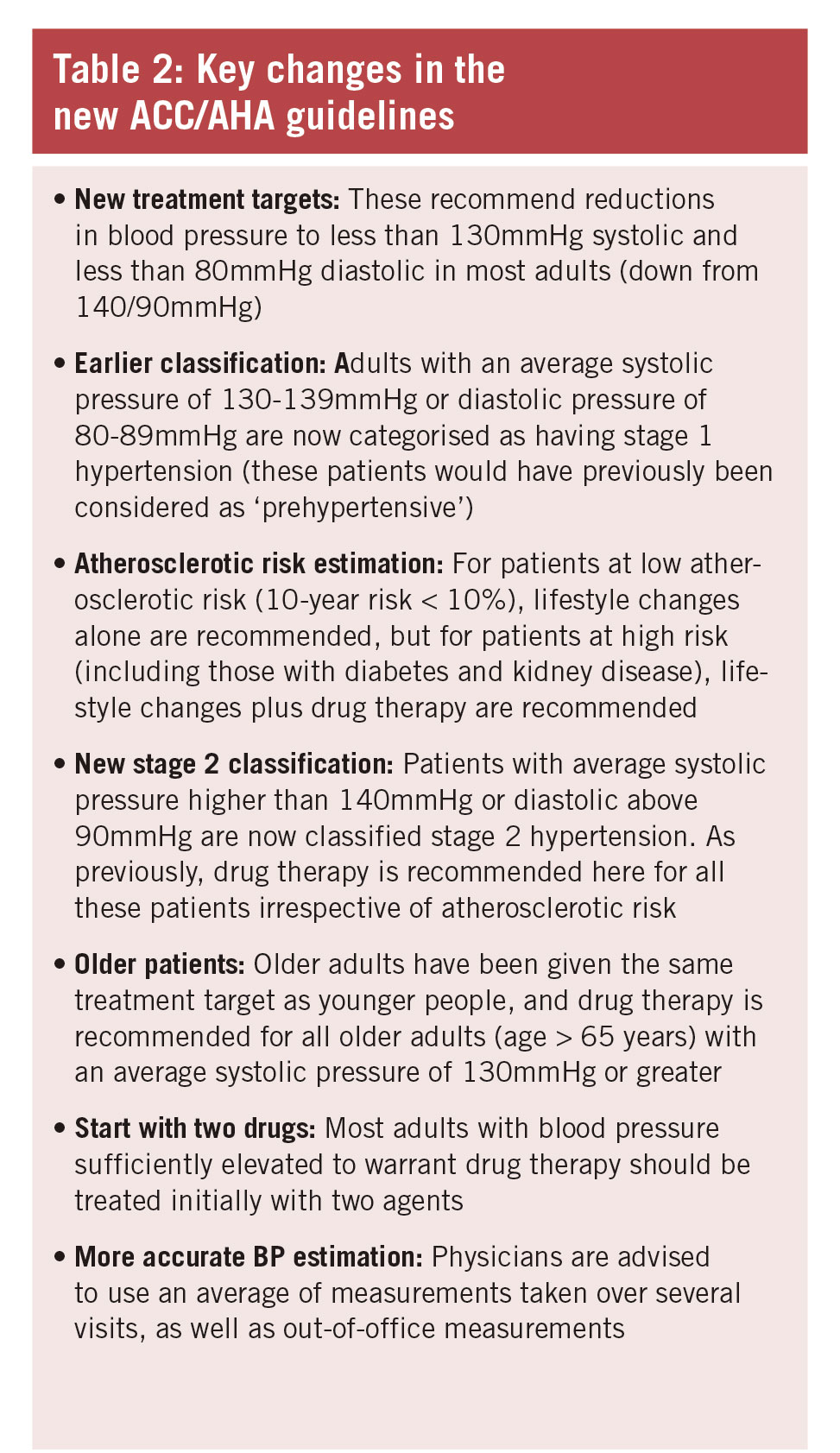
In addition, there are health service resource concerns about the cost of screening and treatment for these additional patients, as well as concerns about possible over-aggressive treatment of hypertension in the elderly. The new guidelines would result in all adults over 65 with systolic BP of 130mmHg receiving drug therapy for hypertension
These guidelines are heavily influenced by the 2015 SPRINT Trial,2 which involved over 9,000 hypertensive adults. This trial was the largest study of its kind to examine how keeping systolic blood pressure at lower than previously recommended levels would affect outcomes in patients at high risk for heart disease. The results showed that lowering systolic BP to 120mmHg or less compared with 140mmHg or less in adults over 50 with CVD risk significantly reduced death from all causes, and specifically from heart failure and heart attack. The SPRINT trial was terminated early due to the positive benefits shown with the lower blood pressure target group.
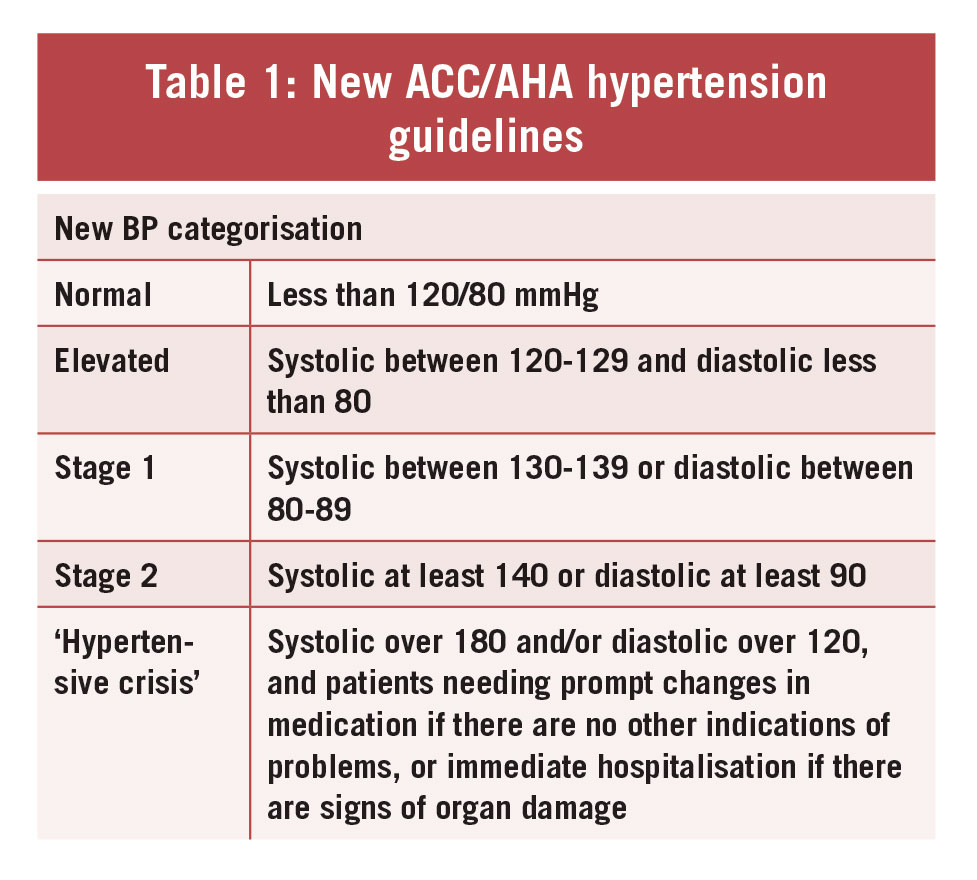
Summarising the main thrust of the guideline changes, the ACC said high blood pressure should be treated earlier with lifestyle changes and in some patients with medication – at 130/80mmHg rather than 140/90 – under the new guidelines (see Tables 1 and 2).
Allowing for earlier intervention
The ACC said the guidelines lowered the definition of hypertension to take account of complications that can occur at lower figures and to allow for earlier intervention. The new thresholds mean that nearly half the US adult population will be classified as having hypertension, with many graduating from what would previously been classed as ‘pre-hypertension’. However, the ACC says only a small increase is expected in the numbers requiring antihypertensive drug treatment.
Greater stroke prevention
The new AHA/ACC US guidelines, published at the recent American Heart Association Scientific Sessions, stress the need for more precise BP diagnoses and greater stroke prevention.
Dr Paul Whelton, lead author of the guidelines said: “If you already have a doubling of (CVD) risk, you need to know about it. It doesn’t mean you need medication, but it’s a yellow light that you need to be lowering your blood pressure, mainly with non-drug approaches.”3
The new guidelines were generally well received in the US, with the commentary highlighting the benefits of the lower thresholds in terms of improving health and reducing mortality. US epidemiologist Dr Paul Muntner said they have the potential to increase hypertension awareness, encourage lifestyle modification and focus antihypertensive medication initiation and intensification in US adults with high CVD risk.3
US physician Dr William Cushman, who was on the writing committee for previous hypertension guidelines, said he believed the new guidelines were strong and evidence-based and would be generally well accepted.
Dr William B White, past president of the American Society of Hypertension, said the new guidelines would greatly improve the precision for diagnosing hypertension and reduce CVD mortality rates.
Some specialists urge caution
But some specialists, particularly in Europe, have urged caution. Dr Bryan Williams, chair of medicine at University College London, said while there is a lot that is good in the guidelines, the key message of getting high-risk patients treated to the lower goal may be lost in endless debates about what to do with the worried well “concerned about their systolic blood pressure of 130mmHg”.
And in a recent article in the European Heart Journal,4 experts from Switzerland and the US, have also urged caution about ‘going so low’ with BP thresholds. Drs Franz Messerli, Stefano Rimoldi and Sripal Bangalore said labelling a person previously designated healthy as having a disease can come at a cost.
They pointed out that the new guidelines would increase by 31 million the number of people in the US designated as hypertensive, pointing to previous studies that highlighted the potential harm caused by creating new worried well, in terms of unnecessary anxiety, perception of poor health and deleterious effects on family life. Messerli et al said the recommendation to uniformly lower BP of all hypertensive patients below 130/80 “had to be considered absurd”.
“We can only hope that despite recent guidelines, physicians will continue to treat patients and not mmHg only.”
The EHJ article also queried why the November 2017 ACC/AHA guidance differed so significantly in terms of thresholds from BP guidelines issued by the American College of Physicians and American Academy of Family Medicine earlier that year. These recommended a higher threshold – 150mmHg for those aged 60 and over, yet were based on the same body of evidence as the more recent ACC/AHA guidance, the authors pointed out.
Current UK NICE guidelines on hypertension5 state that stage one hypertension is defined as clinic blood pressure of 140/90mmHg or higher, and subsequent ambulatory blood pressure monitoring (ABPM) daytime average or home blood pressure monitoring (HBPM) average is 135/85mmHg or higher. NICE defines stage two hypertension as clinic BP of 160/100mmHg or higher, and subsequent ABPM daytime average or HBPM average is 150/95mmHg or higher.
Treatment according to individual circumstances
The argument for treating the patient according to their individual circumstances and not just according to guidelines was highlighted recently in Irish research. Recently, researchers from TCD concluded that the SPRINT trial may have underestimated the risk of falls and syncope as a side-effect of intensive BP-lowering therapy in older people. 6 While SPRINT did show that aggressive BP lowering can reduce all cause mortality in the elderly, treatment targets should be individualised, the TCD team suggested.
Co Wexford GP, Dr John Cox, who has a special interest in hypertension, told Forum that while the ACC/AHA guidelines will lead to a substantial increase in the prevalence of people diagnosed with hypertension, the approach to decision-making for treatment incorporating underlying CVD risk will in effect result in only a small increase in the percentage of adults recommended for antihypertensive medication.
“However, the guideline effectively recommends that a substantial proportion of adults taking antihypertensive medication will need to be treated more intensively,” he added.
Dr Cox said these developments will have an effect on the BP treatment targets in the new version of the NICE guidelines due for publication in August 2019.
References
Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017;Nov13
A Randomized Trial of Intensive versus Standard Blood-Pressure Control (The SPRINT Research Group) N Engl J Med 2015:371:2103-2116.
www.acc.org
European Heart Journal, 09 January 2018. ehx806, https://doi.org/10.1093/eurheartj/ehx806
 (click to enlarge)
(click to enlarge)